
Abstract
Critical questions arise about how contextual factors affect hospital chaplains. We interviewed 23 chaplains in-depth. Hospitals’ religious or other institutional affiliation, geography, and leadership can influence chaplains both explicitly/directly and implicitly/indirectly—for example, in types/amounts of support chaplains receive, scope of chaplains’ roles/activities, amounts/types of chaplains’ interactions, chaplains' views of their roles and freedom to innovate, and patients’, families’ and other providers’ perceptions/expectations regarding spiritual care. These data have critical implications for research, practice, and education.
Keywords
Introduction
In recent years, research has sought to describe and “map” the field of chaplaincy as a whole, but many critical questions remain about how various contextual factors may affect these professionals. Chaplains face challenges, such as feeling marginalized at hospitals (Gomez et al., 2021; Wirpsa et al., 2019). In 2019, 79.5% of hospitals had chaplains (White et al., 2023). In the United States, the presence of chaplaincy services has been associated with hospital location, size and church affiliation, with smaller, rural and investor-owned (rather than not-for-profit) institutions less likely to have chaplaincy services (Cadge et al., 2008). Teaching hospitals and those with oncology and occupational health services and those in the South and Midwest, rather than in the West, were more likely to have chaplains. From 1993 to 2003, church-affiliated hospitals were more likely to discontinue chaplaincy services than to add them, while non-profit institutions were more likely than investor-owned ones to add these services (Cadge et al., 2008). From 2010 to 2019, among hospitals, the presence of chaplaincy services was associated with being non-profit or government-affiliated (vs. for-profit), Joint Commission accredited, urban and a teaching hospital, and having church affiliation, system membership and more Medicare inpatient days (White et al., 2023). Hospitals with more chaplains per 100 inpatients have been found to be more likely to have clinical pastoral education programs, more outpatient ministry, and use fewer volunteer chaplains (VandeCreek et al., 2001). As Cadge (2012) has also described, there are variations across the three kinds of chaplaincy departments—professional (which emphasize board certification), traditional (in which chaplains tend to work alone, rather than as parts of interdisciplinary teams, and to not be board certified), and transitional (between these two models). Physicians in the Midwest are also more likely than those in the Northeast to be satisfied with chaplain services (Fitchett et al., 2009). Among hospital wards, palliative care more likely than others to incorporate chaplains (Jeuland et al., 2017; Massey et al., 2015).
Yet many critical questions emerge about how these and/or other differences may “play out” on the ground—for example, whether other phenomena besides the presence or absence of chaplains may be affected, and if so, what. It is unclear, for instance, whether factors such as hospital affiliation may affect not only the presence or absence of chaplains, but also what these professionals do, how they are organized, and fill and see their roles and how the professionals, patients, and families perceive these spiritual care providers.
Antoine et al. (2021, 2022) interviewed 11 healthcare leaders (e.g., the director of patient relations and chief nursing officer) and 14 chaplain managers, and reported that the healthcare leaders saw chaplains’ value in supporting staff in tragic situations and organizational change, and felt they supported chaplains, despite financial strains on the institution (Antoine et al., 2021, 2022). These institutions varied in how they staffed and integrated spiritual care programs, but saw the value of chaplains in helping staff and patients (through providing quality care, responding to patient and staff needs and having experience in the complex hospital milieu) (Antoine et al., 2022). Antoine et al. (2022) also mentioned several formal structural aspects of relationships within healthcare institutions, as seen by executives and chaplain managers, such as whether institutions collected data on chaplains and what categories of types of work chaplains performed.
But questions remain as to the nature of other informal and implicit aspects of these relationships. In general, in any institution, both formal and informal processes may operate and play key roles (Hunter et al., 2020). Many questions thus surface about the possible ways that various contextual factors may affect chaplains.
It is vital to understand such aspects of pastoral care in order to know how best to make it as effective and beneficial to patients as possible across multiple types and varieties of institutions. Yet, strikingly, scant research has explored these possible critical effects of contexts.
