
Abstract
The (Spiritual) Self-Assessment Tool Study was designed to test the novel engagement tool’s effectiveness. Providing the (Spiritual) Self-Assessment Tool Study to newly admitted medical patients led to few instances where the tool was completed. Nevertheless, the (Spiritual) Self-Assessment Tool Study patient questionnaire generated significant secondary findings: a third of responding patients consider their hospital care incomplete without their care team having access to (Spiritual) Self-Assessment Tool data. Nursing staff also desire this data, but are unable to access it without the (Spiritual) Self-Assessment Tool or an equivalent source.
Background
There has been a marked increase in the ratio (# patients attended)/(# spiritual care practitioners) at Niagara Health over the past decade. With this increase, it became logistically impossible to integrate spiritual care into traditional patient care teams. The situation warranted a novel and innovative tool to provide patient information exchange concerning spiritual care needs. Our prototype was developed in early 2014.
By that year, spiritual care screening and assessment were recommended to be provided by all American inter-disciplinary palliative care teams (Puchalski et al., 2009). The patient’s existing circle of care would then make needful referral to a certified spiritual care professional. This model was arguably generalizable.
Primary resources for spiritual care screening and history-taking included SPIRITual History (Maugens, 1996), FICA (Puchalski, 2006; Puchalski & Romer, 2000), and the HOPE Questions (Anandarajah & Hight, 2001); as well, there were Kenneth Pargament’s (2007) broadly researched question-sets. These resources guided the patient to identify themselves spiritually or religiously by stating their religion, faith, or beliefs, or, more specifically, their church, synagogue, mosque, temple, or community. Further, spiritual and religious histories elicited the patient’s past and present practice patterns. Some of the tools explored more abstract possibilities such as if the respondent considered themselves religious or spiritual. The limitation across these inquiries was their focus on what is outright religious. They failed to identify the lived dynamics or inner workings of people’s meaning-making (i.e. where and how they locate themselves within their overarching conceptual framework or world view). In addition, the primary resources failed appropriately to attend to the patient’s spiritual distress, which Pargament (2007) had demonstrated to be pivotal.
There was also a need to attend to nuances and tensions. In this sensitive and emotional realm, patients can feel intruded upon, defensive, or even judged. Direct questioning about religion or spirituality can lead to opting out. Miscommunication is also a serious issue due to the use of charged but undefined terms. For example, a person who states “I’m very religious” may, in fact, be ritualistic and/or dogmatic, but have limited awareness or practice of purposeful meaning in life. Alternatively, a person who states “I’m not at all spiritual or religious” may, in fact, be keenly self-aware, sensitive to others, curious, open, and highly reflective … in other words, arguably quite spiritual. (Rethinking is in order concerning screening questions such as “Do you currently have what you would describe as religious or spiritual struggles?” (King et al., 2017)!)
Accordingly, the need existed for a tool that would seek patient behaviors, relationships, thinking, attitudes, and reactions revealing their religious and spiritual reality in practical terms, rather than asking the patient to conceptualize, or define themselves. Furthermore, the authors’ desire was to promote and resource every multidisciplinary team member’s engagement with a given patient’s social supports, thinking and believing, self-care practices, struggles and distress—through which their meaning-making takes place—no matter how religious or irreligious, spiritual or un-spiritual the patient or care-giver might see themselves. The tool that resulted was, and remains (Balboni et al., 2017), a novel pathway alongside and overlapping spiritual and religious screening and history-taking, which pathway the authors have designated “engagement.”
The investigators’ assertion is that an integrated use of a spiritual engagement tool will improve the therapeutic alliance between inter-professional care-providers and the patient, and will lead to improved outcomes in terms of effectiveness, safety, and satisfaction.
Development of the Spiritual Care Engagement Tool and the (Spiritual) Self-Assessment Tool
The initial instrument was the Spiritual Care Engagement Tool (SCET) (Appendix I – see supplemental material). It was designed for use by a physician, nurse, or allied health professional to make a fulsome spiritual review, concurrently provide a basic level of spiritual care, and make purposeful referrals to spiritual care practitioners. Its elements were drawn from primary resources. Spiritual care colleagues provided critical review. A 2014–2015 quality assurance project explored the patient experience of being assessed with the SCET in an emergency room setting. Of 125 patients who consented to reflect on their experience, 89% felt the SCET allowed them to “be understood,” and 81% rated the SCET information as “important” or “essential” in their care.
