
Abstract
On-demand support is necessary to mitigate distress and attrition in healthcare staff. Healthcare chaplains’ scope includes such support. This pilot studied the acceptability, feasibility, and effectiveness of a Code Lavender protocol utilizing chaplain support and stress-relief items. A post-hoc analysis examined the protocol's cost-effectiveness. The results indicated the protocol's acceptability, effectiveness, feasibility, and cost-effectiveness. Healthcare worker distress can be mitigated with this simple, on-demand support utilizing the specialized skills and training of healthcare chaplains.
Healthcare workers practicing in clinical environments experience significant stress (Davidson et al., 2017). They face numerous challenges such as long hours, heavy caregiver-to-patient ratios, and patient deaths (Lovell et al., 2023). Staff are also stressed by the current healthcare system's tendency to focus on what “can” be done rather than what “should” be done (Montgomery & Lainidi, 2023). Support for staff is often delayed or overlooked, yet staff distress is leading to increasing resignation rates. Given the costs of replacing clinical staff, retention of existing workers is needed in the modern healthcare landscape (Lovell et al., 2023). Holistic staff support is a crucial means of retaining workers (DeVries et al., 2023). With their specialized training in psychological first aid, stress-management techniques, and active listening, healthcare chaplains are ideally suited to provide such support. Chaplains do not exclusively provide support to patients. Their responsibilities extend to supporting staff members and the more important staff members perceive chaplains to be, the higher their own emotional wellbeing (Gaines et al., 2023). Here we present our Code Lavender intervention, piloted in our 20-bed intensive care unit (ICU), and developed to be a self-selected, on-demand staff-support intervention tool during the immediate aftermath of difficult events.
Code Lavender
Code Lavender is a coordinated response to hospital staff members’ emotional need for holistic care in response to difficult clinical events (Tsai, 2020). The term was coined in the early 2000s by a physician at North Hawaii Community Hospital who identified a need for caregiver support (Tsai, 2020). Named after the lavender plant, known for its calming and anxiety-reducing effects, Code Lavender has become a broad term for crisis intervention/response tools in hospitals (Cleveland Clinic, 2016). With the goal of offering emotional support in real-time, Code Lavender interventions are now created and developed to fit individual hospitals’ unique cultures and needs (Tsai, 2020). Hospitals with Code Lavender protocols include Cleveland Clinic, Princeton Health, and AdventHealth Parker Hospital.
In theory, care provider emotional distress is an emergency like that of any other hospital code (Tsai, 2020). Although not an urgent medical matter like a Code Blue, these instances of emotional crisis represent critical events for caregivers (Brand, 2021; Cleveland Clinic, 2016). Health practitioners require support and compassion to tend to the feelings and thoughts associated with difficult circumstances faced on the job (Brand, 2021). Code Lavender interventions are designed to provide the emotional cushion caregivers need to complete a shift after a difficult event (Brand, 2021). Moreover, these tools help staff to feel supported and connected, to build strong work bonds and secure organizational ties, to bolster team performance and engagement, and, ultimately, to retain qualified staff (Lovell et al., 2023).
Gap Identification
Healthcare leaders must attend to their staff members’ needs for compassion-based modes of rejuvenation as a means of mitigating distress and building resiliency in the workplace (Brand, 2021). There is a gap in many healthcare organizations with respect to understanding staff care support needs and implementing actions to address those needs (Graham et al., 2019). Leaders and staff members must all commit to acknowledging the stressful nature of healthcare work, and to taking actionable steps to promote self-care (Phillips et al., 2018). Indeed, creating a structure and process that recognizes colleagues under stress is essential to optimizing the healing environment (Graham et al., 2019). Thus, crafting dedicated times and designated spaces for in-person dialogue and support following stressful events can be helpful in promoting resilience (Delassalle & Cavaciuti, 2023; Gregory, 2021). As noted at our facility and elsewhere, the high stress environment amid the COVID-19 pandemic highlighted the important role chaplains may play in attending to staff care needs (Tartaglia et al., 2024). Chaplains offering Code Lavender interventions is one simple yet effective strategy to meet healthcare providers’ needs for support and care (Gregory, 2021).
Conceptual Framework
Compassion-based care is a holistic, prompt, intensive, emotionally and/or spiritually supportive strategy (Greene, 2014). Code Lavender, as a component of compassion-based care, communicates to staff that support is available to help alleviate suffering when needed. This type of compassion-based care supports the idea that time must be taken to “replenish and rejuvenate” after a stressful event (Phillips et al., 2018). Thus, facilitation of a Code Lavender falls within the domain of hospital chaplains.