Methods
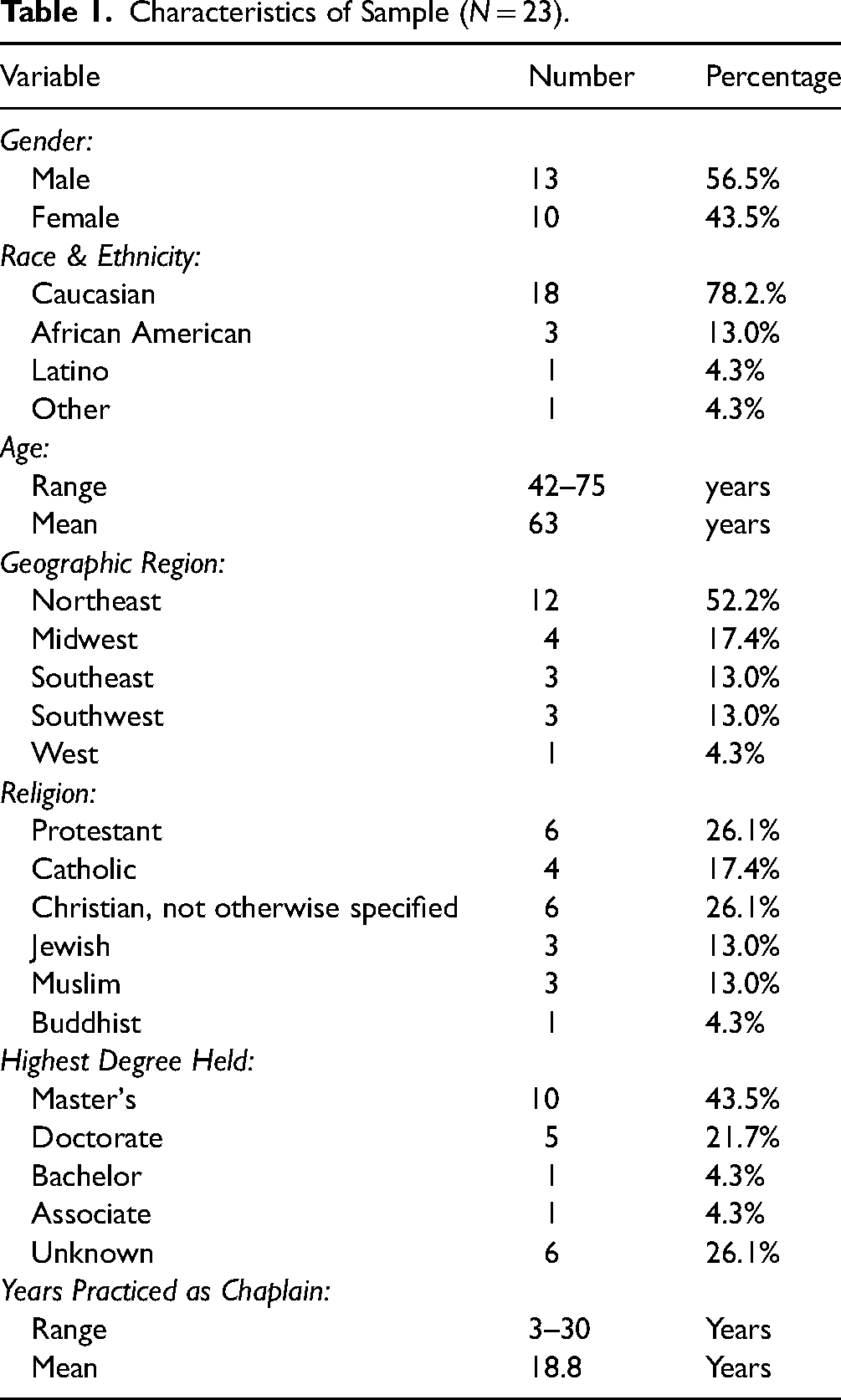
In brief, as described elsewhere (Klitzman et al., 2022, 2022a, 2023), the researchers followed COREQ guidelines (Tong et al., 2007). Telephone interviews were conducted with board-certified chaplains in the United States between 2020 and 2021. The principal investigator (PI), who has extensive experience conducting and analyzing data (Klitzman & Bayer, 2003; Klitzman & Daya, 2005; Klitzman, 2008, 2012, 2015, 2019; Klitzman et al., 2022, 2022a, 2023) conducted the interviews. Twenty-three board-certified chaplains were interviewed for approximately 1 hour each. As seen in Table 1, 13 were men and 10 were women; 78.2.% were Caucasian, 13.0% African American and 4.3% Latino; the mean age was 63 (range 42–72). They were from throughout the U.S., with diverse religions; 43.5% had Masters degrees; 21.7% doctorates; and they had practiced for a mean of 18.8 years (range 3–30). These interviewees worked in various types of hospitals (e.g., Catholic, secular, Veterans Administration [VA]) and had often switched among these types over their training and careers.
Characteristics of Sample (N = 23).
Qualitative methods were chosen because these can best elicit the full range and typologies of attitudes, interactions and practices involved, and can inform subsequent quantitative studies. The methods for the present study adapted key elements from “grounded theory” (Corbin & Strauss, 2008), and were thus informed by techniques of “constant comparison,” with data from different contexts compared for similarities and differences, to see if they suggest hypotheses. This technique generates new analytic categories and questions, and checks them for reasonableness.
From a theoretical standpoint, Geertz (1973) has advocated studying aspects of individuals’ lives, decisions, and social situations not by imposing theoretical structures, but by trying to understand these individuals’ own experiences and perspectives, drawing on their own words to obtain a “thick description.” Such an approach can reveal crucial aspects of social phenomena that qualitative data or other approaches might miss.
