
Abstract
There is a growing public support for medical interventions at the End of Life (EoL), such as euthanasia and physician assisted suicide (EPAS) and palliative sedation (PS). This paper explores pastors’ views and their pastoral care on the place of EPAS and PS and uses a 2.556 pastors’ survey.
Keywords
Introduction
End of life (EOL) in the Netherlands increasingly involves medical interventions, which in addition to life-prolonging measures include Euthanasia/Physician Assisted Suicide (EPAS) and Palliative Sedation (PS). In euthanasia the patient dies through intravenous administration of lethal drugs while in assisted suicide the patient swallows a deadly medication provided by their physician. With PS, the patient is put into a deep and usually permanent sleep until death. The percentages of people that are given PS in the Netherlands are strongly increasing (Heijltjes et al., 2020). From 2005 to 2022, the percentage of deaths that were preceded by PS in the Netherlands rose from 8.2% to 26% (Stichting Farmaceutische Kengetallen 2023). In addition, 9,958 cases of EPAS were reported in 2024, which is 5.8% of all deaths in the Netherlands (Regionale Toetsingscommissie, 2025). The numbers for PS also appear to be rising internationally, as shown in figures from the US (Bruinsma et al., 2013), UK (Seale, 2010), Belgium (Chambaere et al., 2015) and Austria (Schur et al., 2016). In Switzerland, for example, the number of deaths involving PS was four times higher in 2023 than in 2001: 24.5% vs. 6.7% (Bosshard et al., 2016; Ziegler et al., 2018). The increasing trend over time appears to be related to changes in medical end-of-life practices rather than to patients’ clinical characteristics (Ziegler et al., 2018). So far, in the Netherlands there is no research on the possible causes of this increase in PS. Den Hartogh (2023) suggests that that is prompted by doctors, who would have a propensity to shorten the time the patient suffers. According to all existing guidelines on PS, a patient should be actively involved in this decision-making process. In practice, this discussion is often postponed and consultation during the last stage of life is often no longer possible, resulting in sedation that is begun without consulting the patient but usually involving their loved ones (Robijn et al., 2016). In Dutch practice, EPAS at this stage without prior consultation of the patient is out of the question.
From the physicians’ perspective (Miccinesia et al., 2006; Cohen et al., 2006) and from the nurses’ perspective (Gielen et al., 2009; Vézina-Im et al., 2014) there is a lot of attention in the literature on the attitudes towards and experiences with proactive interventions at the EoL. Less is known about the attitudes and experiences of pastors – that other group of professionals that are frequently involved at the EoL. Boer et al. (2019) and Graafland et al. (2022, 2023a, 2023b) have published about Dutch Protestant pastors’ experiences with EPAS and about the dilemmas this group encounters. In both the more orthodox and the more liberal subdenominations pastors are encountering parishioners with an EPAS-request, but major differences in their normative views are found between subdenominations. When asked about EPAS in patients with a natural life expectancy of six months or less, 86.4% of the orthodox pastors said that this contradicts their Christian faith, whereas 15.6% in the group of liberal pastors said this contradicts their Christian faith. Support for EPAS for patients with a longer life expectancy (e.g., psychological disorders, dementia, accumulated age-related disorders and a ‘completed life’) is much lower. However, thus far, no research has been published on pastors’ views and experiences regarding PS.
