
Abstract
Mental health care that is open to patients’ existential needs requires well-trained professionals who work in teams and use an open conceptualization of spirituality, religion and other meaning-making domains. Using a mixed methods approach, this article explores how professionals (n = 262) in secular Norway perceive obstacles and opportunities in existential care. The results show correlations between age group, personal religiosity, terminology and perceived expertise. Commitment is high, but collaboration with chaplains and team training are neglected.
Background
In increasingly diverse societies, the need for cultural sensitivity in health care is also increasing, including the need for knowledge and skills to answer patients’ diverse existential needs. While existential questions in human life may, by definition, be somewhat universal, the way people try to answer them is highly individual and dependent on different societal and cultural factors (Austad et al., 2020; Eckersley, 2007; Hvidt et al., 2022). Religion and spirituality are part of many people's resources when meeting existential challenges such as severe or chronic illness or psychological crises. Health care professionals, however, being just as diverse as their patients, are likely not to share the same religious tradition or worldview. Therefore, good existential care must comprise a framework of knowledge and skills and an open attitude towards religious and spiritual diversity. Both professional training and work conditions, including interdisciplinary cooperation, should enable this openness.
Norway, as part of the Western sphere, is, together with Denmark and Sweden, regarded as one of the most secular societies in the world (Lundby & Repstad, 2018). The political and healthcare systems are meant to be based on science and human rights, not influenced by other factors like religion. But contrary to what some experts thought, religion and spirituality have not disappeared from influence. Research by Furseth et al. (2019) found that even as people in northern countries become less religious individually, religion is still a hot topic in the media, and there is more recognition of different beliefs. Repstad (2020) warns that this mix of beliefs does not automatically make people more accepting of each other. In fact, he suggests that it could lead to more conflict because people see the world so differently. When it comes to health, this mix of beliefs can cause disagreements on what sickness is and what we expect from healthcare. The Norwegian government has chosen to openly welcome all kinds of worldviews, as opposed to not favoring any (Stålsett, 2021). This openness can be seen in how Norway's healthcare system operates, making sure to consider all sorts of beliefs, for instance, when they are treating patients with mental health issues like psychosis (Helsedirektoratet, 2013).
The healthcare system should, as such, acknowledge and accommodate patients’ spiritual and cultural needs in providing care. Yet, the extent to which these guidelines are put into practice is highly unknown and needs to be examined. Moreover, there is an continuous debate on the best ways to deliver effective care that addresses the deeper existential concerns and well-being of patients (Frøkedal et al., 2019; Gulbrandsen et al., 2016; Nissen & Andersen, 2022).
Recent studies in Scandinavia and Western Europe on obstacles and potentials of spiritual care have pointed out various relevant aspects, some of which will be highlighted in the following.
In Germany, the work by Frick et al. (2021) brought to light the complex landscape of spiritual competence within healthcare. Through a comprehensive exploratory study involving a survey of 674 health professionals, they revealed a paradoxical stance: While there is a general desire to address the spiritual needs of patients, many professionals expressed a lack of confidence in their ability to engage with spiritual topics effectively. A notable distinction emerged in their findings – older health professionals and those with more religious beliefs felt more adept and responsible for providing spiritual care. From this, it appears that spiritual care competence is often viewed as inherent to the individual rather than as a professional skill set. The study also pointed to practical barriers such as time constraints and lack of suitable spaces, with interdisciplinary collaboration, such as working with chaplains, not commonly practiced.
Echoing the German findings, our studies of Norwegian psychotherapists revealed a similar pattern of limited existential competence, which they connected to a notable absence of relevant training in university curricula (Mandelkow et al., 2022; Mandelkow & Reme, 2022). However, a comprehensive assessment focusing on the challenges and opportunities for delivering existential care within the Norwegian context remains to be undertaken.
In Denmark, Hvidt and Hvidt (2019) and la Cour and Hvidt (2010) have delved into how spirituality and religion intersect with secular healthcare. A vital contribution by Hvidt et al. (2022) involves their analysis of different conceptualizations of spirituality, religion and other meaning-making domains. They argue that “the existential” is a particularly encompassing term, integrating spiritual, religious, and secular aspects, especially relevant within the Western European healthcare setting. Their work also corroborated the link between age and religiosity. As for Norwegian mental healthcare, a question arises regarding the impact of terminology since various phrases like “existential and spiritual needs” (Koslander et al., 2009), “spiritual concerns” (Cone & Giske, 2022), “spirituality” (Holmberg et al., 2017) and “existential information” (Ulland & DeMarinis, 2014) are interchangeably used. It is yet to be determined if this diverse vocabulary reflects a broader spectrum of interpretations or a lack of consensus, calling for more precise research within this context.
In spiritual care, interdisciplinary teamwork is the gold standard (Best et al., 2020). Integrating patients’ existential concerns, previously viewed as chaplains’ domain, is now increasingly recognized as a shared responsibility among healthcare professionals. Post-secular negotiation is an example of a communication approach that can facilitate professional discourse on existential matters, including religious and spiritual concerns, without compromising the ethical standards of a secular healthcare system (Nissen & Andersen, 2022). Chaplains in Nordic countries, mostly church-affiliated, rarely use traditional religious practices such as prayer, scripture reading, or blessing (Thomsen et al., 2019). Their contribution to health care might be best described as the provision of existential care. Therefore, if healthcare professionals, in general, are supposed to become experts in existential care (Danbolt & Stifoss-Hanssen, 2020), would this render chaplains superfluous? To approach this question with regard to Norwegian mental health care, it is essential first to examine the current level of general competence within the system. Additionally, identifying any unique aspects of chaplaincy within the Norwegian mental healthcare system may provide further insight into the potential benefits and challenges of integrating spiritual care into mental healthcare services.
Research Questions
Considering the above factors for fostering or inhibiting spiritual competence in a secular society, issues of terminology and conceptualization as well as the gold standard of teamwork, the main research question of this study is: What is the current state of existential care competence in Norwegian mental health care, including obstacles, potentials, conceptualization influence, and interdisciplinary teamwork? This question can be addressed through several subordinate questions:
How do healthcare professionals perceive their competence in managing existential topics? Which obstacles do healthcare professionals report in addressing religious, spiritual, and existential questions in therapy? Do healthcare professionals’ reported competencies and perceived obstacles differ based on their profession, level of religiousness, and age? Does preference differ for certain terminology (e.g., religious vs. existential)? What role does interdisciplinary teamwork have in this context, especially with hospital chaplains?
Method
To address the different aspects of the research question, a cross-sectional study was conducted in three Norwegian clinics for mental health care.
Sample and Instrument
All clinics are located in southern Norway and have some connection to religion and spirituality, either because they are located in a part of the country that has an especially religious tradition (Sørlandet Sykehus, (Repstad, 2009)) or because they have a religious founding history (Modum Bad and Diakonhjemmet). At the same time, all clinics are part of the secular health care system. By choosing this sampling, we wanted to ensure a statistically sufficient number of religious participants to be able to compare groups. A Norwegian version of the Spiritual Care Competence Questionnaire (SCCQ), the same instrument used by Frick et al. in the German study on obstacles and possibilities, was given to all staff with patient contact. Using the same instrument allowed for a direct comparison of studies. Furthermore, the instrument has shown good validation results (Frick et al., 2019) and covers a broad scope of relevant aspects. The survey consists of 41 Likert scale items, two free text answers and a small number of questions on demographics, including profession, age, and personal religiosity. A factor analysis also confirmed for the Norwegian version (Mandelkow, 2023), resulted in seven factors and seven items concerning obstacles to spiritual care.
Ethics and Procedure
The data were collected in 2019. After providing a general introduction of the project to the clinic management, standardized questionnaires were distributed on the wards in paper format.