Educational modules were produced and made available on the hospital’s intranet as a resource for any care-provider to administer the SCET. A 2015 quantitative research study (the “SCET Study” or SCETS), approved by the hospital’s Research Ethics Board (REB), used a longitudinal survey of inter-professional staff trained in the use of the SCET, to discover the impact on (enduring change in) practice. What SCETS found was that only rarely will inter-professional staff members participate; this was not a reliable means to receive system-wide spiritual care assessments.
The next phase of the work was undertaken in the same emergency room. It was reasoned that the desired information could be provided directly by patients if the SCET was redesigned. Through multiple quality improvement (QI) cycles over four months in 2016, a well-functioning (Spiritual) Self-Assessment Tool ((S)SAT) was completed (Appendix II – see supplemental material).
Methods
In November 2016, the (S)SAT was integrated into inpatient care at the test site. The method used included a cover letter inviting patients’ use of the tool and providing them with an option to include the (S)SAT in their medical record, or to utilize it as a private, self-reflection exercise. When admitted patients arrived at their inpatient bed, their primary nurse brought them the cover letter plus the (S)SAT. The nurse later collected the (S)SAT from patients wishing to place this material in their medical record. Patients who lacked capacity or were otherwise unable to participate in the process had their forms maintained in a secure file at the nursing station.
An on-line user’s guide was made available to all inter-professional staff (Appendix III – see supplemental material). Inter-professional care-providers were encouraged to find important connections to their patients through their patients’ (S)SATs. Additionally, when patients revealed spiritual opportunities or struggles and a desire to engage with the care team, the user’s guide was there to flag and guide a referral process.
Evaluating Patient and Staff Impressions of (S)SAT
A quantitative experimental study was designed, with two stages: (a) a consecutive-sampling survey of test and control patient populations exploring the correlation between (S)SAT use and experience of care; and (b) at the patient study’s end, an on-line survey of inter-professional staff, on test versus control units, to explore the impact of (S)SAT data availability on care provision. The study was approved by the hospital’s REB; its monitoring was continuous as institutional REB oversight was “handed up” to the Hamilton Integrated Research Ethics Board (HIREB).
Patients who were nearing discharge and not in isolation on the medical unit of the primary test site were approached by research assistants (RAs) who introduced the study, discerned interest, thereupon fully described the study, obtained signed consent, and administered the patient questionnaire. Questionnaires bore no patient identifying information; they were numbered and thereby linked to a patient list (allowing removal of data should a respondent withdraw consent before data analysis); this list was kept secure and destroyed upon turning to work with the data.
Simultaneously, the RAs used the same approach for near-to-discharge and non-isolation medical patients on a medical unit at a second site (within the same health system) to serve as a case-control group. These patients had not been given the (S)SAT as part of their hospital admission.
After data gathering was completed, inter-professional care-providers on both study units were emailed an information letter inviting them to complete a one-time, on-line care-provider questionnaire. The letter was resent once to increase response rates. Participation confirmed a respondent’s consent.
Questionnaires for both stages of the study were 5-point Likert scale question-sets, the queries directly probing either the patient’s experience of care or the staff’s experience of care provision utilizing information made readily available by the (S)SAT. Both questionnaires were trialed by small test groups whose feedback was used to verify understandings and increase readability; the questionnaires were not otherwise validated.
Results
Participation of patients completing the (S)SAT was low and provided insufficient data to answer the research question or validate the (S)SAT. Based on this finding, discovered midpoint by opening and inspecting the dataset, the study’s first stage was prematurely arrested and the second stage performed. Useful information was drawn from consenting patients and nursing staff who completed the evaluation questionnaires.