PS and EPAS: the concepts ( RDMA, 2022 )
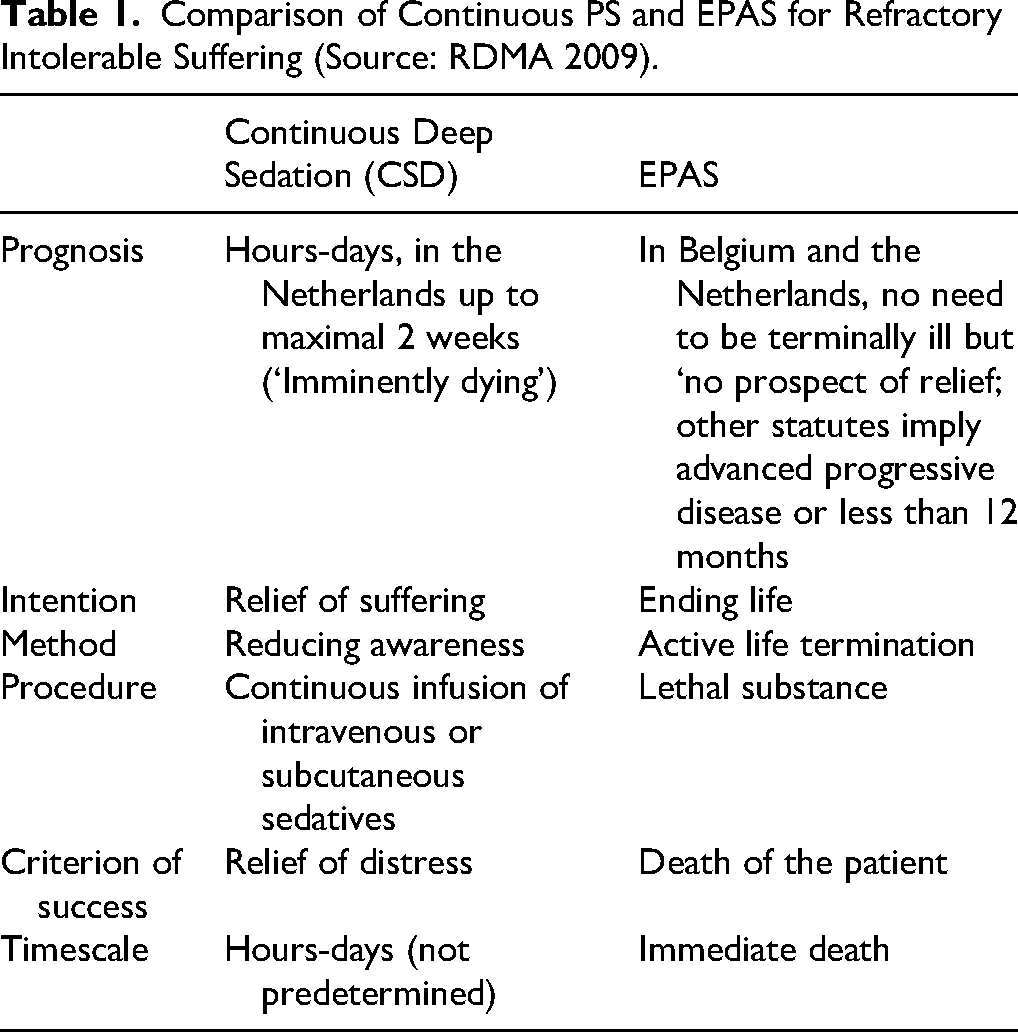
PS and EPAS are two important medical interventions worldwide in EoL-care. In the Netherlands, PS involves patients with a life expectancy of two weeks or less being put into a deep sleep until their death (KNMG Guideline 2009, 2022). Refractory symptoms such as pain, dyspnea and delirium cannot be adequately treated with the usual palliative means and a deep sleep is assumed to be the only remaining option (KNMG, 2022). Three different forms can be distinguished: (1) crisis sedation for very severe sudden symptoms, usually leading to an immediate death, (2) intermittent or short-term sedation and (3) deep continuous sedation until death (CSD). This latter form of PS involves a ‘dual procedure’ in which patients no longer receive nutrition or hydration and is the most used in the Netherlands. There are now many international guidelines for PS. There are two important differences between them: first, the patient's life-expectancy, which varies from 4–14 days, where the limit should be set at 4 rather than 14 days. Furthermore, the question of whether existential suffering in addition to the more physical refractory symptoms is an indication for PS. All guidelines advocate restraint in the use of the continuous form of PS and the restriction to the partial, titration form of PS. In practice, there is usually CSD, which means that here EPAS and PS approach each other closely, which can sometimes lead to confusion for the patient, their relatives and other bystanders, such as the pastor. (See Table 1 for an overview). There is international consensus that PS is a form of responsible medical action in the above situations. There is more discussion about applying CSD in combination with food and fluid deprivation. This combination varies greatly in occurrence in Europe, but is most frequently used in the Netherlands, i.e., in 79% of all cases of sedation (van der Heide et al., 2012). In comparison: Italy 35%, Flanders 39%, Sweden 56%, Germany and Switzerland 60%, Denmark 64% (Miccinesia et al., 2006). Critics often regard this CSD without the administration of fluids as disproportionate medical action and cannot be properly separated from EPAS. In addition, PS, which is generally regarded as ‘normal medical practice’, can be quite complex. There is sufficient support for this for the performing physician in the Netherlands, but the necessary errors can nevertheless be made during the implementation.