Participants
The chaplains were recruited through the listservs of the Association of Professional Chaplains and through word of mouth. Chaplains who were interested in participating contacted the PI by email. Participants were from across the United States. In-depth interviews were conducted until “saturation” was reached (i.e., “the point at which no new information of themes are observed in the data”) (Guest et al., 2006). The Columbia University Department of Psychiatry Institutional Review Board approved the study.
Instruments
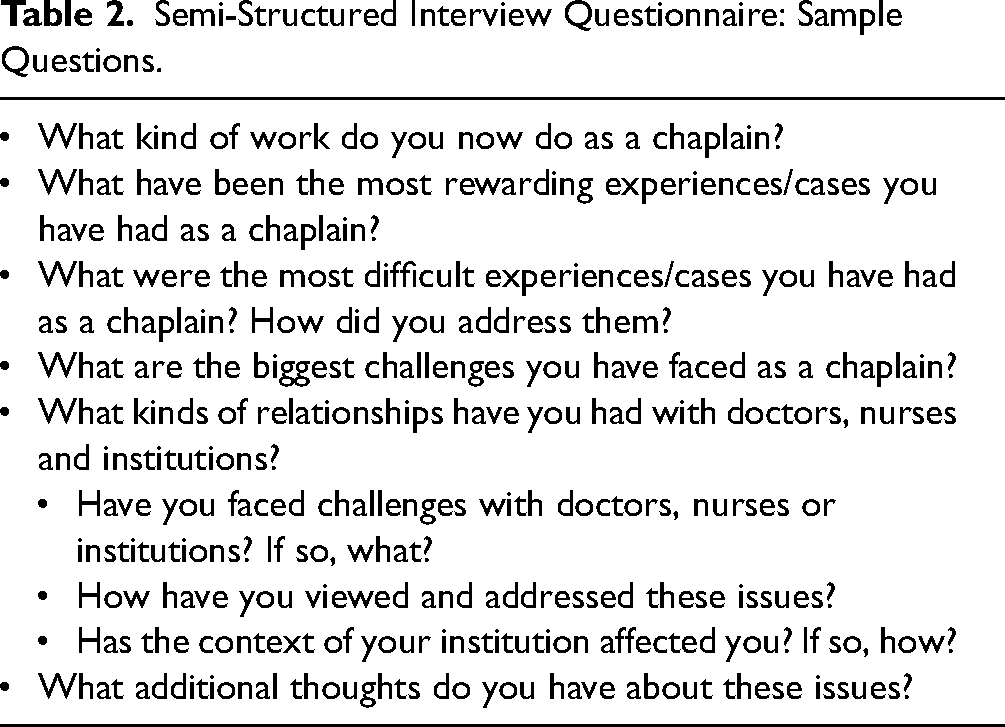
The semi-structured interview questionnaire was drafted, drawing on the prior literature on chaplains. Questions explored chaplains’ views, experiences, and decisions. The PI conducted all the interviews. Sample questions, asked of all participants, appear in Table 2.
Semi-Structured Interview Questionnaire: Sample Questions.
Data Analysis
Interviews were audio-recorded. The PI took field notes after each interview. Transcriptions and initial analyses of interviews occurred during the period in which the interviews were being conducted, helping to shape subsequent interviews. Once the full set of interviews was completed, subsequent analyses were conducted in two phases, primarily by trained research assistants (RAs) and the PI. In phase I, each independently examined a subset of interviews to assess factors that shaped participants’ experiences, identifying categories of recurrent themes and issues that were subsequently given codes. The PI and RAs read each interview, systematically coding blocks of text to assign “core” codes or categories (e.g., different types of institutional contexts and settings in which chaplains worked).
While reading the interviews, a topic name (or code) was inserted beside each excerpt of the interview to indicate the themes being discussed. The PI and RAs then worked together to reconcile these independently developed coding schemes into a single scheme. Next, a coding manual was prepared, defining each code and examining areas of disagreement until reaching consensus. New themes that did not fit into the original coding framework were discussed, and modifications made in the manual, adding themes or sub-dividing existing codes as deemed appropriate.
In phase II of the analysis, the PI and RAs independently content-analyzed the data to identify the principal subcategories and ranges of variation within each of the core codes. They reconciled the sub-themes identified by each coder into a single set of “secondary” codes and an elaborated set of core codes. These codes assessed, for instance, the specific impacts on chaplains of hospital affiliation, geography, and institutional leadership (e.g., chaplains getting assigned to hospital committees, or feeling marginalized or encouraged).
