
Abstract
Periodontal disease has been suggested to be an important risk factor for preterm low birthweight (PLBW). Here we report a case-control study of 236 cases (infants < 37 wks and weighing < 2499 g) and a daily random sample of 507 controls (≥ 38 wks and weighing ≥ 2500 g). Clinical periodontal indices were measured on the labor wards. Associated risk factors for periodontal disease and PLBW were ascertained by means of a structured questionnaire and maternity notes. The risk for PLBW decreased with increasing pocket depth (odds ratio [OR] 0.83, 95% confidence interval [CI] 0.68 to 1.00). After adjustment for maternal age, ethnicity, maternal education, smoking, alcohol consumption, infections, and hypertension during pregnancy, this decreased further (OR 0.78, 95% CI 0.64 to 0.99). We found no evidence for an association between PLBW and periodontal disease. Our results do not support a specific drive to improve periodontal health of pregnant women as a means of improving pregnancy outcomes.
INTRODUCTION
The determination of risk factors for the delivery of preterm low-birthweight infants represents a major public health priority. In the United Kingdom, 6% of all live births are classified as low birthweight (under 2500 grams) and 6.7% as preterm low birthweight, that is, delivery before 37 weeks' gestation, usually as a result of premature labor or premature rupture of membranes. Fifty-nine percent of neonatal deaths are associated with preterm delivery and birthweight of under 1500 grams (Mortality Statistics, 1995). Birthweight is considered to be an important determinant of the chances of an infant to survive, grow, and mature (Nelligan et al., 1976; Barker, 1998).
Various factors have been associated with the delivery of preterm and/or low-birthweight infants. Maternal risk factors include age, height, weight, socio-economic status, ethnicity, smoking, alcohol, nutritional status, and stress (Kramer, 1987; Verkerk et al., 1993; Copper et al., 1996; Nordstrom and Cnattingius, 1996; Barker, 1998). In addition, parity, birth interval, previous complications, pre- and ante-natal care, maternal hypertension, infections, and cervical incompetence may also be important (Hillier et al., 1995; Lamont, 1998; Walker et al., 1998). However, a significant proportion of low birth-weight is of unknown etiology.
The role of infection is receiving increasing attention. For example, women with asymptomatic bacteriuria or abnormal colonization by pathogenic micro-organisms are twice as likely to deliver preterm infants as a result of spontaneous preterm labor, pre-labor rupture of membranes, and chorioamnionitis. The etiological role of maternal infection, either in the genital tract or elsewhere, on preterm delivery remains controversial but may be an indirect effect as a consequence of the production of increased levels of inflammatory mediators which shorten gestational age. It is also plausible that micro-organisms may gain direct access to the amniotic fluid and fetus in several ways: ascending via the vagina through the cervix into the choriodecidual sac during pregnancy, via the endometrium which may be chronically infected prior to pregnancy, or alternatively through a hemotogenous route (Romero and Mazor, 1988; Taylor et al., 1997; Brocklehurst, 1999).
The hypothesis that infection remote from the fetal placental unit may influence PLBW has led to an increased awareness of the potential role of chronic bacterial infections elsewhere in the body. Periodontal disease is associated with a chronic Gram-negative infection of the periodontal tissues which results in long-term local elevation of pro-inflammatory prostaglandins and cytokines (Page and Kornman, 1997) and an increase in the systemic levels of some of these inflammatory mediators (Page, 1991). Hence, periodontal disease has the potential to influence PLBW through an indirect mechanism involving inflammatory mediators or a direct bacterial assault on the amnion.
There is evidence of an association between periodontal disease, especially severe periodontitis, and a variety of systemic conditions. Among these are cardiovascular disease, including endocarditis and coronary heart disease, insulin-dependent diabetes mellitus, and respiratory disease (Seymour and Steele, 1998). The 1996 study by Offenbacher and colleagues suggested that maternal periodontal disease could lead to a seven-fold increased risk of delivery of a PLBW infant. Moreover, it has been observed in animal models that infection with Gram-negative periodontitis-associated micro-organisms may adversely affect pregnancy outcomes. Collins and co-workers (1994) reported that there was a 25% reduction in birthweight in pregnant hamsters challenged subcutaneously in the dorsal region with the periodontal pathogen Porphyromonas gingivalis, compared with normal healthy pregnant hamsters.
As pointed out by Offenbacher et al. (1996), these findings have enormous potential significance to risk assessment of PLBW, to oral health care during pregnancy, and potentially to health care costs associated with PLBW. The aim of the present study was to examine the relationship between maternal periodontal disease and preterm low-birthweight infants in a United Kingdom case-control population attending the Royal London Hospital.