Ethical questions also recur in medical-ethical reflections about PS. These include: 1) providing PS for cases of existential suffering (Anneser, 2018; Bozzaro, 2018; Ciancio et al., 2019; Kamprad & Helm, 2018; Miccinesi et al., 2017; Rodrigues et al., 2018; Voeuk et al., 2017), 2) the proportionality of cases of CSD (Anneser, 2018; den Hartog, 2016; Kamprad & Helm, 2018; McCammon, 2015; Miccinesi et al., 2017; Sulmasy, 2018), 3) PS as a last resort (Meilaender, 2018; Miccinesi et al., 2017), 4) PS for patients who are not yet completely terminal (Anneser, 2018; den Hartog, 2016) and 5) the grey area between EPAS, PS and the use of palliative opiates (Riisfeldt, 2019).
Comparison of Continuous PS and EPAS for Refractory Intolerable Suffering (Source: RDMA 2009).
Although PS, and particularly CSD, is a significant portion of total deaths, this has not resulted in much ethical or political discussion. While CSD according to the guidelines should be reserved for exceptional situations, ‘dying while asleep’ seems to have become a new normal in the Netherlands (Scholten, 2022). Furthermore, according to critics, this maximum form of sedation is not necessary to relieve suffering or to provide comfort and, in most cases, lower doses of sedatives will suffice (Scholten 2022).
The difference in how different forms of PS is applied has to do with different objectives. For example, in the UK the aim is to relieve symptoms, which in many cases is possible with lower doses of sedatives, while in the Netherlands the goal with continuous sedation is often ‘to put the patient to sleep’ (Seymour et al., 2015) and to control the dying process. Above all, Seale et al. (1997) make it clear that in the Netherlands, in contrast to the UK, the emphasis is on the specific moment when sedation starts, which is often preceded by a family gathering when family members can say farewell to their loved one and after which the patient's biographical life ends. Thus, PS and EPAS may function to take the dying process into their own hands and not to experience dying and the accompanying emotions. Despite the differences between PS and EPAS, in Dutch practice, there are also considerable similarities (see Table 1).
As mentioned, little is known about pastoral care in PS situations. Since PS has become an increasingly frequent EoL phenomenon in pastoral practice, and because many may find the similarities between PS and EPAS confusing, this study will examine pastors’ attitudes towards PS and compare those attitudes with their attitudes towards EPAS. Our study is based on a 2017 survey which was the premise for a publication on pastors and EPAS (Boer et al. 2019). Although it included questions about PS, the PS data was not analysed. This article will address the following questions:
What are pastors’ experiences with EPAS and PS (and how does this relate to their different sub-dominations?) What problems do pastors experience regarding PS in their pastoral practice? What are their personal views on PS? Does the Bible play a role in pastors’ attitudes towards EPAS and PS and do parishioners ask their pastor about the Biblical perspective of PS?
Methods
Design Setting and Study Population
This cross-sectional study used a database containing 2,556 pastors registered in the Protestant Church in the Netherlands (PCN). It is comprised of pastors serving in congregations, retired pastors up to the age of seventy, and pastors serving no congregations, most of whom work in care facilities. The number of fully completed questionnaires came to 684, which is a 26.8% response rate. Forms that were not fully completed were excluded from the quantitative analysis. Still, in some of these questionnaire's answers to the open-ended questions could be used for qualitative purposes. For the present study we specifically used answers to the following question: ‘Which difficulties or dilemmas did you experience during your pastoral care with regard to medical interventions at the EoL?’ The answers were anonymized, and the data stored at the National Protestant Services Centre in Utrecht (PLD).