Codes and subcodes were then used in analysis of all of the interviews. To ensure coding reliability, two coders analyzed all interviews. Where necessary, multiple codes were used. Similarities and differences were assessed among participants, examining categories that emerged, ranges of variation within categories, and variables that may be involved. Areas of disagreement were examined through closer analysis until consensus was reached. Consistency and accuracy in ratings was checked regularly by comparing earlier and later coded excerpts. The themes that emerged in the data are illustrated below by excerpts from the interviews. Subcodes included specific types of chaplains’ interactions with hospital patients or their families (e.g., effects of contextual factors on chaplains’ work, activities, and interactions with patients and families).
Results
In brief, as seen in Figure 1 and described more fully below, several types of contextual factors, particularly religious and other organizational affiliation, geographic location, and leaders’ attitudes, can affect chaplaincy both formally and informally. Examples include how chaplains work, interact and see their roles, and how institutions organize chaplaincy departments, whether and how they give chaplains additional roles in institutions (e.g., serving on various administrative committees), and expectations of patients, families, and medical staff.

Institutional and other contextual factors and their effects on chaplains.
Effects of Institutional Contexts
Institutional contexts can affect roles and attitudes concerning chaplains, the organization of chaplaincy departments, and patients’ and families’ expectations.
Effects on Roles and Attitudes Regarding Chaplains
Formal and Informal Effects
Hospitals vary in whether they have larger institutional affiliations, and if so, what type and how these affiliations affect chaplains. Across different institutional contexts, chaplains have both similarities and differences in perceptions, functions and roles. In certain regards, the essential underlying work of chaplains in different types of hospitals is similar, partly since patients themselves face similar challenges across a wide range of religious affiliations and beliefs. As a chaplain who had worked in both a secular and a Catholic institution said, On one level, interacting with patients isn’t different. Your role as a chaplain is to serve that person and their spiritual well-being. They might not be religious, and we work with Muslim, Jewish and non-religious patients, but really, it's the same thing: how do they make sense of what's happening and find the strength to go on? [Chaplain #13]
Yet institutional contexts can shape several key aspects of chaplaincy, including both formal, logistical as well as informal, institutional support and attitudes, such as encouragement and positive feedback. I’ve worked for both faith-based and secular institutions. Doctors at faith-based institutions tend to be a little more sensitive to the mission of the institution…One doctor walked up to me at the nurse's station and said, ‘You know what? Without hope, my patients can’t heal, and you just instilled hope in that patient. I appreciate that.’ That blew me away. I lived off of that compliment for months. [Chaplain #10]
Differences in Administrative Roles Within the Institution
Different institutional contexts can also affect key aspects of chaplaincy departments themselves—such as the roles they fill. For instance, Catholic hospitals may provide more explicitly religious services and rituals, though these may be more Christian than inter-faith. As a chaplain at a Catholic hospital said, They offer daily Mass, do blessing of the hands, and in the context of Mass, honor employees with awards for their values. We take our employee award winners on a free trip to our founding congregation. [Chaplain #13]
Hospitals can vary, too, in the additional roles they give chaplains within institutions, such as serving on various committees. As another chaplain observed, Catholic hospitals have mission leaders, a role in administration, helping to ensure the organization is living its mission, and maintaining a Catholic identity. So, my ‘patients’ include employees. Spiritual care, ethics, and community outreach all report to me. [Chaplain #13]
Institutions vary as well in whether they have chaplains serve on hospital ethics committees and/or perform ethics consults. One chaplain, for instance, “was Chair of our Ethics Committee for many years. I’m still on the Committee” [Chaplain #16]. Inclusion of chaplains on hospital committees may result from varying institutional as well as individual chaplain characteristics, but overall suggest relatively more formal recognition in hospitals of the value of chaplains.
Such wider committee and institutional involvement can aid chaplains, providing intra-institutional relationships on which chaplains can then potentially draw. One chaplain described, for instance, a young pregnant African American woman who had come multiple times for pain management, but was not getting optimal evaluation and care. The staff saw the patient simply as a drug addict. “Luckily, I had a very good connection with a fantastic maternal-fetal specialist. We had worked together on the Ethics Committee” [Chaplain #16].
This chaplain thus called this specialist and had him see the patient. He just blew the medical team away. They were missing a huge medical issue because they kept seeing this patient only as an addict. But we found out she had a kinked bowel, which can come and go, but get stuck…The medical team had not done certain tests. My work as a chaplain is to create a connection, to leverage power and see beyond racism… [Chaplain #16]
Differences in Challenges Chaplains Face
Institutional contexts can also affect the challenges that chaplains encounter and perceive in their work. A chaplain who has only worked at large, secular academic medical centers said, If you’re at a Catholic- or religious-based institution, there's probably a greater appreciation of spiritual care, because it's in the institution's DNA—that it's important. At a more secular place, there's more of an uphill battle. I’ve worked in three large, secular hospital systems, and [the issues] are the same... [Chaplain #21]
Abilities to Innovate
Institutional contexts can also affect the relative freedom chaplains feel they have to innovate and/or start new programs (e.g., new support or discussion groups for patients, family, or staff). A chaplain who has worked at both U.S. Veterans Affairs (VA) and other hospitals, said, I had a little bit of experience in different kinds of hospitals, and I’ve got more freedom at the VA hospital to do what I do than I did in those two other hospitals. Within the VA, one of our roles is to support religious freedom—a veteran's right to practice their religion or to not be around it. We support that, and the right to have that religious service available to them. [Chaplain #9]
Interactions With Staff
Institutional contexts can also affect chaplains’ interactions with staff. Catholic hospitals may, for instance, appreciate staff's spiritual and religious needs more. One such institution gives staff a “work sabbath” once a year, allowing employees to take an extra paid day away every year, if they choose, “where we go to a lake. It's a day about work–life balance. I lead it” [Chaplain #13]. Secular hospitals may offer staff retreats as well, but these may not be as related to spiritual issues per se, however that may be defined.