Compassion has been defined as “caring toward another's suffering and being present emotionally” (Straughair, 2019, p. 98). Recognizing another's suffering often leads to helpful actions in an attempt to alleviate the witnessed suffering. Actions such as listening, touch, a kind act, competent interventions, or seeking to understand the other's experience demonstrate compassion (Koloroutis, 2004). Compassion and care are experienced in the moment when one person connects with another person. This establishment of connection is echoed in the organizational model of Relationship-Based Care (RBC).
The RBC model centralizes and recognizes the powerful effect of relationships (Koloroutis, 2004). The model recognizes different relationships staff members have in healthcare settings: relationships with patients and families, relationships with colleagues, and relationships with self (Koloroutis, 2004). This is the care model used in our organization and our pilot study focused specifically on enhancing relationships among colleagues and relationships with self. Consistent with the tenets of RBC we began by recognizing that healthcare professionals come to work because they choose to care for people who are suffering. We wanted to provide a mechanism by which staff members could experience care and compassion themselves in response to their own suffering. Through deliberate action we wanted to harness the power of a healing relationship among colleagues. We also wanted to create time and space for people to engage in actions that demonstrate self-care and self-compassion.
Intervention Development
The facility where this pilot study took place is a regional, 121-bed, suburban, level III trauma hospital in the western United States. This Code Lavender pilot program was developed by a multidisciplinary team and led by chaplains. The pilot aimed to provide both tangible and emotional stress-relief tools for the hospital's ICU staff, including registered nurses, certified nursing assistants, respiratory therapists, providers, and physicians. The ICU was selected for the pilot due to its size and patient acuity.
Preliminary work on the Code Lavender pilot project began during the height of the COVID-19 pandemic. Like most hospitals, the infection and death rates were rapidly escalating during the early waves of the pandemic. The ICU bore the brunt of the hospital's COVID-19 infections, with extremely high census and acuity. Staff grappled with daily stress, anxiety, and fear. One of the hospital's chaplains witnessed these emotions and provided the following reflection on the pandemic's impact on the ICU: I served as a chaplain in (the hospital's) ICU in the fall of 2021 — during what I have termed the “angry surge” of Covid. Many families with loved ones in the ICU were attached to a narrative that made it difficult for them to accept a Covid diagnosis. Additionally, visitor restrictions for Covid patients resulted in isolation and increased fear and anger. The hospital staff became the outlet for their profound grief. I witnessed multiple family members blaming staff for “killing” their loved ones, swatting at staff, and threatening staff. ICU staff faced daily resistance and hostility for many months, while continuing to tenderly care for patients. Exhaustion and frustration became continuing undercurrents.
In response, the purpose and scope of the pilot program was presented to the ICU leadership and the hospital's executive team by the chaplain team together with nurse leaders. Approval was granted, and financial support was provided by the Chief Nursing Officer. The original intent was to recruit and train members of other departments to participate as Code Lavender responders in collaboration with the hospital's spiritual care team. Due to time and personnel constraints, staff members from other departments were not able to participate. Following approvals and the prescribed education period of one month, the Code Lavender Pilot went live in June 2022. At that time, Covid infections and deaths were waning in the region and the hospital was no longer inundated with cases and deaths (Centers for Disease Control and Prevention, 2023). Nevertheless, the emotional toll of the pandemic was still palpable.
Purpose
The primary objectives of the Code Lavender pilot study were to assess the acceptability, feasibility, and effectiveness of the urgent response team's interventions in the hospital's ICU. Primary questions posed were a) is the Code Lavender protocol designed by the team achievable? b) do ICU staff perceive Code Lavender interventions as helpful and meaningful? and c) do staff perceive the Code Lavender interventions as supportive? After the pilot study's completion, a post-hoc analysis to assess cost-effectiveness of the intervention compared to nurse turnover costs was completed.