MATERIALS & METHODS
Selection of Subjects
The study population was comprised of a multi-ethnic group of women from the East End of London, UK, who gave birth at the Royal London Hospital between January, 1997, and August, 1998. They lived mainly in the East London and City Health Authority situated in the North Thames region. Subjects were enrolled into a case-control study within 24 hrs of delivery at the Royal London Hospital, after giving informed written consent. The hospital birth register was scrutinized each day by the study team support members to identify all cases, defined as those mothers who delivered an infant weighing under 2500 g and born before 37 weeks' gestation. A random sample (selected according to random number tables) of up to four control mothers (those who delivered an infant weighing more than 2500 g and born after 38 weeks' gestation) was selected daily from the birth register at the same time as the cases. All mothers were eligible for the study, except those with congenital heart disease requiring antibiotic cover for invasive procedures, who had a multiple delivery, whose infants were stillborn, or whose infants did not fit either the “case” or “control” definitions (mainly because they were “small for dates”).
The study received ethical approval from the East London City Health Authority research Ethics Committee. Power calculations assumed a 3% prevalence of severe periodontal disease (defined as CPITN score 4) in the age range of 16-44 yrs (Todd and Lader, 1991). At a ratio of two controls to one case, 446 controls and 223 cases were required for detection of an odds ratio of 3 with 80% power at a 5% significance level. To allow for loss of power when controlling for confounding factors, we increased the ratio to 3:1 (Davenport et al., 1998).
Clinical Examination
The same dental clinician (CESW) who had been calibrated prior to the commencement of the study carried out all periodontal examinations, blind to case-control status. The maximum periodontal pocket depth (mm), level of inflammation of the periodontal tissues (based on bleeding index scored 0-3), and the Community Periodontal Index of Treatment Need (CPITN scored 0-4) were recorded for each tooth (Ainamo et al., 1988). Attachment loss (mm) was also determined for the 10 worst teeth for each subject. The examination took place on the maternity ward with the subject lying flat on her bed, head to the foot end of the bed to facilitate a reproducible examination position for the clinician. Illumination of the subject was by a single light source (DaRay lamp, Glover Supplies, Shrewsbury, UK) and periodontal examination by an Ash SE CPITN-C probe (Dentsply Limited, Weybridge, Surrey, UK) and a disposable pressure-sensitive probe (Vivacare TPS, Vivadent, Schaan, Liechtenstein), and a standard form as previously described (Davenport et al., 1998).
A convenience sample of 273 mothers was invited to attend a follow-up examination six weeks post-delivery. A further examination was carried out according to the same periodontal indices and performed by the same clinician (CESW).
Identification of Risk Factors
A dental therapist or an advocate (for Bengali-speaking mothers) administered a structured questionnaire after the clinical examination to ascertain risk factors for preterm low birthweight and periodontal disease (Williams et al., 2000). Care was taken to minimize the effects of bias by adherence to a strict protocol, since the interviewers were not blind to the status of the mother. These included details of tobacco consumption (past and present smoking and the chewing of paan with added tobacco), alcohol consumption, maternal general health during pregnancy, infections (including genito-urinary) and their treatment, dietary habits, dental treatment, level of education, ante-natal care (including use of iron tablets), and total number of pregnancies and live births.
Subjects' Hospital Maternity Notes were scrutinized by the dental therapist to recover as many pregnancy details of each mother as possible. The main information retrieved was maternal height, weight, blood group, serology, scans, and relevant medical history of the subject and family. Any infection (chest, genital, urinary, throat, head, and neck), type where known (streptococcal, staphylococcus, E. coli, yeast, anaerobic, chlamydia), and treatment received (antibiotics, antifungals) during the pregnancy were recorded. The outcome of previous pregnancies was recorded. Where feasible, details ascertained in the questionnaire were validated from the Maternity Notes. These included infection history, medications, ante-natal care, and alcohol and tobacco use. Further validation of tobacco use was carried out on a subsection of the study group (291 mothers) by determination of cotinine in stimulated whole-mouth saliva, as described by Feyerabend and Russell (1990), which demonstrated very good agreement with the self-reported data. These findings will be presented in a subsequent manuscript.
Statistical Analysis
Data were stored in a relational database (Microsoft AccessTM) and analyzed by means of Stata version 6.0 (Stata Corporation, College Station, TX, USA). For each subject, we calculated the mean values of the pocket depth, CPITN index, and bleeding index for all teeth present. We used logistic regression to estimate associations between case-control status and these measures of periodontal disease severity. Analyses were controlled for the effects of variables considered a priori to be likely confounders of the association between PLBW and periodontal disease (maternal age group and ethnic group) plus those whose association with PLBW in univariable analyses had a P value of less than 0.1. Analyses were repeated after the exclusion of cases resulting from (elective or emergency) Caesarean section or induced births, because these were more likely to have a defined etiology. We examined the shape of the association between log odds of PLBW and mean pocket depth using generalized additive models (Hastie and Tibishirani, 1990).