Effects on Chaplaincy Departments
Types of Chaplains
Larger hospitals and those in urban, rather than rural areas, and thus potentially having more diverse populations, may also be more likely to hire a wider range of chaplains—for example, including Muslim, secular or humanist chaplains. Several hospitals have a Muslim chaplain because they treat a relatively larger number of Muslim patients, who may strongly prefer having a chaplain of their own faith. A Muslim patient was dying at a major hospital, and the hospital sent him a Catholic priest. The Chaplaincy Department marketed themselves as a ‘multi-faith’ organization, but was not, because it left out Islam, Buddhism, Hinduism and others. The Catholic chaplain met him. The patient said, ‘I do not want a Catholic chaplain. I want a Muslim one.’ The priest said, ‘Who would you recommend?’ The patient said his Imam. The Imam was a very elderly man. I was assisting him as an Associate and he asked me if I would visit this patient. So, I did. A couple of weeks later, the head of the hospital's Chaplaincy Department spoke with the Imam, asking if I would be willing to take clinical pastoral education courses. I said yes. [Chaplain #3]
Effects on Chaplains’ Interactions With Each Other
Institutional context can also impact chaplains’ interactions with each other. Hospitals with larger chaplaincy programs may, for instance, allow these professionals to establish and benefit from more mutual support. Chaplains at institutions with fewer colleagues, in some cases even only a single such individual, face added stresses, lacking in-house peer support. Colleagues of mine operate as the sole, individual chaplain in a hospital. I am very sad for them. The burden they carry seems to me insurmountable. Chaplains do things that we can only talk about with other chaplains. We can’t go home to our spouse or families and talk about these things, or do so with people in church who might share our faith. What we expect and are taught from our faith, versus what we experience is jarring. Usually, only another chaplain understands. I feel sad for the patients, families, and staff who are not getting the safe spaces that chaplains can provide. [Chaplain #17]
Effects on Patients’ and Families’ Expectations
Institutional affiliation can shape, too, patients’ and families’ expectations of chaplaincy services. At secular institutions, patients as well as other providers may sense that issues related to religion may be somehow off-limits or taboo, even if these perceptions are incorrect. A chaplain at a secular institution reported, I once prayed with a family. The patient had just been diagnosed with breast cancer. I asked if they would like to have a prayer. Her husband looked at me and asked, ‘Is that allowed?’ I said, ‘Yes, even in this godless university hospital, we’re allowed to pray.’ [Chaplain #17]
At secular hospitals, religious patients may have lower expectations of the availability of religious practices and support. One patient told me, ‘I’m just so surprised I’m getting communion here in the hospital.’ I asked why. He replied, ‘Well, I know that the Catholic hospital across town would have priests and religious people. This is a secular hospital. I just didn’t think it would, and I’m just so pleased with this.’ [Chaplain #17]
Effects Related to Institution's Physical Appearance
Institutional affiliation often shapes hospitals not only directly and explicitly but indirectly and implicitly as well. Such affiliation can influence, for instance, key aspects of a hospital's physical appearance, which can serve as reminders and set a tone, influencing a hospital's ethos and culture. “My training took place in an Adventist hospital, and there were scriptures on the wall and pictures of Jesus on every floor” [Chaplain #17].