Results from Nursing Staff
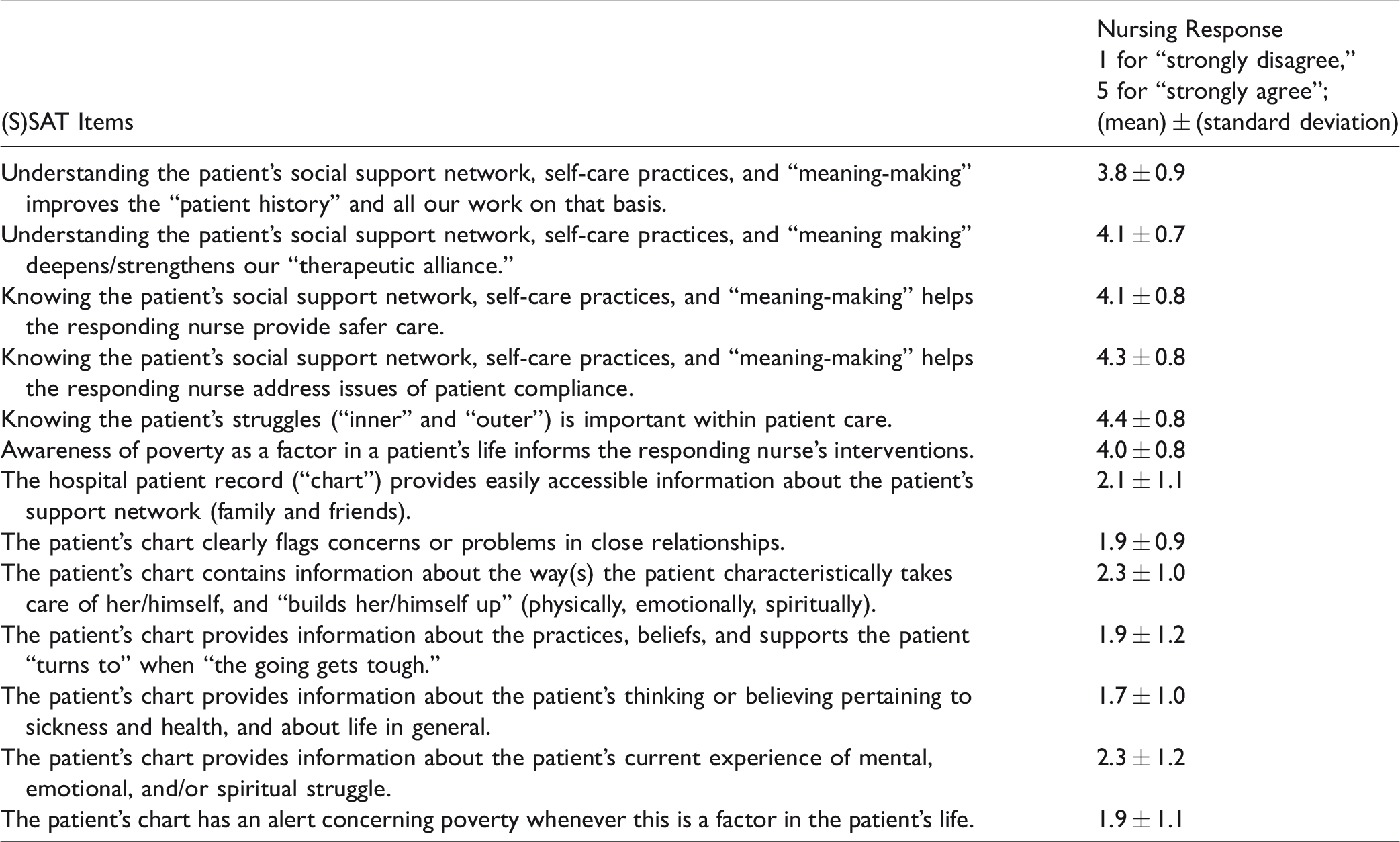
Table 1 shows the degree to which nurses want to know the kind of information revealed by the (S)SAT and the degree to which this information is being provided for them in the hospital’s medical record without a (S)SAT. While the sample size is small (n = 14) and the results not on their own generalizable to the entire professional audience, they do align with findings from the 2014–2015 quality assurance project: professional staff benefit from and desire this patient information.
Nursing staff’s responses concerning their need for the information contained in the (S)SAT, and the degree to which this information is available in a patient’s chart without the (S)SAT (n = 14).
Results from Patients
Data was analyzed separately for the intervention site (where 79 patients were invited and 26 consented to reflect on their experience) and the control site (where 178 patients were invited and 74 consented). Due to the low percentage—only 1 of 26 responders—who actually utilized the (S)SAT, differences between data sets were negligible, so the conglomerate results are presented here.
Thirty percent of patients disagreed or strongly disagreed that their care team understood their views on life. Twenty-one percent disagreed or strongly disagreed that their care team understood “how I view my illness” and/or their beliefs about sickness and health. Of the 21% of the disagreeing respondents, 90% stated that it would have been helpful for their care team to have this understanding.
Twenty-six percent of patients reported that their views on life caused them distress during their hospitalization. Of these responders, 35% disagreed or strongly disagreed that their distress was expressed and addressed as part of their care.
Thirty-one percent of patients reported that their life circumstances caused them distress during their hospitalization. Of these responders, 35% disagreed or strongly disagreed that their distress was expressed and addressed as part of their care.