Variables
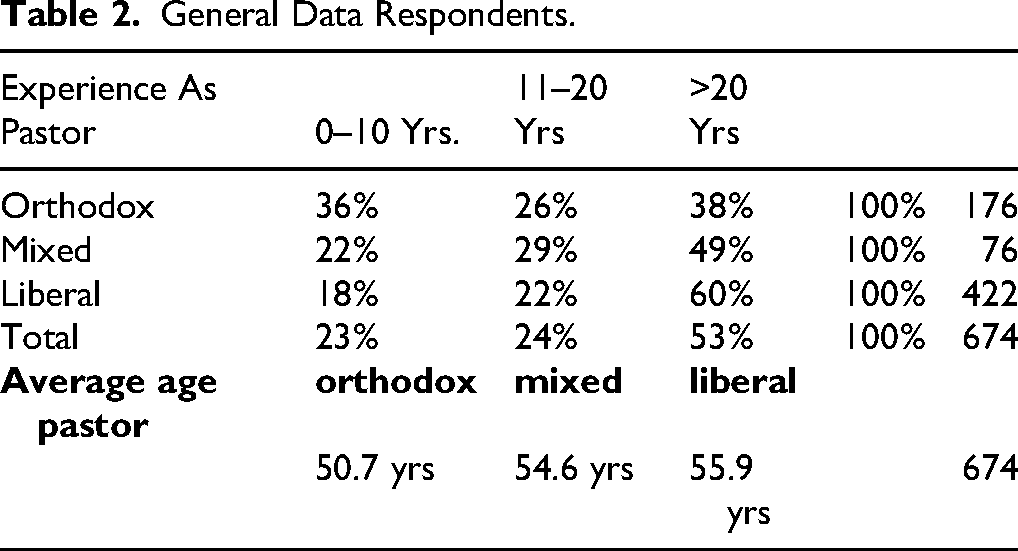
Questions on background characteristics included the pastor's age (26–40, 41–50, 51–60, >61 years), years of professional experience (0–5, 6–10, 11–20, >20) and their self-perceived subdenomination within the PCN. The PCN is a plural church with congregations and pastors belonging to different subdenominations that we here categorized into three: ‘orthodox,’ ‘liberal’ and ‘mixed’ (or ‘mainstream). They are characterized by differences in Bible interpretation, liturgy, doctrine, and ethics. The largest group are the orthodox (50%), the liberal subdenomination consists of 8% of the church members and the mixed group of 20%.
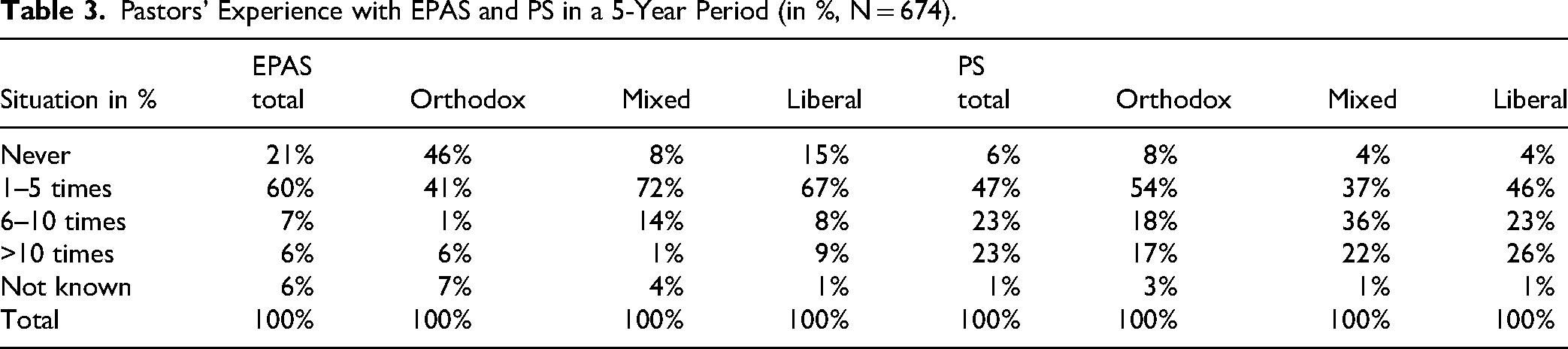
Regarding the pastors’ experience, we asked them on a four-point scale (never, 1–5, 6–10, >10, unknown) in 2016 how many persons they counselled at the EoL and for how many of them that included EPAS or PS, respectively. Furthermore, we investigated on a four-point scale with how many patients there had been contacts during the past 5 years about EPAS and PS (never, 1–5, 6–10, >10, unknown).