Even certain secular hospitals may have explicit trappings of religion. One major hospital was adamant that it was going to be a secular hospital, but when you walk in, there is ten-foot statue of Christ the Consoler. People even with no religion at all always touch the foot. [Chaplain #13]
Effects of Geographic Contexts
Types of Religious Beliefs and Views
Hospitals’ geographic locations can also influence local, and thereby hospital, culture in several ways that can affect chaplains, both directly and indirectly. The cultures of geographic regions can differ, for instance, in the strength and prevalence of particular religious faiths, practices and attitudes among the local population, and thus among patients, family members, doctors, nurses, hospital administrators, other staff, and chaplains themselves. A hospital's geographic location and consequently local culture can therefore affect the institution's culture. As the director of one chaplaincy department said, We’re in the Bible Belt of the South. Sometimes, I think we sit on the buckle! My hospital is reflective of the culture in which we live. I think we chaplains reflect the culture of our administration and our board of directors. I think we are moving in a good direction toward being more inclusive and aware that inclusivity is healthy, but we are very much a product of our environment. [Chaplain #17]
I think it says something that they have hired a woman in this position of chaplaincy department director, which is something wouldn’t even be considered a ‘thing’ on either coast. But here in the middle of the country, it is—there are still people who want to talk to me about being a woman in the ministry. I don’t have time for that conversation. [Chaplain #17]
Chaplains suggested, too, that differences may exist as well across certain geographic areas in how often providers attend religious institutions and/or see patients and other staff there, which can also affect interactions within the hospital.
Still, prevalent religious and cultural attitudes may not extend to everyone within a particular milieu. Chaplains then need to beware of prevalent assumptions regarding gender roles or certain religious or other attitudes that lead to potential discrimination. People here utilize and are familiar with Evangelical Christian language, but have not necessarily thought through the nuances of that language. So, we don’t want to assume that when we say, ‘baptize your baby’ and someone else says, ‘baptize your baby’ those are the same things. We also don’t want to assume that because you are unable to use an Evangelical Christian language that you don’t hold your child's life sacred and want to honor that life before the Creator, whatever Creator you consider. Evangelical language is also used, misused and abused. The Bible is used as authoritative and as club and battering ram. [Chaplain #17]
Effects on Other Staff
Across geographic areas, doctors, too, can vary in their religiosity, affecting the milieu in which chaplains work, and potentially various aspects of chaplaincy. A Southern chaplain reported, A medical student here went to the Northeast for her residency and then came back. I asked her, ‘What was it like up North?’ She said that being up North was ‘extremely difficult’ for her because there was much less attention on spirituality, and the medical community was ‘so secular, kind of anti-religious. Religion was just not a topic of people's regular everyday identity, in a way that is different from here.’ So, she was happy to come back here, where just about everybody seems to have some kind of connection to religion in some way in their regular life. I suspect that that affects chaplaincy. [Chaplain #4]
Attitudes about science, too, can vary across regions, even among physicians. Some religious medical students and doctors remain doctrinaire and in the South even oppose evolution. In a lecture, I once mentioned evolution in passing. An attending in the audience took great offense and challenged me: ‘I think evolution is just a hypothesis. There are other points of view.’ I was shocked…I just said, ‘We can talk more afterwards.’ [Chaplain #1]
Differing Uses and Types of Volunteer Chaplains
Across geographic areas, attitudes among chaplains may vary as well, with hospitals differing as well in the degrees to which they rely on unpaid clergy who might be Evangelicals and take on less open non-denominational approaches. Here in the South, most chaplains come out of a Christian Evangelical background, and consequently see themselves as an advocate for God. A lot of the chaplains are also not board-certified, but are former church pastors. They have a perspective of ‘save ‘em.’ It is subtle, not necessarily brazen. It comes across, for instance, in asking questions about eternal life in a gratuitous way. The circumstances may raise the question. But it's also what they’re used to. Many chaplains getting certified still feel they’re basically there to save the person from eternal damnation, or apocalyptic outcomes. Even though they should be neutral, many chaplains proceed as they would in a church ministry and evangelize, or think the patient needs to be saved to God before they die. That can be offensive. Chaplains don’t explicitly say, ‘I’m here to win ‘em to God.’ But I get that sense. If a patient says, ‘I don’t know if the doctors are really telling me how serious this is.’ The chaplain might say, ‘That brings up the issue of where we’re going after we pass away in this life. Let me ask you, where do you think your soul is going to be when you pass away?’ The chaplain is bringing up that issue. That's not what the patient was asking, but the chaplain turned it into an evangelistic question. Hospitalized patients do not want that. They want someone to empathize with their suffering and maybe relate to their religious tradition, but not necessarily create a situation where they’re concerned about what happens if they die. That's a key reason not to use volunteers as chaplains. They tend to be highly evangelical and have their own agenda. The more professional the chaplain, the less likely that happens. Board certified chaplains in the Northeast are less likely to do that and to just scare the life out of Mrs. Jones.’ [Chaplain #10]
Cultural Norms
Cultural norms concerning respect, politeness and approaches toward different kinds of authority and others can also differ across geographic locations in the United States in ways that can influence both chaplains and patients. More than words, the tone in which you enter the room can change everything. The facial expressions, body language of the patients and the lighting of the room are all key elements in gauging the existing tone of the room, especially because people in the South are too polite to request a chaplain to leave, even when they don’t want them. [Chaplain #11]