To ensure a comprehensive understanding of the items related to “spiritual” or “religious” topics, the survey was presented as including spiritual, religious, and existential elements, and corresponding definitions of these terms were provided.
The study was approved by the Norwegian Centre for Research Data (approval number 61076). Individual informed consent was obtained by signing paper-based information distributed with the survey.
Analysis
Descriptive statistics were used and compared to the German study to address the explorative research questions (1, 2, and 5). For question 5, the SCCQ factor “team spirit” and item 41 on contact with appropriate counselors were especially analyzed. Additionally, a thematic analysis of the free-text answers was conducted. Research question 3 was addressed by using a series of MANOVAs for the independent variables profession (physician/nurse/psychologist), religiousness (believing/non-believing), and age (3 age groups). Following the reflections of Hvidt et al. (2022), possible terminological differences (religious v. existential, question 4) were analyzed using a t-test of the mean differences of two items that are identical apart from the words “religious” and “existential”. For this purpose, the difference between the items was computed as a new variable. The new variable captures, as such, the difference between the responses to the two items. It quantifies the extent of variation or discrepancy between their attitudes, beliefs, or perceptions related to the concepts of «religious» and «existential». This allows for a more detailed investigation of terminological differences, as questioned in research question 4. The thematic analysis was also used to answer this question and question 5. SPSS 29.0 was used to conduct all statistical analyses.
Results
Sample
Two hundred sixty-two mental health care workers participated in this survey (Table 1). Two-thirds were from the largest institution, Sørlandet Sykehus; 69% were female; 61% were protestant; age ranged from 23 to 68 years, with a mean of 44 years (SD = 11.6); and 36% were psychologists (n = 92). Psychologists were marginally younger (M = 40, SD = 10.2) than the other professions (p < .001). In order to obtain clean group data for the comparisons, 78 participants who belonged to “other” professions were excluded from this analysis, leaving 178 physicians, nurses, and psychologists.
Sample characteristics for the three participating institutions (n = 262).
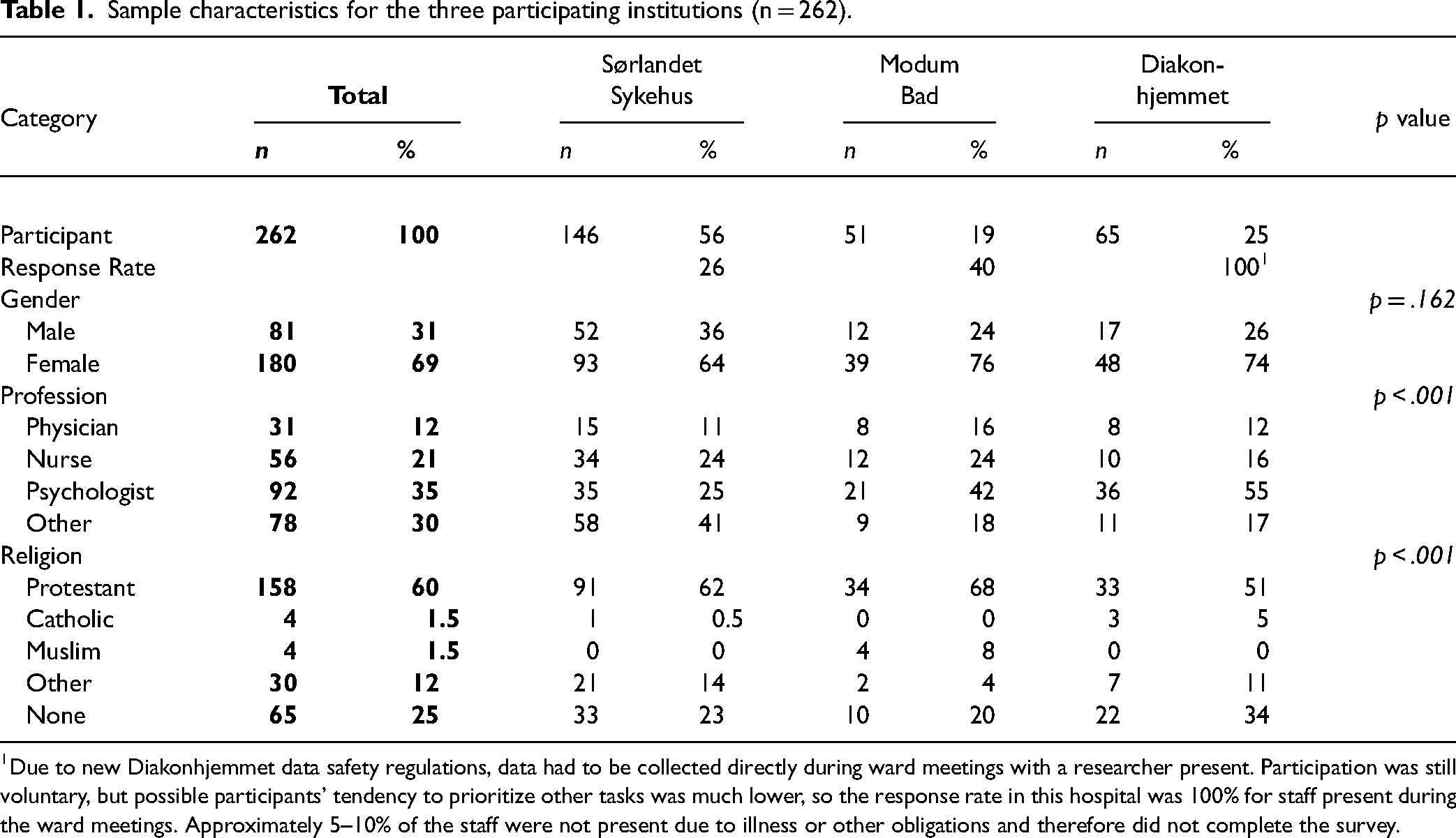
Due to new Diakonhjemmet data safety regulations, data had to be collected directly during ward meetings with a researcher present. Participation was still voluntary, but possible participants’ tendency to prioritize other tasks was much lower, so the response rate in this hospital was 100% for staff present during the ward meetings. Approximately 5–10% of the staff were not present due to illness or other obligations and therefore did not complete the survey.
Competence Factors
Healthcare professionals across the professions show a close to equal distribution of mean scores in the different spiritual care competence factors. The factors themselves, however, show quite different means (Figure 1). With a range of 0–3, the factors team-spirit, documentation, and self-awareness score under 1,5, thus not reaching 50% of possible scores, the factors perception, knowledge, and empowerment range around the middle, only communication is slightly higher with means around 2,3.