Questions about the attitude of the pastor regarding EPAS and PS included: 1) whether EPAS should be limited to terminal diseases only, 2) the Biblical perspective about EPAS and PS, and 3) whether they thought that the Bible offered sufficient guidance to formulate a personal perspective on EPAS and PS.
Analysis
In the analysis the answers to questions on the pastors’ attitude towards PS were related to both their viewpoint on the acceptability of EPAS and to their subdenominations. In our exploration and classification of the difficulties and challenges reported by pastors in the context of PS, we used the method of concept mapping (Kane & Trochim, 2007). Analysis of the EPAS-data, plus a full explanation of the method of concept mapping, can be found in Graafland et al., 2023a.
Results
General Data Respondents.
Degree of Experience with EPAS and PS as Related to Subdenomination (Research Question 1)
Pastors’ Experience with EPAS and PS in a 5-Year Period (in %, N = 674).
What Problems do Pastors Experience About PS in Their Pastoral Practice? (Research Question 2)
For the question, ‘Which difficulties or dilemmas did you experience during your pastoral care with regard to medical interventions at the EoL?’ we received more than 600 responses, 33 of which related to PS. Many of the difficulties reported with PS are of a more practical nature than those related to EPAS (Graafland et al., 2023a), but nevertheless influenced their pastoral care. The difficulties regarding PS influencing the pastoral care process can be clustered as follows:
The time course. Sometimes PS is experienced as occurring too quickly, especially in the case of a sudden deterioration of the patient's condition, leaving the patient with little-to-no time for necessary arrangements and farewells. On other occasions PS lasts too long and exhausts the next-of-kin and the caregivers. The doctor is sometimes pressured by the next-of-kin to ‘intervene’ (which, in practice, means to speed up the dying process). Little communication between the patient and those close to them. This also has two sides: some patients are being sedated without informing their relatives; and some relatives may ask the doctor to sedate their loved one without his or her knowledge or consent. There is also often a lack of communication between the patient and doctor and between the pastor and doctor, resulting in pastors feeling trapped. A sudden initiating of PS may come as a surprise to the pastors, so they must drop what they are doing to say farewell to a dying parishioner: ‘you must come now, the patient wants to speak to you first, you are a man of God.’ PS sometimes develops differently than expected. Not only may it take longer (see 1 above), but also may a patient wake up unexpectedly. Both can be experienced as hard for next-of-kin, caregivers, and pastors. With the continuous form of PS, just like in EPAS, farewells are said: the patient's biographical life comes to an end. This can cause confusion among patients, relatives, and the pastor. Those involved may ask, “Is PS not another form of EPAS”? Or, conversely, “Why does the patient receive PS rather than the desired EPAS?” Pastors experiencing their parishioners’ doubts about whether PS is allowed by God or the Bible.
Pastors’ Attitude Towards PS (Research Question 3)
In a prior study (Boer et al. 2020), we found that according to 59% of pastors EPAS is not incompatible with a Christian worldview but with great differences between the subdenominations: orthodox pastors (86%) are considerably more critical than their liberal colleagues (16%). We found here that this has in part to do with a more conservative reading of the Biblical material. In comparison, the overall acceptance of PS among pastors is much higher – around 90%. Remarkably, however, a pastor's subdenomination, age and years of work experience seem to be of much less importance here (
Moral Questions About EPAS and PS.