Differing Legal Issues
In the United States, states also vary in laws and policies that can affect key aspects of healthcare, including Medicare and Medicaid coverage for palliative care, hospice and other services, and hence the amount, type and other characteristics of chaplains within an institution. In our state, we’re trying to get a palliative care pilot with Medicaid that would cover the whole team, because we feel strongly that the chaplain and social worker need to be on the team. [Chaplain #13]
Effects of Institutional Leaders
Hospital leadership can vary as well in ways that influence both institutional contexts and chaplains. Leaders can reflect and/or try to alter key aspects of institutional cultures, as well as the amounts and types of encouragement and financial support spiritual care departments receive, and how much chaplains feel comfortable attempting to develop new programs or initiatives. Chaplains’ perspectives of the contexts and constraints in which they work can affect their sense of the amounts of freedom they have to develop their own creative ways of integrating spirituality into hospitals. As a community hospital chaplain reported, In our secular hospital, the prior CEO gave me a free hand to do whatever I wanted. So, there's a lot of religion going on. We do prayers over the loudspeaker, blessings for our staff members and of nurses’ hands, and in October, the blessing of the animals for St. Francis of Assisi. On July Fourth we do a blessing for the military and our country. The local high school's uniformed Junior ROTC posts the colors. We distribute Christmas and Hanukah cards. Our chapel has Bibles, Qur’ans, the Torah, rosary beads, prayer cards, pamphlets and spiritual readings. We give communion. We ask patients, ‘Do you want us to call your pastor or rabbi and see if they’ll come in and give you a blessing?’ [Chaplain #2]
Hospital leaders may vary in their support of chaplains’ activities, but also shift over time, rather than remain fixed. One chaplain tried to establish an informal support group for ICU nurses, but the nursing director resisted, arguing that the nurses should instead just persevere. The nursing director said, ‘The nurses don’t need that. We just tell them, ‘Suck it up. This is how it is.’ I said, ‘Would you mind if I tried? I’d like for you to attend as well.’ [Chaplain #21]
We did a session, and new nurses broke down sobbing, saying, ‘This is the first death I’ve ever experienced in my life. No one I know has ever died. Other nurses just tell me: Just suck it up. This is how it is.’ They were just in real distress. Luckily, the nursing manager heard that, and told me to schedule more sessions for the nurses. She could see that it was important to them. [Chaplain #21]
Individual institutional leaders can thus vary and reflect their institutional and geographic location, but also differ in whether and to what degree they do so.
Discussion
These data suggest how several contextual factors can affect critical aspects of chaplaincy. Specifically, variations in religious or other institutional affiliation, geography and leadership can affect each other and chaplains, patients and other providers, both explicitly and implicitly and directly and indirectly. Institutional factors can influence not only the presence or absence of chaplains, but attitudes and roles regarding chaplains, including the scope of chaplains’ roles and activities and their views of these roles. These factors can influence, too, the organization of chaplaincy departments, including the types of chaplains, the range and diversity of faiths represented in the chaplaincy department and their availability, the types and amounts of support chaplaincy receive, the degrees of interactions among chaplains (with fewer chaplains allowing for less mutual support and “strength in numbers”), and the roles they may play within the institution (e.g., serving on various committees). These effects can influence not only chaplaincy departments but also, indirectly, chaplains’ work and sense of purpose and support. These institutional factors can mold, too, patients’, families’ and other providers’ perceptions and expectations regarding spiritual care that can, in turn, affect chaplains and the latters’ work. Geographic location can affect the prevalent beliefs and practices of providers and the importance of religion to them. Specific leadership at multiple institutional levels can influence the relative freedom chaplains feel they have to innovate and pursue activities that they sense are important. While prior quantitative research has indicated that larger, non-rural, not-for-profit, Southern and Midwestern hospitals were more likely to have chaplaincy services (Cadge et al., 2008), and that chaplaincy departments vary in the importance and degrees of board certification (Cadge, 2012), the present study suggests that additional contextual factors and their effects, specific institutional affiliation and leadership, and broader geographic and cultural contexts of the surrounding community itself can influence not only the presence or absence of chaplains, but also informal characteristics of interactions between providers, patients and chaplains.
These data have critical implications for future practice, policy, education of multiple stakeholders and research. While White et al. (2023) and Cadge et al. (2008) examined factors that may be involved in whether chaplains exist in a hospital or not, the current data suggest that contextual factors also affect what activities chaplains might engage in, with what encouragement, challenges, and abilities to innovate, what types of chaplains might exist, what relationships they may have with other staff, and what other aspects of religious views among patients and staff may exist. The current data suggest, for instance, how individual hospital leaders can shape also institutional culture and context, which can affect chaplaincy departments and chaplain's experiences, beyond characteristics such as the institutions’ religious affiliation and whether the department is professional, traditional or transitional. Broader prevalent community attitudes concerning religion and spirituality can also infuse and influence the culture of a hospital and both formal and informal interactions. Geography, too, can influence the range and diversity of religions among patients and chaplains, including the number of patients who are not Christian, but are Muslim, Hindu, or spiritual but not religious.