Methods
Population and Setting
This was a pilot study with a pre and post assessment using convenience sampling. The target population consisted of 157 staff members including registered nurses, certified nursing assistants, respiratory therapists, providers, physicians, and ancillary associates who worked in the ICU between June 20 and September 20, 2022. There is only one 20 bed ICU in the hospital and chaplains and staff members are known to one another to varying degrees. The chaplains are responsible for covering every department in the hospital and are assigned to specific units, but coverage varies daily. There is one full-time staff chaplain working weekdays, alongside ACPE Clinical Pastoral Education (CPE) residents and interns. A chaplain is on-call on weeknights, and CPE students provide on-call coverage on weekends, beginning Friday at 5pm-Monday at 8am. The CPE residents and interns rotate quarterly and changed in mid-August during the project. During the pilot the ICU and spiritual care departments were adequately staffed. Once the Code Lavender program was initiated there was no point in time that pandemic related workload or understaffing impacted its availability.
Procedures
Upon receipt of CommonSpirit Institutional Review Board approval (# 1906570-2), an email inviting eligible staff members to participate was distributed via organizational email account; follow-up emails were sent every Monday for three weeks. An informational flyer describing the nature and purpose of the study was posted in the ICU breakroom and staff restrooms, and communication about the Code Lavender pilot program was disseminated at staff meetings. Clear explanations were provided including that access to Code Lavender interventions was independent of participation in research activities. After being screened for eligibility by the primary investigator, those interested in participating in the Code Lavender research were emailed links to the pre-intervention survey. Completion of the surveys implied consent to participate, and participants were notified of their right to withdraw from the study at any point without penalty. The only foreseeable risk associated with participation was the potential for experiencing painful feelings or memories related to the difficult situation being addressed. All Code Lavender participants were given information for the hospital's Employee Assistance Program if a need for follow up support was identified.
Intervention
The Code Lavender program went live in the ICU on June 20, 2022, after one month of staff education regarding its purpose. Flyers were posted notifying staff that any ICU staff member who perceived an acute need for emotional care for themselves or for someone on their team (e.g., after a complicated Code Blue, workplace violence event, or difficult death) could call a Code Lavender. Paging the on-call chaplain initiated the Code Lavender intervention. The intervention response team, consisting of at least one chaplain, arrived on the unit within two hours of the call. In addition to their physical and emotional presence, they brought the Code Lavender supply basket. Basket contents included self-care items (e.g., bath bombs, hand cream, essential oils, fuzzy socks, eye pillows), treat items (e.g., luxury chocolates and snacks, high-end teas and coffees, hospital coffee shop gift cards), and other resources (e.g., crisis phone numbers, bookmarks, poetry and verses, mandalas, stress balls, chaplain contact cards). The chaplain response team was present, offering empathic support and opportunities for conversation. Although a single staff member typically initiated the Code Lavender call, interventions were provided to the whole unit to mitigate stigma or embarrassment. The basket and supplies were left on the unit for the remainder of the shift.
Measures
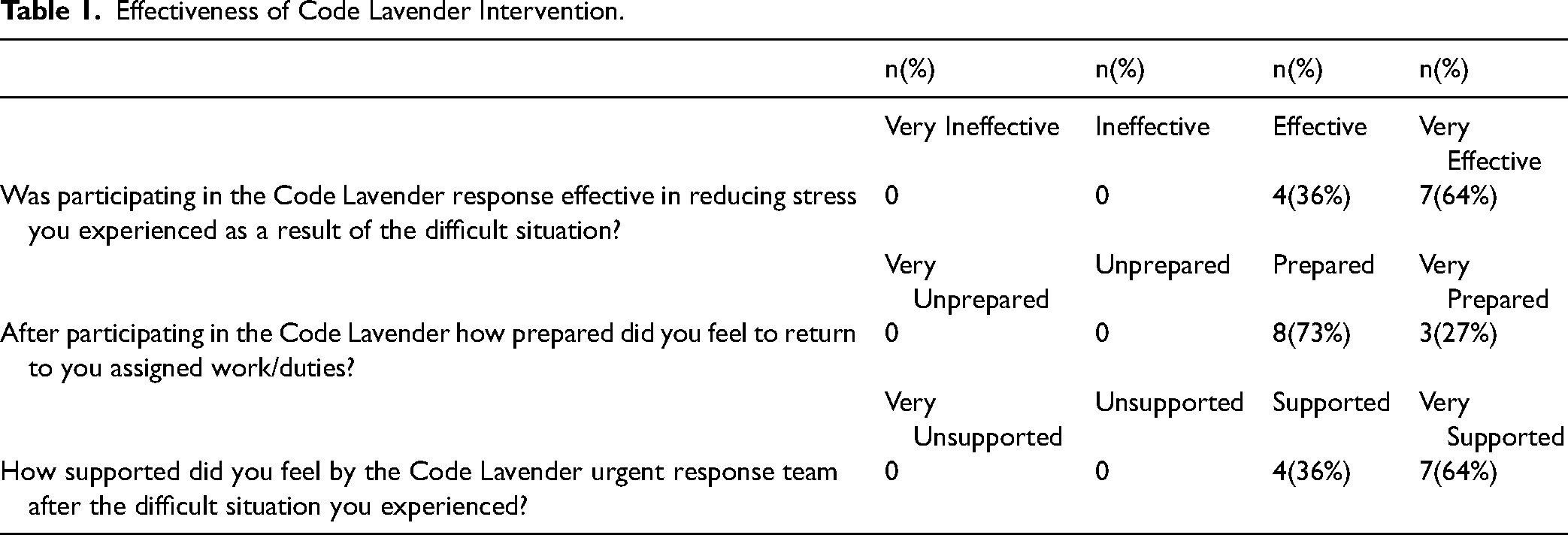