Twenty-one percent of patients stated that financial stress played a role in their sickness (including impacts on coping strategies). Of these responders, 43% disagreed or strongly disagreed that the care team was aware of their financial distress. In addition, 48% disagreed or strongly disagreed that their care team was useful in helping overcome financial barriers to health.
Thirty-seven percent of the patients reported that it would have helped if their care team understood more about their family and friends. Further, 13% overall disagreed or strongly disagreed that their care team knew about the people in their life who support and/or make things harder for them. Within this 13%, 25% of the responders declared that it would have been helpful for their care teams to understand more about their family and friends.
Seventeen percent of patients disagreed or strongly disagreed that their care team knew about the ways that they take care of themselves and support their well-being. Of these responders, 41% stated that they wished that their care team understood their self-care and coping strategies, such as reading, exercise, and meditation.
Discussion
The most manifest result of the clinical trial is that providing the (S)SAT to newly admitted patients and expecting them to complete the assessment independently is unsuccessful. Secondarily, though, it is verified that there is a significant fraction of patients dissatisfied because their care team did not come to know and act upon information put forward by the (S)SAT. On the receiving end of the data, nursing staff report their desire for this information which is not otherwise clearly located or documented by them in the medical record. (As discovered in the SCETS and the development of the (S)SAT, one barrier for this undocumented information may be that nursing staff are not inclined to add another task to their already significant workload.) Overall, the importance of this spiritual engagement data to both the patient and his/her care team compels a solution.
Limitations
Low uptake of the (S)SAT by newly admitted medical patients (4%) meant the study’s first stage could not demonstrate intended outcomes concerning effectiveness, safety, and satisfaction. Little staff involvement (n = 14 from nursing) yielded only suggestive power from the (S)SATS’s second stage.
First designed in 2014 for engagement in domains of meaning-making between patients and professionals who may or may not see themselves as religious or spiritual, the SCET and thereafter the (S)SAT initiate a differently nuanced pathway amongst spiritual care screening and history-taking tools. More work is obviously needed to validate the SCET and (S)SAT. Required first are means to put “spiritual engagement” material into general use. Without ability to mandate an institution’s use of the SCET, the authors plan to make the (S)SAT generally available to the public both before and during hospitalization. The “before arm” is akin to advance medical directive or organ donation directive. It will be pursued by (S)SAT distribution through faith communities, seniors’ residences, long-term care facilities, family physician offices, and the hospital’s website. Once spiritual engagement material is in greater use, the study of effectiveness, safety, and satisfaction outcomes becomes feasible.
Conclusions
The (S)SATS provided credible evidence (n = 100 across 2 sites) in reproducing and appreciably reinforcing the findings of quality assurance (QA) work on the (S)SATS predecessor, SCETS: a significant proportion of patients want and need this information to be in the hands of their care team. Further, the desire of the nursing staff to have and use this information in their delivery of care is ongoing.
Through this publication, the (S)SAT and SCET are made available for use by any and all inter-professionals wishing spiritual engagement with their patients, and/or to study their use.
Supplemental Material
sj-pdf-1-pcc-10.1177_1542305020949443 - Supplemental material for Testing of a (Spiritual) Self-Assessment Tool ((S)SAT) in a Community Hospital Setting
Supplemental material, sj-pdf-1-pcc-10.1177_1542305020949443 for Testing of a (Spiritual) Self-Assessment Tool ((S)SAT) in a Community Hospital Setting by Robert Bond and N. Shira Brown in Journal of Pastoral Care & Counseling
Footnotes
Acknowledgments
Gratitude must be expressed to spiritual care colleagues in Southwestern Ontario for reviewing and critiquing early versions of the SCET to ensure its breadth of content and to make its language both simple and clear. In particular, thanks to Doug Jones, Niagara Health, and to the chaplains at Hamilton Health Sciences whose feedback was orchestrated by Claire Gosselin. The (S)SATS research assistants were Jacob Potwara, Benson Ompoc, and Sagiri Ikenaga. Thank you to them for their work, and to Fabio Frigolé who did the SCET QA assistant work as a Niagara College student placement.
Let it be noted that critical developmental work on the patient questionnaire (and on the care-provider questionnaire, administered after the patient data-gathering phase) was contributed by Dr Jennifer Tsang and Katie Ross of the Niagara Health Research Mentorship Program. Thank you also to Corrine Davis-Schinkel and Marc Brown for assistance with the writing and editing of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Hamilton-Niagara-Haldimand-Brant LHIN “Emergency Department Quality Enhancement Fund” and by the Canadian Foundation for Spiritual Care. Together these sources sponsored the work of (S)SATS research assistants.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.