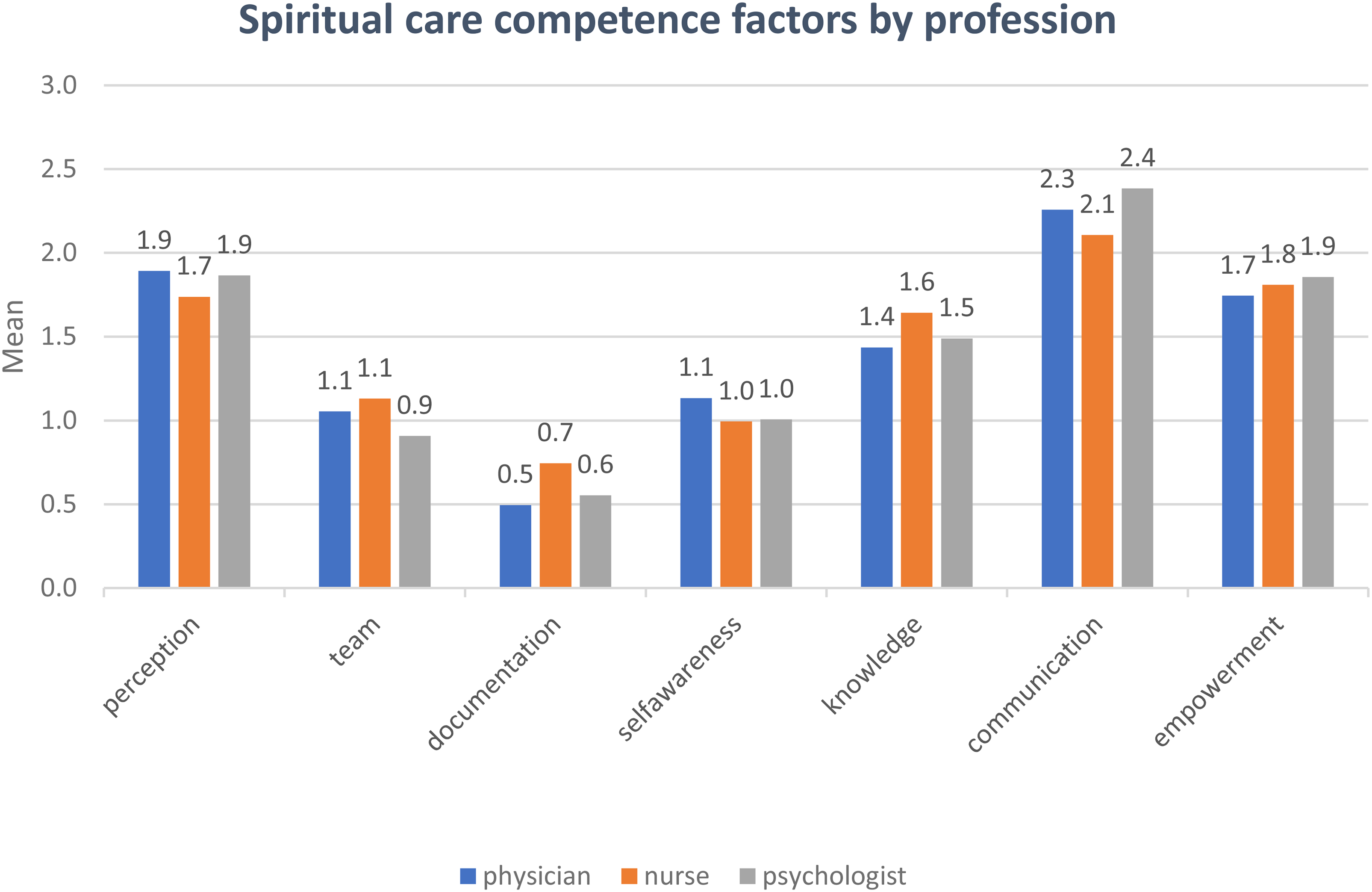
Means of Spiritual Care Competence Factors, Whole Sample, Divided by Profession (n = 178).
Test of Assumptions for MANOVA Calculations
There were no outliers in the data. No multivariate outliers were found, as assessed by the Mahalanobis distance (p > .001). The error variances were homogeneous for all the variables (p > .05), as assessed by Levene's test. There was homogeneity of covariances, as assessed by Box's test (p > .001). Because of the large sample size and MANOVA's robustness, we decided to accept weaknesses in the normal distribution of the data, as assessed by the Shapiro-Wilk test.
Professional Groups and Existential Competence
A one-way MANOVA (results not displayed) analyzing the relationship between the variable “profession” and the seven factors did not show significant differences, the only exception being the factor communication, where psychologists rated higher than nurses p = .012 (MDiff = −.28, 95%-CI[.05, .50]).
Religiosity and Existential Competence
A one-way MANOVA showed a statistically significant difference between the professionals’ religiosity, displayed dichotomously as “rather believing” vs. “rather doubtful” on the combined dependent variables, the seven competence factors, F(7, 169) = 5.306, p < .001, partial η² = .180, Wilk's Λ = .220.
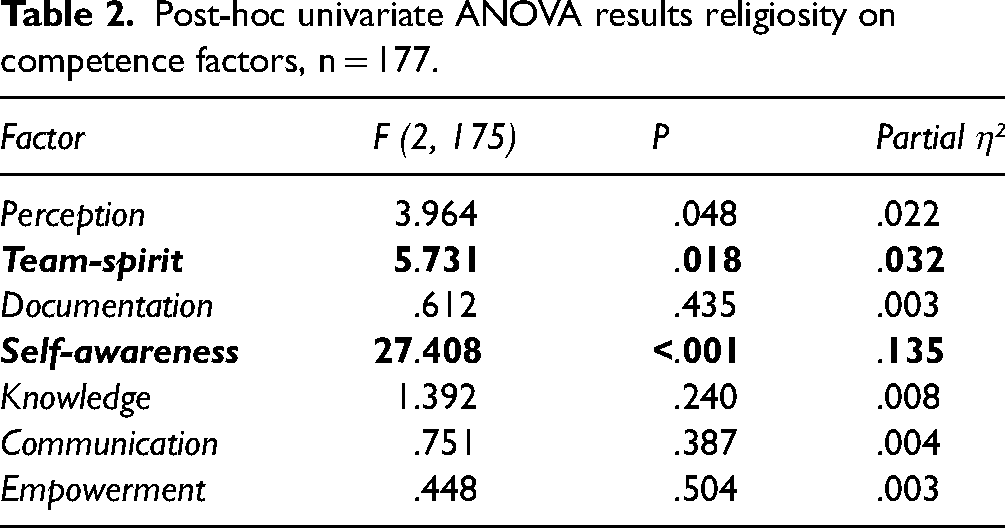
Post-hoc univariate ANOVAs were conducted for every dependent variable. Results show a statistically significant difference between believers and non-believers for the factors team-spirit, F(1, 175) = 5.731, p = .018, partial η² = .032 and self-awareness, F(1, 175) = 27.408, p < .001, partial η² = .135, but not for the other factors (results in Table 2). Throughout the data, believers rate their competence higher than non-believers.
Post-hoc univariate ANOVA results religiosity on competence factors, n = 177.
Age and Existential Competence
A one-way MANOVA showed a statistically significant difference between three age groups: under 40, between 40 and 50, and over 50 on the combined dependent variables, the 7 competence factors: F(14, 338) = 2.334, p = .004, partial η² = .180, Wilk's Λ = .088.
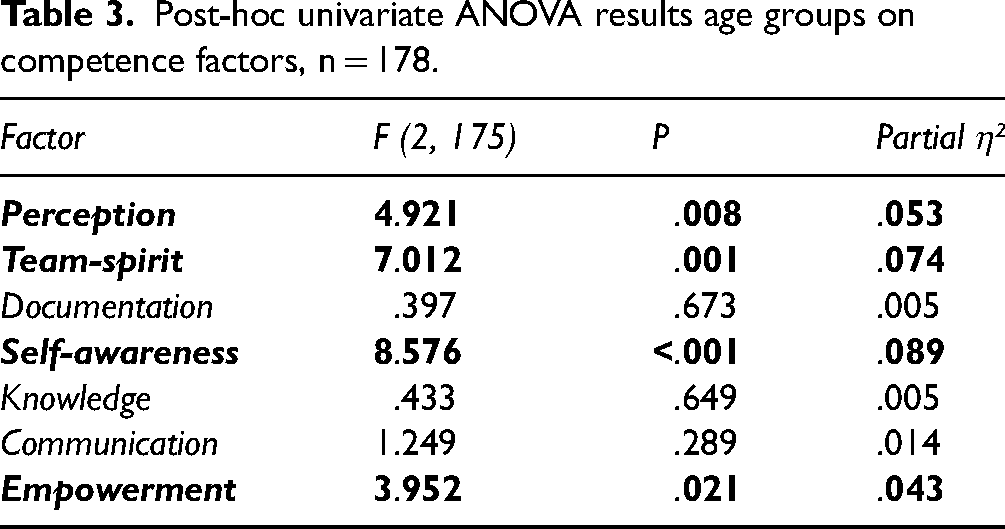
Post-hoc univariate ANOVAs were conducted for every dependent variable. Results show a statistically significant difference between the age groups for the factors perception, F(2, 175) = 4.921, p = .008, partial η² = .053, team-spirit, F(2, 175) = 7.012, p = .001, partial η² = .074, self-awareness, F(2, 175) = 8.576, p < .001, partial η² = .089, and empowerment, F(2, 175) = 3.952, p = .021, partial η² = .043, but not for the other factors (results in Table 3). Throughout the data, older staff rate their existential competence higher than the younger.