The present data highlight how patients’ and families’ perceptions of contextual differences may also affect these individuals’ expectations concerning chaplaincy and potentially requests for different kinds of religious and spiritual activities (e.g., prayer or communion), ways they view and feel able or encouraged to draw on religion and spirituality for support, and thus their interactions with chaplains. Families and patients in secular, as opposed to religiously-affiliated hospitals, might not expect, and therefore not know, to request chaplaincy services.
Differences in geographical locations can influence local culture and norms and the prevalence of certain religious views, practices, and faiths, in ways that can affect both hospitals and chaplains. Other data suggest that geographic regions vary in the roles and importance of religion and the distribution of different faiths. Specifically, more people say they are “very religious” in the Southwest and Southeast than in New England and the Rockies (45% and 43%, vs. only 26%, respectively). So-called “Nones” (who indicate “None of the above,” when asked about their religion) account for 28% of the West and 25% of the Northeast, but only 19% of the South. About half of Evangelicals (49%) live in the South (Norman, 2018). Similarly, Cadge et al. (2008) found that Southern and Midwestern hospitals were more likely to have Evangelical services.
These findings support those of Antoine et al. (2021, 2022), suggesting that hospital leaders vary in how they staff and integrate chaplaincy departments. However, while these researchers found that the 11 hospital leaders surveyed appeared to see chaplains in positive ways (Antoine et al., 2021, 2022), the current data suggest that challenges can also arise in these relationships, and that hospital leaders may not always be wholly and optimally supportive, but may at times be less than fully supportive, and can be affected by various contextual factors. These data suggest, too, how VA hospitals, for instance, may support chaplains relatively more than many other secular institutions, due to federal policy mandates.
These findings also underscore the complex relationships between religion and hospitals—the fact that secular hospitals may accept and incorporate spirituality in varying ways that get shaped and negotiated at different institutional levels (from hospital-wide to individual wards) by various chaplains, staff, administrators, and patients.
These insights highlight, too, needs to enhance awareness of these issues among patients, families, chaplains, hospital administrators and others, given, for example, that some patients and families at secular hospitals appear to have limited knowledge and expectations concerning chaplaincy services. Indeed, chaplains see only a minority of patients and families in hospitals (e.g., 5.6% of patients seen in one study (Marin et al., 2015) and 26.5% in another (Damen et al., 2019). Chaplains and institutions should more fully educate these groups, and providers and the public at large, about the availability and scope of such services.
This study underscores, too, needs for chaplains to further educate a wide range of leaders at multiple levels within an institution about potential roles of pastoral care and the benefits of supporting innovation. Secular institutions could also potentially adopt, and benefit from, some of the expanded roles and activities of chaplains at religiously-affiliated institutions, such as holding day-long retreats, and including chaplains on ethics and other committees.
These data suggest as well a vital research agenda—to investigate, among larger samples, the effects of contextual factors on chaplains’, patients’, families’, medical providers’, administrators’ and the public's perceptions, expectations, knowledge, attitudes and practices—for example, types of chaplains’ support, roles and abilities to develop new programs, inclusion on ethics and other hospital committees, factors that may be involved in leaders’ relative support for chaplaincy, such as aspects of these leaders’ professional and personal backgrounds (e.g., age, discipline, particular type of training, and religious beliefs and practices). Future studies can examine, among larger samples, rates in different hospitals of the presence of chaplains on various hospital committees, and what types of committees, and associations with other institutional characteristics, and how chaplains perceive the types, degrees and implications of institutional support and freedom they have to innovate. The present data underscore as well needs to study more fully how patients and families in various contexts perceive and seek chaplaincy services—for example, how patients view the availability and potential benefits of chaplains in varying institutions and what other variables may be involved. Such research and attention to these issues can enhance chaplains’ roles and positions and the benefits they can provide.
These data have several potential limitations. The study included 23 chaplains, which is a sufficient number for qualitative research and analyses. However, future studies with larger samples can further illuminate these issues and factors that may be involved. Of the respondents, 52.2% were from outside the Northwest. Yet these data are nonetheless suggestive of geographic differences among regions and reveal needs for further research that recruits much larger samples from multiple regions to examine these issues regarding geographical diversity further. The study included only chaplains who are certified through the Association of Professional Chaplains, a leading organization that certifies chaplains. However, future research can explore these issues among non-certified chaplains and volunteers as well.
In short, this paper, the first to explore how various contextual factors affect several key aspects of chaplains’ work and interactions, has critical implications for future research, institutional and chaplaincy practice, and education of chaplains, other providers, administrators, patients and families.
Footnotes
Acknowledgements
The authors would like to thank Beverly Gu, Amanda Shen, Gabriella Smith and especially Patricia Contino for their assistance with the preparation of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.