Members of the research team with expertise in spiritual care in the ICU setting developed pre and post-intervention surveys. The pre-intervention survey was emailed to participants during the month prior to the Code Lavender program beginning and had two questions: Would you be open to calling a Code Lavender after experiencing a difficult situation (yes/no)? How likely would you be to call a Code Lavender after experiencing a difficult situation (4-point Likert scale)? The post-intervention survey had eight questions. Questions 1–3 assessed effectiveness with a 4-point Likert scale: 1) How supported did you feel by the Code Lavender urgent response team after the difficult situation you experienced? 2) Was participating in the Code Lavender response effective in reducing stress you experienced as a result of the difficult situation? 3) After participating in the Code Lavender how prepared did you feel to return to your assigned work/duties? Questions 4 and 5 assessed acceptability with yes/no questions: 4) Would you call a Code Lavender again in the future after a difficult situation in your department? 5) Would you recommend calling a Code Lavender to colleagues who experience a difficult situation in their work environments? Answers to questions 6, 7, and 8 were narrative: 6) What, if anything, did the Code Lavender urgent response team do that made you feel supported? 7) What, if anything, did the Code Lavender urgent response team do that made you feel unsupported? 8) What was meaningful in the Code Lavender response?
Data Collection and Analysis
Throughout the three-month study timeframe, Code Lavender requests were logged by the response team. Documentation included the number and reasons for the interventions, participants’ names and roles, the duration of the Code Lavender intervention, and supplies from the basket utilized by participants. Members of the research team then cross-referenced attendance sheets with the list of study participants. Within 48 h of each Code Lavender, study participants who had attended the intervention were emailed a link via organizational email to the post-intervention survey. A prompt response was requested.
Feasibility was measured by logging all calls and noting the Code Lavender team's response time as well as the duration of the interventions. A feasibility threshold was set at a maximum of 2 h response time. Acceptability was measured by documenting the number of Code Lavender calls, the stated reasons for the calls, and the numbers and disciplines of clinical team members present during the interventions. Effectiveness of Code Lavender interventions was evaluated by post-intervention surveys assessing perceptions of support. All data analysis was descriptive in nature and no inferential statistical testing was done.
Results
Eleven individuals completed pre and post intervention surveys; there was no attrition. Occupation was the only demographic information collected from respondents. Nine respondents were registered nurses, 2 were respiratory therapists. Pre-intervention, all respondents (11, 100%) indicated they were “open” to calling a Code Lavender after experiencing a difficult situation, and 9 (80%) were “likely” or “very likely” to call a Code Lavender. Twelve Code Lavender requests were made by the ICU staff during the three-month study period. Seventy-seven people attended Code Lavender interventions. Attendance ranged from 3–10 and averaged 6 staff members. Attendees were primarily registered nurses (n = 60), certified nursing assistants (n = 5), and respiratory therapists (n = 8); 1 physician, 2 social workers, and 1 ancillary staff person also participated in Code Lavender responses. Chaplain response time to each event ranged from 5 to 30 min, with an average of 10 min. See Table 1 for post-intervention survey results related to perceptions of support, stress, and readiness to return to work. Responses indicated that 100% (11) of respondents would call a Code Lavender again in the future, and 100% (11) would recommend calling a Code Lavender to colleagues.
Effectiveness of Code Lavender Intervention.