Post-hoc univariate ANOVA results age groups on competence factors, n = 178.
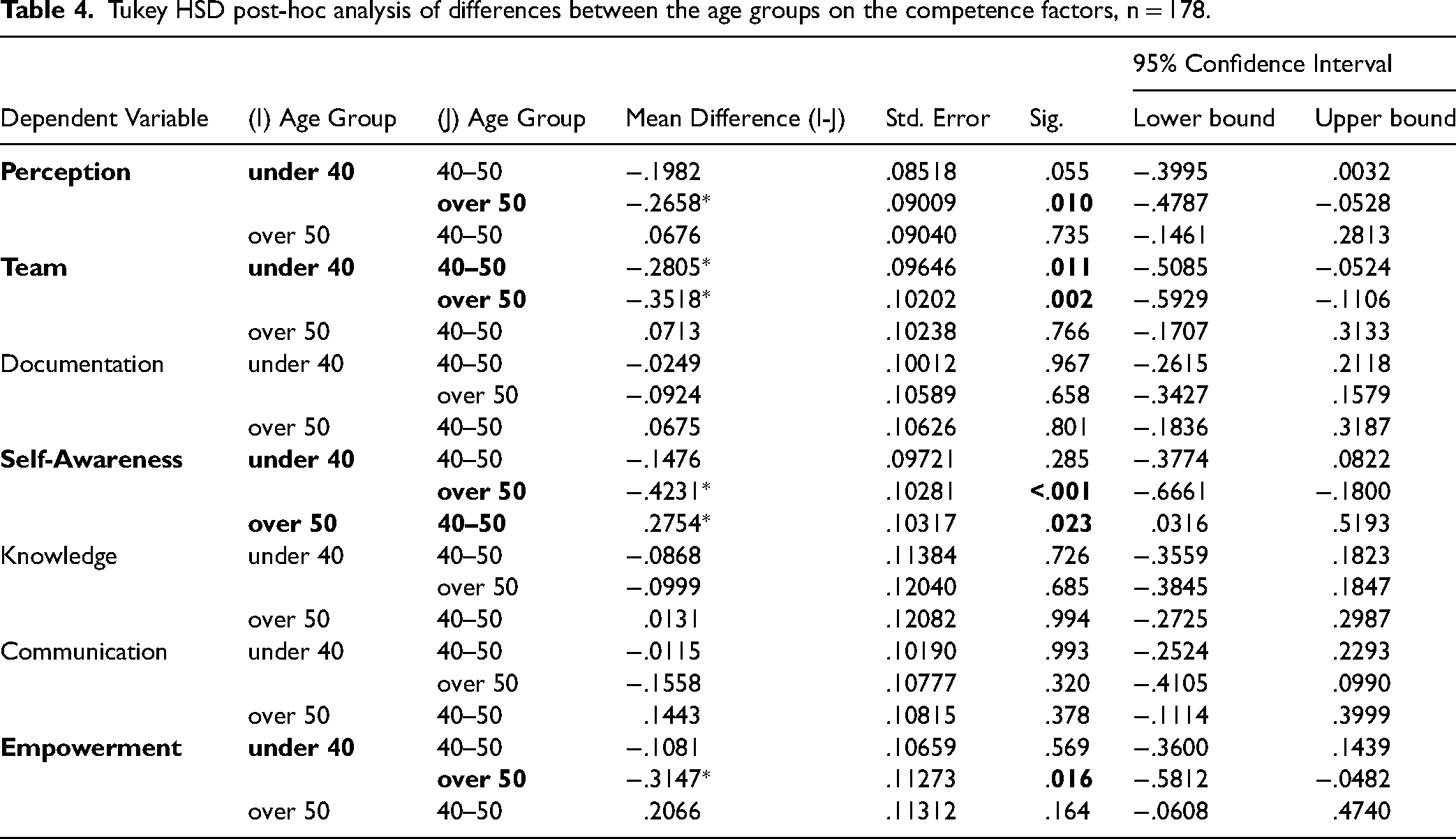
A Tukey HSD post-hoc analysis on the factors perception, team-spirit, self-awareness, and empowerment revealed significant differences between the age groups, as displayed in Table 4—the professionals over 50 scored significantly higher on these factors.
Tukey HSD post-hoc analysis of differences between the age groups on the competence factors, n = 178.
Obstacles
The obstacles to addressing religious, spiritual or existential issues in therapy are operationalized by the following seven items (abbreviations in bold letters):
I feel I would like My I do not perceive myself as an I I think that my
Overall, the participants reported few obstacles (Figure 2). Almost nobody agreed with the statement that it was uncomfortable to talk about spiritual issues, and the highest score was found on the item “I would like to have more time”. Some agreement can be seen on the items that address time, knowledge about religion and being the appropriate person for religious/ spiritual subjects. At the same time, the knowledge about possible counselors, for example, hospital chaplains, was rather low; 75% answered negatively to the corresponding item (Figure 3).
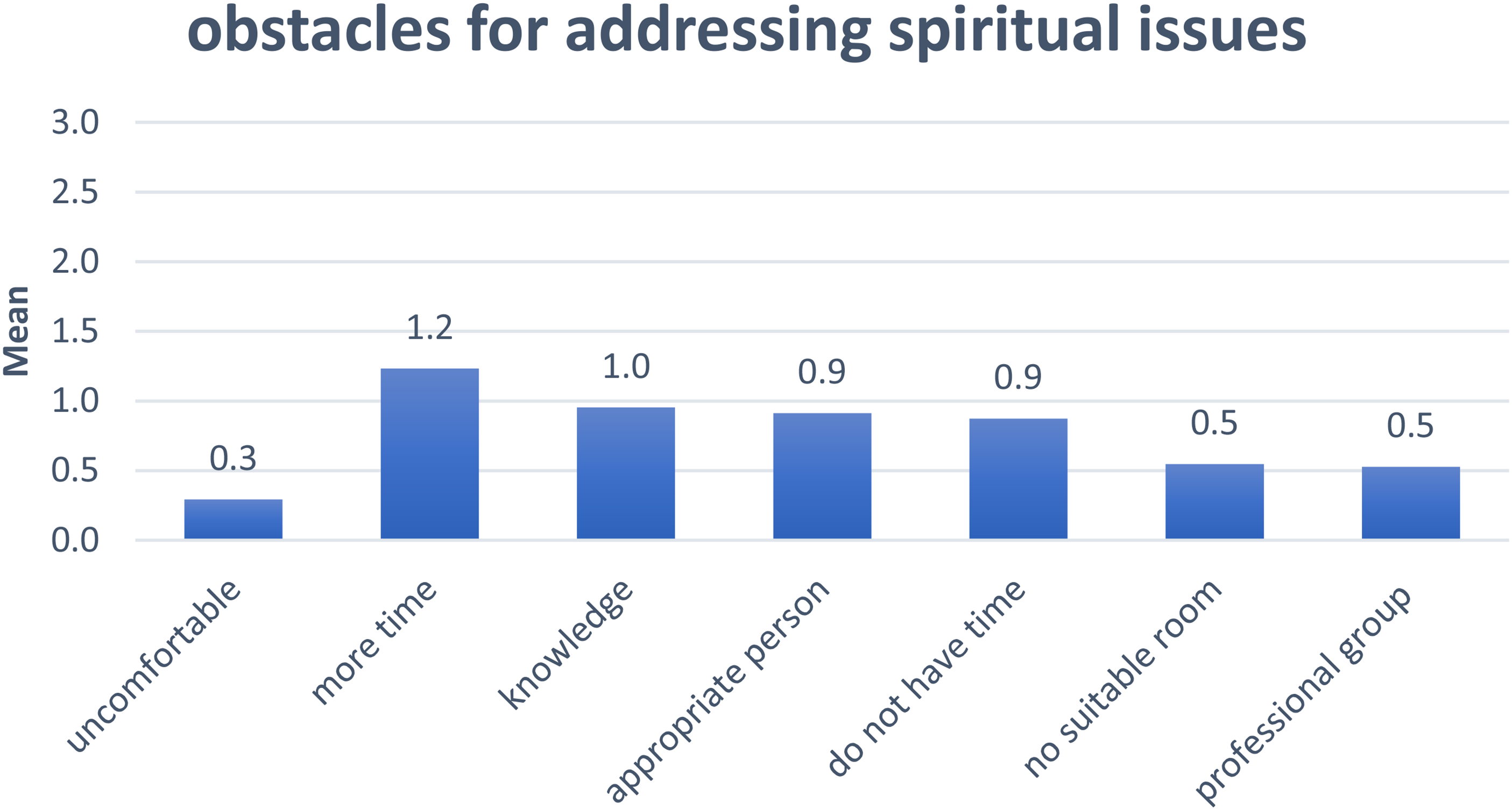
Obstacles for Addressing Spiritual Issues, Whole Sample, n = 178.