The Role of the Bible in Pastors’ Attitudes Towards EPAS and PS, and Parishioners Asking About the Biblical Perspective (Research Question 4)
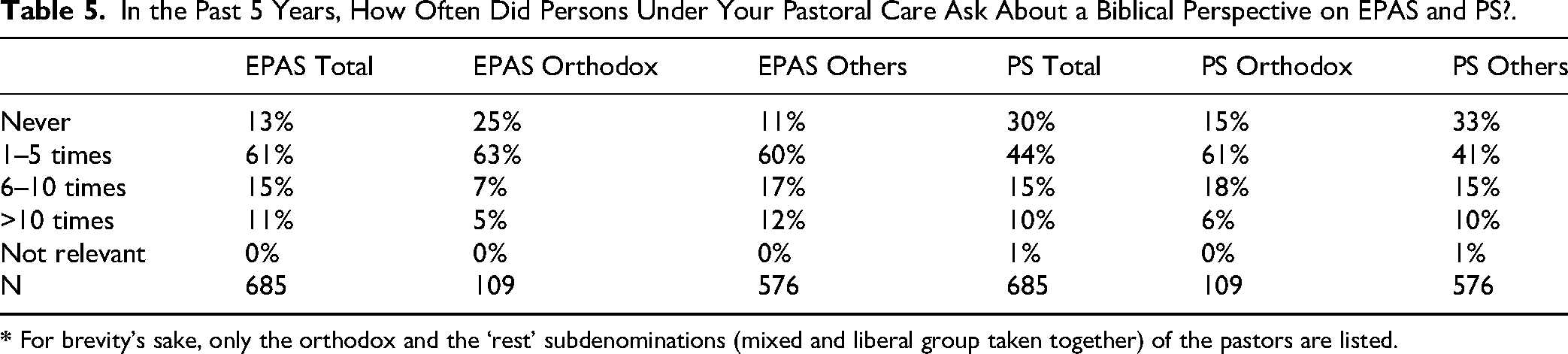
Pastors are generally more often asked about a biblical perspective on EPAS than on PS (
In the Past 5 Years, How Often Did Persons Under Your Pastoral Care Ask About a Biblical Perspective on EPAS and PS?.
Discussion
In this empirical study, the experiences of Protestant pastors with PS are presented and compared with their experiences with EPAS. The comparison between these two types of medical decisions at the EoL is made because despite their different objectives in medical and pastoral practice, they have many similarities and can come close to each other. Interestingly, pastors’ attitudes towards both actions differ considerably.
Summary of the Results
Pastors have frequent encounters with PS and the number of encounters shows little difference in subdenomination, age, and years of experience. We found a high level of moral acceptance (90%) of PS with no differences based on background characteristics. More than twice as many orthodox pastors receive questions about PS than their more liberal colleagues. This suggests that orthodox church members are more hesitant about PS and have more questions about it.
In the answers to the open-ended question about difficulties experienced in PS, we discerned seven clusters that can be categorized in three categories: First, the suddenness of PS was mentioned. This may be due to the patient's worsening condition together with a lack of communication between the doctor and the pastor. A pastor may have to drop everything to see their parishioner a last time. Secondly, pastors mention the confusion among patients’ relatives about the difference between PS and EPAS. In particular, they mention the family's expectation that the patient would receive EPAS instead of the applied PS. In one way or another, communication between doctor, patient, family, and other health care providers failed. Finally, the long duration of PS may be a burden on relatives, and professionals (including the pastor). This may be because all parties were not sufficiently informed about the potentially long duration of PS.
The Great Moral Acceptance of PS by Pastors
PS has earlier been referred to as ‘terminal sedation’ (Enck, 1991) but to avoid the suggestion that it shortens the patient's life, ‘terminal sedation’ was gradually replaced by the term ‘palliative sedation’ (Broeckaert, 2000). Still, in a certain sense the concept of PS can be said to be a euphemism. First, a patient who is deeply and permanently sedated loses consciousness, can no longer communicate with their loved ones, and can no longer experience the end of their life. Secondly, as Den Hartogh (2023) argues, the attempt by some to stress the differences between EPAS and PS as strongly as possible may be misleading. Although it is conceptually possible to distinguish between EPAS and PS (See the differences in Table 1), in practice the boundaries are sometimes blurry. Both interventions aim to intervene in the suffering of the patient: EPAS by ending a life, PS by inducing a deep sleep, in which a patient usually dies within days or (rarely) weeks (Rietjens et al., 2008; Van der Heide, 2012).