Narrative Responses
The open-ended post-intervention survey questions elicited narrative responses from participants. The first of these questions read: “What, if anything, did the Code Lavender urgent response team do that made you feel supported?” Responses to this question included: “Being present, listening to us, touching back with us after,” “It was nice to be treated to popcorn! Also, I can recall moments in my career- difficult patients, patient passing or coding- where a Code Lavender would have been appropriate. I’ll utilize this in the future, as I think it's a great idea,” “Gave much needed reprieve in a day full of chaos,” and “Making the break room into a place to relax!”
The second question asked, “What, if anything, did the Code Lavender urgent response team do that made you feel unsupported?” Responses to this question included: “Nothing, they went above and beyond, it was so appreciated,” and “Nothing, the team is reachable.”
Finally, participants were asked, “What was meaningful in the Code Lavender response?” Respondents offered the following insights: “Everything: chaplain support and presence, snacks, supportive tools for after work,” “Great chance to take a break and enjoy something nice,” “Knowing this team exists to help us when we need it,” and “Everything. My expectations were blown out of the water.”
Cost-Effectiveness
There was no significant turnover in ICU staff participating in this Code Lavender program. During the three-month pilot study period just under $800 was spent on Code Lavender supplies. The average hospital chaplain was paid $27 per hour and during the pilot period chaplains spent an average of 2 h per week responding to Code Lavender calls; it is estimated that $648 in chaplain wages was spent on Code Lavender responses during the pilot period. Utilizing these figures, it is possible to extrapolate that a single-unit, year-long project such as ours, using similar supplies and employing 2 chaplain hours per week would cost an organization ∼$5,700 per year. The turnover of a single registered nurse is estimated to cost an organization $52,350 (Gamble, 2023). If the presence of the Code Lavender response team for a year prevents a single nurse from leaving, the organization will have saved more than $46,650.
Discussion
This pilot study showed that an innovative and simple on-demand Code Lavender protocol facilitated by hospital chaplains was acceptable, effective, feasible, and cost effective in an ICU in a tertiary care hospital.
Resilience
One caregiver's post-intervention survey response suggested that participation in a Code Lavender intervention led them to reflect on previous difficult events in their career. Connecting experiences in this way demonstrates integration as well as grounding, both of which are important tools for resilience. The cultivation of resilience is crucial in the context of a predicted future nursing shortage. Code Lavender staff responses reinforce the need for holistic wellness programs to support healthcare workers in that effort and underscores the urgent need for creative and sustainable support and care for healthcare staff to mitigate avoidable loss (Lovell et al., 2023). The expressions of gratitude and acceptance by staff for both the items selected by the research team and the transformation of their usual staff breakroom into a place to “relax” when participating in Code Lavender interventions demonstrated the impact on attendees’ resiliency.
In an effort to maximize receptivity, the research team selected a range of items for the Code Lavender response basket including fun and silly items in addition to snacks, treats, and more traditional self-care items like essential oils and mandalas. For instance, squishy unicorns were selected in lieu of lavender stress-balls. These unicorns proved to be one of the pilot's most popular items as a source of playfulness and joy amidst the stress of the ICU. In his work on Family Systems Theory, Edwin Friedman noted that “nurturing and playfulness evolve together” while “chronic anxiety is a regressive emotional process” (Friedman, 2007, p. 79, 84). Including items that prompted laughter and joy in the Code Lavender protocol was intentional and resulted in playful banter and moments of joy the pilot team envisioned. Staff members appreciated the emotional support provided by the chaplain's presence and empathic communication. Whether staff members needed play and lightheartedness or to verbally process their emotions the Code Lavender team was prepared to offer whatever response was necessary.
Incidentally, initiation of the Code Lavender pilot coincided with the unforeseen resignation of the ICU's manager. Staff members of the unit expressed feeling “leaderless” during much of the pilot. Their genuine appreciation at being remembered and supported by employees in the hospital (chaplains) outside of their unit was reflected in the survey responses. These expressions of appreciation reflect organizational care, commitment, and compassion.
COVID-19 Pandemic
Although the Code Lavender pilot took place in the summer of 2022 when Covid infections and deaths were no longer surging in the state as they had been when the pilot was conceived the previous fall (Centers for Disease Control and Prevention, 2023), staff continued to identify feeling highly stressed by a range of issues. As the pandemic ebbed, so too did morale, which was exacerbated when the manager resigned, leaving the unit struggling with a lack of leadership. Of the original sixty-five nurses employed on the ICU at the start of the pandemic, fewer than thirty remained when the Code Lavender pilot began.