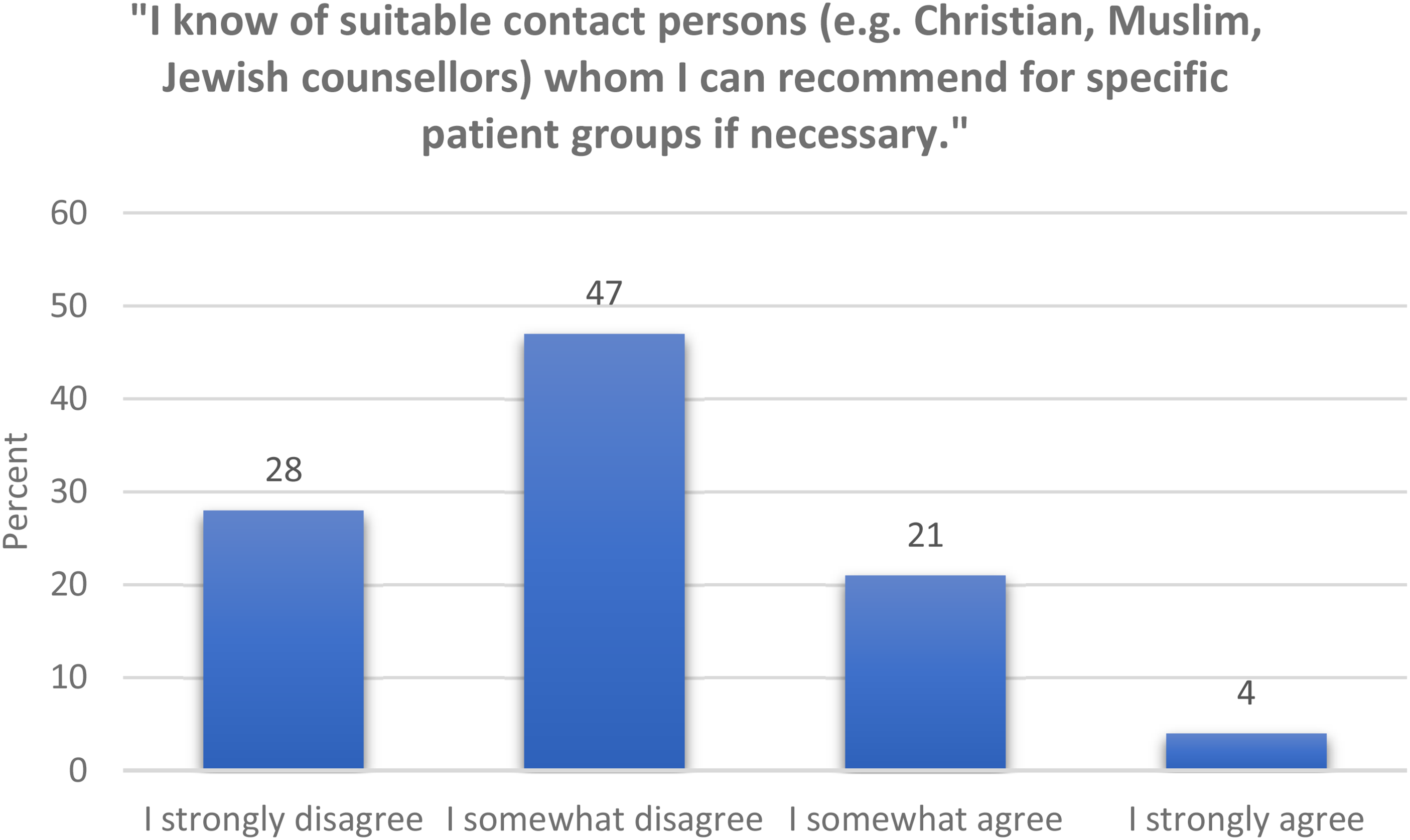
Knowledge of Suitable Contact Persons for Patients’ Religious Issues (n = 178).
Profession and Obstacles
A one-way MANOVA (results not displayed) analyzing the relationship between the variable “profession” and the seven items about obstacles did not show significant differences. The only exception was the item on time for religious/spiritual topics, where physicians agreed significantly more often than nurses, p = .004 (MDiff = .66, 95%-CI[.18, 1.15]).
Religiosity and Obstacles
A one-way MANOVA showed a statistically significant difference between believing and non-believing participants on the combined dependent variables, the seven obstacle items, F(7, 142) = 5.747, p < .001, partial η² = .221, Wilk's Λ = .779.
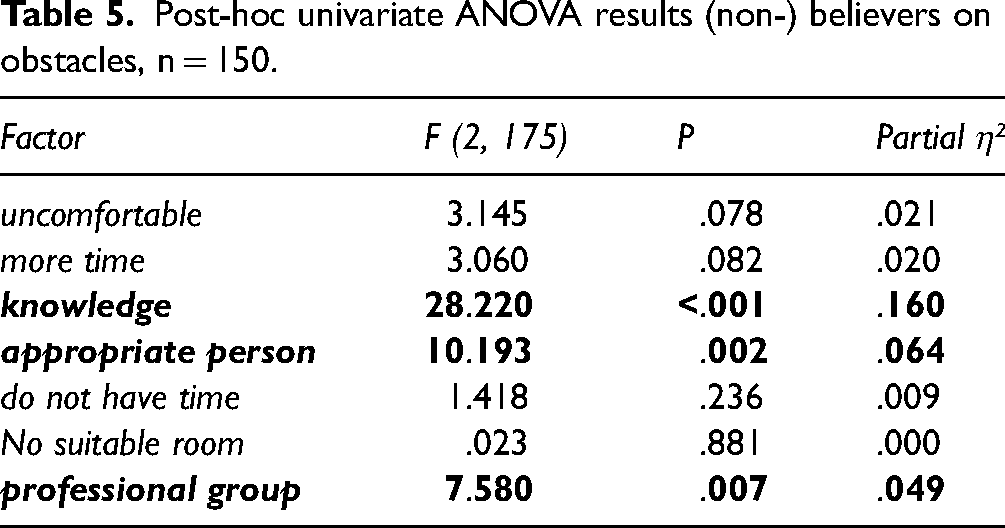
Post-hoc univariate ANOVAs show a statistically significant difference between believers and non-believers for the items knowledge, F(1, 148) = 28.220, p < .001, partial η² = .160, appropriate person, F(1, 148) = 10.193, p = .002, partial η² = .064, and professional group, F(1, 148) = 7.580, p = .007, partial η² = .049, but not for the other factors (results in Table 5). Throughout, non-believers rated obstacles higher. No difference could be found concerning the question about a suitable room.