Whereas EPAS in the Dutch context is seen as an extraordinary medical intervention regulated by the Euthanasia Act, PS features as an ‘ordinary’ medical intervention. The guidelines issued by the Royal Dutch Medical Association (RDMA) are not legally binding allowing physicians to decide based on their professional discretion. Despite the increasingly important role of patient autonomy, EPAS and PS seem to be primarily based on compassion by ending suffering that is perceived as unbearable. The important difference is that in EPAS the doctor kills the patient or assists them in suicide whereas in PS the patient theoretically dies from an illness. The RDMA-guidelines include a maximum life expectancy of fourteen days, in combination with the advice to refrain from administering nutrition and hydration. According to Van Delden (2013), in sedation that lasts longer than a few days deprivation of fluids will shorten life. Some physicians and ethicists regard this earlier death as an acceptable side effect, others see this as crossing a moral line regarding it as ‘slow euthanasia’ (Den Hartog, 2023). In addition, it is very hard accurately predicting a patient's life expectancy. All this could therefore mean that in an unknown (but possibly significant) number of cases we should also see PS as a form of active termination of life and often without request.
If PS is indeed sometimes a form of active life termination, pastors’ high acceptance of PS compared to EPAS is striking, although perhaps not surprising. Worldwide, PS has featured as an accepted EoL intervention (Gurschick et al., 2015; Twycross, 2019), if there are refractory symptoms. This is true in countries both with and without legislation on assistance in dying. Two ethical themes play an important role in this discussion. The first is the question of what type of suffering may justify PS. The deep continuous form of PS – CSD – is used to control refractory symptoms such as pain, shortness of breath and delirium in patients whose natural death is imminent. In many of these patients, however, even existential motivations such as meaninglessness, lack of perspective, and loneliness may play a role (Den Hartogh, 2023). Just like in EPAS, the question in PS is to what extent such non-physical suffering may be a factor. In the literature we find two positions: the categorical rejection of existential suffering as an indication for PS (Anneser, 2018; Bozzaro, 2018; Ciancio et al., 2019; Kamprad & Helm, 2018; Miccinesi et al., 2017; Rodrigues et al., 2018), and the view that existential suffering under certain conditions can justify PS (Voeuk et al., 2017). One such condition is to first explore alternative forms to ease the suffering, another one to consider applying an intermittent form of sedation before resorting to PS (KNMG, 2022).
A second question is how to deal with the moral grey area between EPAS and PS. Many of those who are critical of EPAS also reject the CDS-version of PS –- deep continuous sedation until death in combination with withholding nutrition and fluids, the so called ‘dual procedure’ (den Hartogh, 2016). Only intermittent sedation combined with fluid administration is an option for them. Others do consider CDS to be justified and consider any life-shortening effect justifiable, per the ‘principle of double effect’.
It is therefore remarkable that relatively few pastors express serious ethical concerns with regarding PS (with most of their questions being of a more practical nature). Are pastors aware of the overlap, the sometimes blurred boundaries and other ethical questions surrounding PS? Could it be that, from their often-critical attitude toward EPAS, pastors are inclined to embrace PS more easily without being aware – or wanting to be aware – of critical ethical questions that can be asked about PS as well?
What Does This Mean for Pastoral Practice?
Both EPAS and PS result in the patient's biographical life ending at a self-selected moment. The interaction between pastor and parishioner ends here. EPAS often involves longer preparations, in part because it must be extensively accounted for after the fact. However, PS, is more often initiated on short notice. Sometimes a pastor is expected to drop everything to be in time to say farewell to the parishioner. The urgent nature of PS is also reflected by the pastors’ responses to our questions. It requires good communication and flexibility on the part of the pastor. Looking deeper into pastoral contact with a patient at the EoL, it is important to decide at what point the pastor enters the picture, as this affects the content of the relationship. Ideally, a pastoral relationship should start well before the onset of an illness or at least start when a life-threatening illness is diagnosed. In the weeks and months following, questions can be discussed about the meaning of suffering and its place in the in the person's life. Additionally, a conversation can be held between the pastor and the patient about whether medical interventions such as EPAS or PS are an acceptable and necessary response to the suffering. Our research shows that many parishioners want to be informed about their pastor's own views and the possible Biblical perspectives both about EPAS and PS. Questions of faith and theology can then be discussed within this pastoral context. Both the pastor and parishioner parties can bring their doubts and personal views to the discussion and see where it leads them. When the pastor's involvement begins (much) later and closer to the EoL, pastor and parishioner have no prior relationship to build on. This may turn the pastor into a ‘service provider’ who is focused on the immediate needs of the patient or their family. This can be unsatisfying and sometimes frustrating for the pastor because he may be excluded from important existential matters and instead is confronted with accomplished circumstances. Earlier research (Boer et al., 2019 and 2020) revealed, for example, that not all pastors are informed about the involvement of EPAS or PS. It is therefore important for the pastor to understand in advance where his boundaries lie. Especially when it comes down to how someone would prefer to die (natural versus EPAS or PS), the question is whether the manner of death is influential for the fulfilment of pastoral-ritual duties.