Indeed, emerging data indicates that enduring pandemic effects are causing similar attrition across the country (DeVries et al., 2023; Gamble, 2023). The National Council of State Boards of Nursing (NCSBN) recently announced that in their study, over 700,000 registered nurses have either left or intend to leave the field within the next four years (NSCBN, 2023). Nurses report feeling emotionally drained, used up, fatigued, burned out, or at the end of the rope weekly if not daily. It has been suggested that “the U.S. health care ecosystem is at an urgent crossroads” and that leaders must “coalesce and enact solutions that will spur positive systemic evolution to address these challenges” (NSCBN, 2023). Sixty nurses, nearly every nurse from the unit, participated in Code Lavenders during the pilot; nurse turnover was also minimal during that time.
Cost-Effectiveness
A post-hoc cost/benefit analysis revealed the value of a Code Lavender protocol. By this rough estimation, the cost of a Code Lavender protocol is approximately 9% the cost of replacing a single nurse (Gamble, 2023). Furthermore, retaining experienced, committed staff represents multi-layered value for a healthcare institution beyond the financial bottom line (DeVries et al., 2023). In the post-pandemic healthcare landscape, a Code Lavender protocol like the one implemented here by chaplains is a relatively low-stakes, high-reward tool that provides on-demand tangible stress-relief for staff members. The pilot demonstrated that when staff members feel their experiences of stress and grief are validated, they are less distressed and better prepared to care for their patients moving forward. These positive outcomes indicate that Code Lavender responses facilitated by chaplains provided value for nurses in their practice, and for the leaders of their units, departments, and hospitals.
Limitations
Although these findings are positive, generalizability is limited by the sampling method and small sample size from one ICU at a single site. Findings are descriptive and lack inferential statistical analysis limiting the ability to draw conclusions. Expansion of the project to additional sites would allow for further examination with a larger sample. The survey used was developed by the research team and was not a pre-existing validated instrument. Results could also be strengthened by a rigorous qualitative analysis of the themes identified in the open-ended responses, a project that will be pursued in the future. The results could be biased from the convenience sampling if participants who volunteered to respond to the surveys are also those most likely to participate in Code Lavender interventions. Additionally, a more robust cost effectiveness analysis could be conducted using actual wages and staff turnover numbers. Despite these limitations, our study is the first step in examining outcomes of a pilot Code Lavender program implemented by chaplains. With limited financial resources and time, the Code Lavender pilot focused on the unique context of the ICU however this Code Lavender protocol is scalable to any size unit or hospital. The limitations for implementation are 1) funding for basket items and 2) chaplains committed to sustaining the protocol.
Conclusion
The Code Lavender pilot outcomes indicate that its purpose was achieved. The interventions provided effective and meaningful opportunities for support for ICU staff. Participants in the Code Lavender interventions expressed positive feedback and were eager to continue the program after the pilot study concluded. Compassionate care for staff is a clear need that hospitals must address urgently. The Code Lavender pilot study results indicate that simple, immediate support for staff who are feeling overwhelmed and distressed can be deeply impactful. Given their training and unique role within hospitals, healthcare chaplains are ideally suited to provide the kind of support this Code Lavender study describes. Indeed, this modest and inexpensive form of outreach resulted in positive staff responses. Further, our rough cost/benefit analysis showed potential cost savings. The potential financial impact could be magnified if a future study were to compare staff turnover rates before and after a Code Lavender program implementation. In short, amid the traumatic atmosphere of the ICU, this Code Lavender protocol offered innovative support, using chaplain expertise along with stress-relief items to provide support for staff, offering a meaningful moment of care and compassion.
Footnotes
Acknowledgements
The authors would like to thank the following people from St Anthony North Hospital for their support of this project: Audrey Scrimgeour, Director of Nursing Excellence; Jessie Thurber-Dean, VP of Nursing and Chief Nursing Officer; Donna Jo Martinez, Business Support; Lisa M. Campbell, Hospital Chaplain
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
This study received approval from the CommonSpirit IRB (Approval # 1906570-1) on May 12, 2022.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Participants’ completion of the online survey implied consent to participate.
Summary
This Code Lavender intervention was an effective method for providing much-needed support for healthcare staff.