Post-hoc univariate ANOVA results (non-) believers on obstacles, n = 150.
Age and Obstacles
A one-way MANOVA showed a statistically significant difference between age groups (under 40, 40–50, over 50 years) on the combined dependent variables, the seven obstacle items, F(14, 282) = 2.516, p = .003, partial η² = .111, Wilk's Λ = .790.
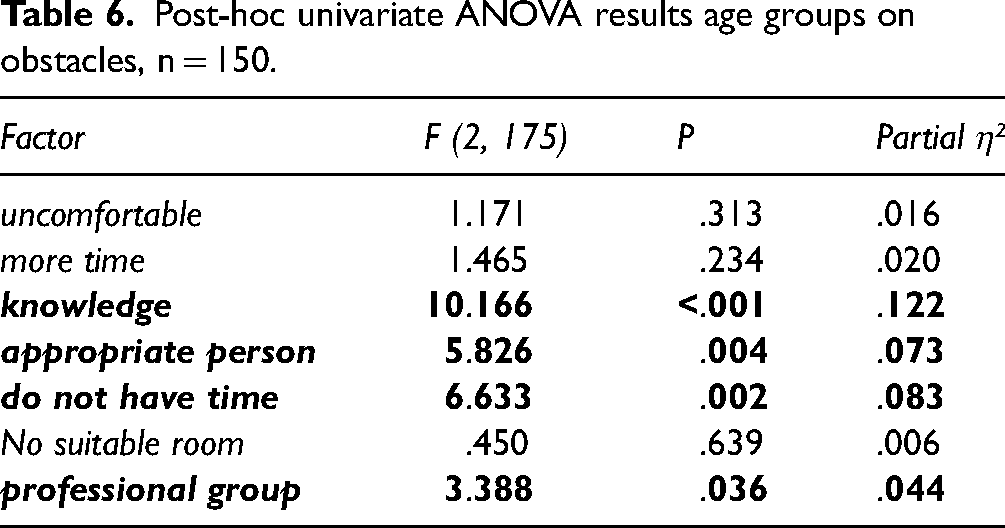
Post-hoc univariate ANOVAs show a statistically significant difference between the age groups for the items knowledge, F(2, 147) = 10.166, p < .001, partial η² = .122, appropriate person, F(2, 147) = 5.826 p = .002, partial η² = .073, do not have time, F(2, 147) = 6.633 p = .002, partial η² = .083, and professional group, F(2, 147) = 3.388, p = .036, partial η² = .044, but not for the other factors (results in Table 6). Again, older staff rate obstacles lower and would like more time for religious/spiritual needs.
Post-hoc univariate ANOVA results age groups on obstacles, n = 150.
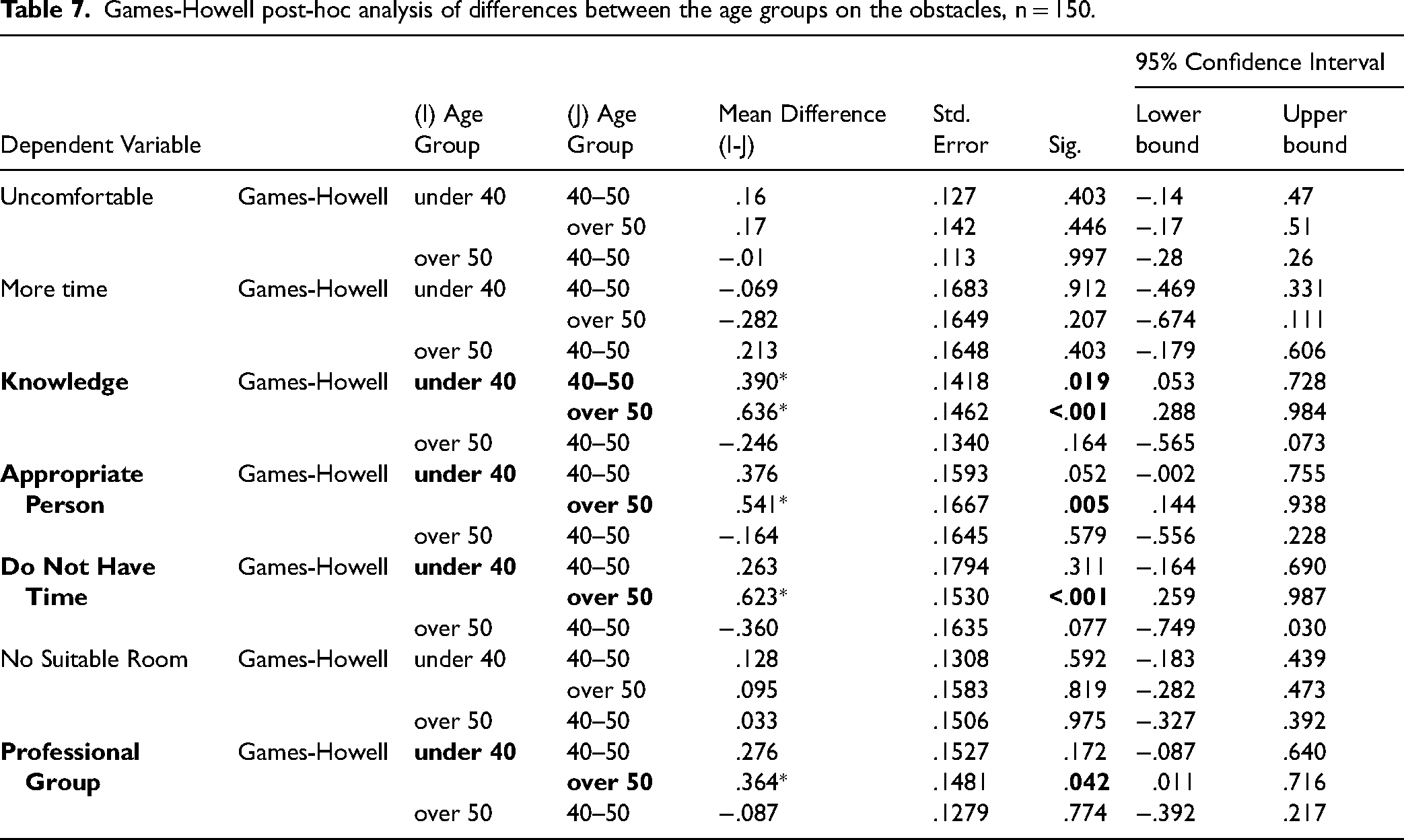
As the Box test for homogeneity of covariances was significant for these variables, Games-Howell tests were performed as a post-hoc analysis of single age-group differences on the items knowledge, appropriate person, do not have time, and professional group. The results are displayed in Table 7. The age group over 50 scored lowest on all these obstacle items.
Games-Howell post-hoc analysis of differences between the age groups on the obstacles, n = 150.