There is also the substantive question about the role the parishioner's own views have in the pastoral encounter regarding EPAS and PS. What prompted the patient to choose EPAS or PS and what aspects of this are relevant for the pastor to address? Finally, what is the pastor's role when he disagrees with the parishioner's choices.
The Pastoral Encounter at the EoL
The pastoral encounter (Mak, 2017; Ganzevoort & Visser, 2018; Heitink, 1998; Menken & Meulen, 2007) takes place between a pastor and his parishioner but it is more than that: “Instead of being simply a dialogue, a trialogue comes into being” (Oates, 1974). The pastoral encounter differs from the conversations between patients and other care providers because there are existential and spiritual dimensions to it. In one way or another the pastor also represents God, Christ, and the Church.
Ideally, pastoral encounters around the EoL, with all the complexities involved in such encounters, do not start when a patient is close to death. Beforehand pastors should convey that they are able and willing to engage in a balanced, open and respectful interaction. This competence not only includes sufficient knowledge about the practical and moral aspects surrounding EPAS and PS but also openness about the pastor's own views and the limitations of those views. During their interactions, parishioners may feel free to share their fears when thinking about the EoL including concrete fears of pain or distress, fears of disillusionment, shame, loss of dignity, becoming a burden to loved ones or society, as well as fears based on past experiences. The motivations for a desire for EPAS or PS cannot easily be lumped together. Giving words to implicit motives may help to avoid misunderstandings. A pastor may try to facilitate such a (potentially beneficial) openness by ‘playing devil's advocate’ and playing the (temporary) role of someone who does not understand. Religious ghosts from the past, such as the great fear of whether you are “saved” for eternity, can also play a role. A pastor who refers to what the Scriptures tell about the EoL (and beyond) may comfort and ease fears. Imagery about heaven and influential concepts such as sin and grace, judgment and forgiveness, being saved and doing penance may come into play. This is an open and respectful exchange between two ‘seekers,’ with both pastoral openness to the thoughts and faith of the parishioner, and clarity on the pastor's part about his own position when it comes to concepts such as mercy, love, autonomy, obedience to tradition, struggle and surrender. A pastor represents a tradition that believes humans are precious and beloved by God. This sets the tone for what pastors stand for and what space they can offer. When the decision has been made about EPAS or PS, it can be important to stay with the other person and play a role, such as giving a blessing, reading a poem or performing a small ritual. This will help others who are present, as well.
Limitations
Until now, Protestant pastors’ experiences with PS in the Netherlands have not been studied well, in contrast to their experiences with EPAS. In this study we fill this gap by comparing pastors’ attitudes toward EPAS with those toward PS by both quantitatively comparisons and qualitatively.
One limitation in our study is that survey questions with respect to EPAS were sometimes asked slightly differently than those about PS. In EPAS, for example, the question was “EPAS conflicts with my Christian convictions,” whereas for PS it read: “PS is morally acceptable to me.” Another limitation is that respondents were not asked how they valued PS and EPAS in relation to each other. Thirdly, the survey did not explicitly ask about difficulties in PS; instead, the difficulties surrounding PS were a “by-catch” of the responses about difficulties in EPAS.
Further Research
There is a clear need for qualitative in-depth research that explains the difference between pastors’ attitudes towards PS and EPAS – especially in the more orthodox segment, where the differences are the most pronounced. In-depth interviews with patients, relatives, caregivers and parishioners may provide a more comprehensive understanding. One hypothesis of such research would be: if pastors are better informed about the similarities between EPAS and PS and about the ethical discussions surrounding PS, would that change their position on PS and subsequently affect their pastoral care in such situations?
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.