Existential vs. Religious
To investigate the impact on the choice of words (existential vs. religious) on the answer, a new variable was computed, using the difference between item 19 (“I am able to conduct an open discussion on existential issues.”) and item 20 (“I am able to conduct an open discussion on religious issues.”). A one sample t-test showed a significant result (difference > 0) with M = .14, SD = .43, t(177) = 4.569, p < .001, with a small effect (Cohen's d = .34).
A further investigation of this difference using one-way ANOVA for the variables profession and age group did not show any significant results (not displayed). The variable religiosity, however, analyzed using an independent samples t-test, showed a significant difference between non-believing participants (M = .22, SD = .48) and believing participants (M = .04, SD = .31), t(175) = 2.937, p = .002 (one-sided). Non-believing participants seem to make a stronger difference between the words existential and religious than believing participants (Figure 4).
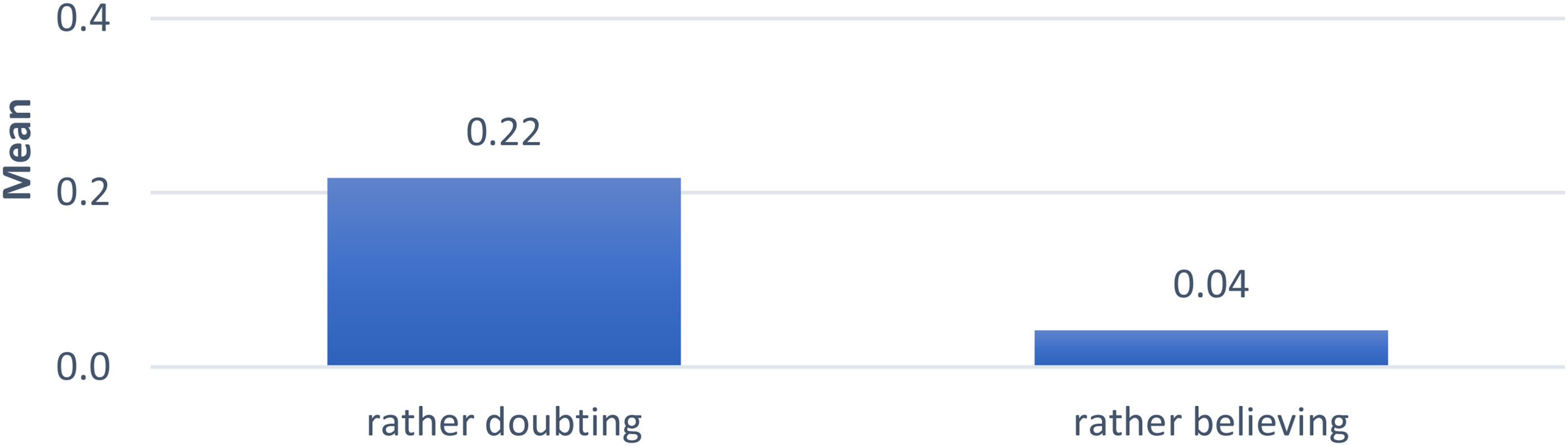
Difference Between Item 19 and Item 20 by Religiosity, N = 176.
Qualitative Results
Furthermore, a directed thematic analysis (Assarroudi et al., 2018; Hsieh & Shannon, 2005) was performed on the 131 free text answers to items 58 (“I think that my professional group has a special spiritual competence, namely:”) and 59 (“I think that my professional group is not responsible for spiritual care, because:”).
Note that translating these items was challenging because a direct translation as “spirituell omsorg” in Norwegian can easily be misunderstood as including esoteric practices. In the process of back-and-forth translation, we decided on “eksistensiell omsorg”, thus offering a broader approach. In a first step, all answers were excluded that were not understandable or did not comment explicitly on obstacles, potentials, or existential, spiritual, or religious issues, leaving 124 answers. The remaining text was coded and categorized, using linguistic differences and positive/negative connotations as orientation.
The coding resulted in three categories: obstacles (containing three codes – knowledge, personal, institutional), potentials (containing three codes – training, attitude, personal experience), and terminology (one code). Several answers could be coded in more than one category.
Obstacles and Potentials
Several participants pointed out that they had insufficient knowledge and skills, stating, for example, that they “lack training”, that there is a “need for competence regarding different cultures, religions and spirituality”, and that many professionals “draw a sharp line between the spiritual/existential and therapy, as training does not focus on this”. Other answers referred to existential competence as a personal rather than a professional property: “In my opinion, existential care is more based on the personality of the helper than on profession”. Some answers underlined insecurity, such as “many are afraid /insecure to talk about existential questions” or even “many are better at it than me”. Some acknowledged the need for existential care but blamed the institutional conditions for preventing the practice, stating: “We should be good at it, but it doesn’t fit with patient pathways”, “we’re lacking resources/time”, “We have a lot to contribute, but the conditions of work emphasize control, effectiveness, and bureaucracy”, or “productivity demands dominate”. Many answers used conditional phrases like “we should have room for that”.
The majority of the participants, however, focus on potential. They point to the experience that existential issues “are part of the formal training”, which gave them “tools/methods to give hope, care, and managing what is difficult in life”. One of the most important effects of the training, according to many answers, is an attitude that comes with a “holistic approach, a high degree of openness and curiosity”, is “nonjudgemental”, and “sees life's different dimensions as equally important”. However, most positive answers focus on personal experience as the main source of competence in existential care. “Being close to patients in life and death” and “experiencing people's existential needs/issues close-up” for many years as a professional are seen as a kind of “quantity training” on a personal level, independent of the profession.
Only two answers mentioned collaboration with chaplains to help solve patients’ existential issues.
Conceptualization
Despite the open translation of “spiritual care” as “eksistensiell omsorg”, several free-text answers noted terminological differences. They drew attention to a prevailing “positivist tendency” in the healthcare sector. Participants repeatedly drew a line between “existential” and “religious or spiritual”. They wrote, for example, that the “competence is not necessarily religious-spiritual, but existential” or that it applies to “the existential school of psychotherapy only; psychology is not mixed with religion, it is just science”.
Discussion
The study set out to answer the research question “
Irrespective of professional specialization, physicians, nurses, and psychologists report a high level of spiritual care competence, particularly regarding “perception” and “communication”. This is evident in their heightened awareness of patients’ existential needs as a crucial component of their suffering, coupled with an openness to discussing such needs. These results are confirmed and further developed through the thematic analysis of free-text answers. Many participants underline that their clinical service is interwoven with patients’ questions of life and death and that a holistic approach is part of their training. In other words, the potential for both professional and personal involvement in providing existential care within the domain of mental health care is vast, and the demand for such care is undeniable. At the same time, the possible overestimation of competence in self-reported data should not be underestimated (Oxhandler et al., 2017). Patients in Norway report a lack of room for existential issues in their encounters with professionals (Holmberg et al., 2017). Therefore, more research is needed to determine what is experienced as appropriate and helpful by both professionals and patients.
Other findings contrast the high potential. The average values for the SCCQ competence factors “team spirit”, “documentation”, and “self-awareness” were low across the professions. Healthcare professionals seem to experience existential care as something personal that happens between the lines rather than openly, for example, as a topic in team conferences or patient care documentation. Despite the openness for existential needs and their obvious relevance, healthcare providers experience role insecurity and the lack of both personal and institutional resources, as demonstrated in the thematic analysis data. Modern work culture's fast-paced and efficiency-focused nature leaves little room for existential care and deflates the potential. Current sociological theories such as the resonance theory (Rosa, 2018) support the idea that there are strong systemic factors that impact the personal experience of connectedness between patient and professional. It might therefore be helpful not to reduce existential care to a purely personal set of competencies.
Professional specialization does not play a large role in reported differences, except for one SCCQ item where psychologists appear less religious than other staff and more hesitant to integrate religious and spiritual topics in therapy (Mandelkow et al., 2022). Religiosity and age emerge as significant factors in elucidating disparities in self-reported competence. Specifically, participants aged 50 and above, as well as those identifying as religious, demonstrate a greater likelihood of asserting sufficient knowledge and personal and professional experience in addressing patients’ existential needs and exhibiting a more positive attitude towards their professional responsibility in this regard. The results of our study align with the findings from a similar study conducted in Germany using the same assessment tool (Frick et al., 2021). In line with their findings, we observed that older and more religious healthcare staff reported higher levels of competence and a stronger sense of professional responsibility in addressing religious/spiritual needs. However, our study did not replicate their findings, indicating that nurses, in particular, would exhibit higher competence ratings or report a lack of suitable rooms for addressing these needs.
The conceptualization of terms like “spirituality”, “religion”, and “the existential” as it is expressed in the choice of words seems to be of importance. We found significantly more agreement with an item asking for the ability to have an open discussion if the discussion is labeled as “existential” instead of “religious”. However, this differentiation does not apply for participants who describe themselves as religious – they are equally open to both alternatives. The qualitative data analysis strongly confirms this finding. Despite using the term “existential care” in the question, several participants utilized the free text section to emphasize the distinction between spiritual and existential care. They preferred the term “existential” as it was considered less controversial, while “spiritual” or “religious” was sometimes associated with unscientific or evangelical connotations. These findings align with the results of Danish studies on the significance of different terminologies and the need for careful differentiation (Hvidt et al., 2022).
Only 25% of the participants answered positively to the question about knowledge of suitable contact persons such as chaplains, only three of 131 free text answers mention chaplains/counselors at all, two spoke of good cooperation, and one assigned the responsibility for spirituality to them. The average values on the SCCQ factor “team spirit” are low. Therefore, despite interdisciplinary collaboration being widely acknowledged as the gold standard in spiritual care and a general willingness to address this issue, little attention appears to be given to fostering teamwork in this regard. This is even the case in institutions with religious affiliations. These findings may reveal a lack of knowledge about chaplain services, but they are also interesting with regard to the visibility of chaplains as experts in spiritual and existential care (Danbolt & Stifoss-Hanssen, 2020).
In summary, mental health care professionals in Norway appear to maneuver patients’ existential needs with passion and professional conviction but without much institutional or team backup. They regard existential competence as a personal quality that comes with age and experience rather than a professional competence that has its place in interdisciplinary teamwork.
Implications
The results of this study align with a large Danish study Nils Chr. Hvidt et al. (2022), which advocates using “the existential” as an all-encompassing notion that integrates spiritual, religious, and secular elements. This contrasts with the American research tradition, which often privileges the concept of “spirituality,” and debates, as seen in the works of Paloutzian and Park (2021) and Pargament (1999), whether “psychology of religion” should be broadened to include “spirituality.”
In Scandinavian contexts, there appears to be a move towards the adoption of the term “the existential,” which seems to be gaining traction as a way to include and transcend both spirituality and religiosity in a manner that is approachable for practitioners operating within secular healthcare systems (Hvidt & Hvidt, 2019). Reflecting this shift, a key Norwegian research center recently rebranded itself from the “Centre for Psychology of Religion” to the “Centre for Existential Health Research” in 2022 (http://religionspsykologi.no/about), emphasizing the evolving focus of their work. Moreover, research involving Norwegian psychology students, as conducted by Mandelkow and Reme (2022), indicates that while religious topics are scarcely covered in clinical training, there is an existing openness to cultural and existential considerations (Mandelkow & Reme, 2022). Given the unequivocal importance of existential care in both research and clinical contexts, a practical step would be to more actively incorporate the broad concept of existential needs and care into educational training and professional supervision. This inclusive approach could both heighten awareness and address the range of existential issues in healthcare, while avoiding the potential discomfort associated with religious connotations that may deter secular professionals from engaging with existential matters.
With these terminological reflections in mind, existential competence can be defined along the same lines as spiritual competence in publications that regard “spirituality” as the overarching concept and, as such, wider than most Scandinavians do. Spiritual care competence combines knowledge, skills, and attitudes related to patients’ religion and spirituality and are tied to their ethical integration in practice (Oxhandler & Pargament, 2018). Applied to the Western European context, this would mean sufficient knowledge about existential needs, including spiritual struggles (Exline, 2013) and their equivalents in secular societies (Hvidt & Hvidt, 2019). The skills might be best described as the ability to analyse patients’ needs with appropriate tools, such as the meaning-making matrix (La Cour & Hvidt, 2010) and helping patients to express them. Nissen and Andersen (2022) suggest the “post-secular negotiation” approach as a communication style that opens for patients’ beliefs and meaning-making systems without forcing the professional to take a stance. The corresponding attitude is often described as religious, spiritual, or cultural sensitivity (Freund, 2017; Mandelkow & Reme, 2022; Sperry, 2014). Best et al. (2016) describe conventional attitudes in health care as difficult for integrating communication about spirituality. However, it will be difficult to establish a clinical culture that corresponds with the guidelines without appropriate training and supervision.
Training in knowledge and skills, as described earlier, seems essential for shifting attitudes toward existential care competence. The correlation between age, professional experience, and self-reported competence need not be the sole focus. While it seems clear that personal and professional experience can enhance existential care competence, healthcare professionals and leaders must recognize that it can also be developed through training. This would encourage younger individuals to provide quality care to patients with existential needs.
According to Best et al. (2020), spiritual and, thus, existential care is a team effort. Across the professions, the results of our study indicate low teamwork around existential issues and, despite individual openness, a hesitant attitude towards addressing the spiritual domain unless the patient asks for it (Mandelkow et al., 2022). An analysis of obstacles might be interpreted in favor of professionals with more time for talking, a mandate for existential issues connected to their role, and a position that connects the secular and spiritual sphere—in other words: chaplains. The scarcity of professionals who are knowledgeable about suitable individuals highlights the need for an expanded provision of such services that have a long-standing tradition in Scandinavia. These services have evolved from a religious service model to an existential care model, further underscoring the urgency of meeting the demand for such care (Danbolt & Stifoss-Hanssen, 2020). Chaplains, trained in existential sensitivity, can work side by side with other professionals in mental health care. Their presence in the team can contribute significantly to raising other professionals’ awareness of existential needs, increasing the institution's sensitivity to such needs, providing supervision for challenging existential issues, and alleviating the burden of a task that some may consider time-consuming or arduous.
Limitations and Strengths
The data collected in this study are not representative of Norway, let alone Scandinavia. Rather, the findings are indicative of southern Norway but do not account for unique aspects such as the presence of the Sami minority, which is more present in northern Norway. Further, the discussion of both terminological questions and the role of chaplains is based on a small number of items – further investigations would need more and more specific survey questions. Nevertheless, we believe the number of participants is sufficient to display variation, especially as both rural and urban areas are covered, including the capital, Oslo, which is Norway's socially most diverse region.
The key strength of this study lies in its mixed-methods approach, which involved the utilization of both statistical analysis and thematic analysis in a complimentary manner.
Conclusion
To summarize the findings and the discussion, three points are salient: First, the conceptualization of the existential domain is moving from religious terminology towards an all-encompassing understanding that includes the complexity of world views in a secular society. Second, relevant training for health care professionals can enhance the quality of existential care and move beyond individual characteristics shaped by age and experience which many professionals consider the main factor of existential care competence today. Third, by fostering the understanding of existential care as a team effort, collaboration can be encouraged by establishing communication structures about existential issues and by supporting the employment of professionals who can facilitate the dialogue about the existential domain with patients and in the professional team. Following these three steps would empower mental health care practitioners to confidently respond to the question of “existential needs – who cares?” with a resounding “We do!”
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.