RESULTS
A total of 236 cases and 507 controls was recruited into the study; 17 mothers declined to participate. The mean age of cases (26.7 yrs) was similar to that of the controls (26.9 yrs). Table 1 shows the distribution of demographic features of the study population and risk factors for periodontal disease, among cases and controls. The majority of mothers were Bengali (52.5%), did not have tertiary education (60.1%), and were in the 20- to 29-year age group (61.0%). A third of the subjects were first-time mothers, and approximately 10% had had five or more previous pregnancies. Those factors most strongly associated with PLBW were hypertension during pregnancy (odds ratio [OR] 3.23, 95% CI 2.05 to 5.10), previous delivery of a LBW infant (OR 2.53, 95% CI 1.68 to 3.80), and smoking during pregnancy (OR 2.15, 95% CI 1.20 to 3.88), in comparisons of mothers who smoked ≥ 10 cigarettes/day with mothers who did not smoke. There was evidence that increasing levels of education were associated with a decreased risk of PLBW (OR per group 0.82, 95% CI 0.65 to 1.02, P for trend = 0.072).
Of the 743 mothers, all except five had 21 or more teeth (excluding wisdom teeth). Those with fewer were two case mothers with 14 and 16 teeth, respectively, one control with 19 teeth, and two controls with 20 teeth each. There was a high level of periodontal disease: 44% of the mothers had at least one sextant with CPITN = 4.
A total of 50 mothers attended follow-up examinations 6 wks post-delivery. Table 2 shows that there were strong correlations between mean pocket depth measured on the labor ward and mean pocket depth and attachment level 6 wks post-delivery. As expected, reduction of pregnancy-associated gingivitis led to a reduction in mean pocket depth at 6 wks (average reduction 0.23 mm, 95% CI 0.13 mm to 0.33 mm) and attachment level (0.19 mm 95% CI 0.07 mm to 0.31 mm).
Table 3 shows mean periodontal status for case and control mothers, together with results of logistic regression analyses which examined the association between periodontal status and PLBW. There was no evidence for an association between increasing levels of periodontal disease and increased risk of PLBW. Indeed, there was evidence for an inverse association between subjects' mean pocket depth and PLBW (OR 0.83, 95% CI 0.68 to 1.00). Controlling for maternal age, ethnic group, maternal education, smoking, alcohol consumption, number of infections during pregnancy, and hypertension during pregnancy made little change to this result (OR 0.79, 95% CI 0.64 to 0.99). When 70 cases whose births were induced were excluded from the analysis, a similar relationship was also found (OR 0.87 (95% CI 0.69 to 1.11). Similarly, excluding 45 mothers who were diabetic made little difference to the results (data not shown). The Fig. shows the relationship between the log odds of PLBW and mean pocket depth, estimated by means of a generalized additive model with 3 degrees of freedom (Hastie and Tibishirani, 1990). There is a general tendency for decreasing odds of PLBW with increasing mean pocket depth. In particular, we found no evidence for an increase in the odds of PLBW among mothers with the greatest mean pocket depth. We found no evidence that increasing levels of periodontal disease were associated with an increased risk of PLBW in analyses which examined Bengali and White mothers separately.
DISCUSSION
This large case-control study has found no evidence that maternal periodontal disease is associated with an increased risk of premature low-birth-weight (PLBW) births. Indeed, we found evidence that increasing mean pocket depth at the time of delivery was associated with a reduction in the risk of PLBW.
In any case-control study, it is important to avoid selection bias and to control for confounding. Our study was conducted among a well-defined population (mothers giving birth at a particular hospital), and almost all mothers agreed to participate in the study. We selected control mothers randomly from among those present on the ward at the time that cases were recruited. We can therefore be confident that selection biases have not influenced our results. Our analyses also controlled for known confounding variables: We confirmed several of the well-known risk factors for PLBW, including hypertension, tobacco and alcohol use, and previous PLBW.
In studies of clinical periodontal disease, a great many potential measures of disease severity are available. Our choice of periodontal indices was essentially determined by the need to carry out the clinical examination on the ward. CPITN (Ainamo et al., 1982) was seen to provide the most appropriate screening system for the chosen setting. However, we think it unlikely that different choices of outcome would have produced different results. For example, one alternative would have been to concentrate on the deepest pockets, or most inflamed sites. The correlations between mean pocket depth for all teeth and mean depth of the 6 deepest pockets was 0.88, while the correlation between mean bleeding index and mean index for the 6 most inflamed teeth was 0.80, so that analyses according to these alternative outcomes give conclusions similar to those presented here. Another possible criticism is that we measured levels of periodontal disease at a time when these are increased by pregnancy-associated gingivitis. However, we have shown that mean pocket depth is strongly correlated with mean pocket depth and attachment level 6 wks post-delivery.
Few data are available to have enabled the level of periodontal disease in our particular study population to be predicted. It has been reported that 70% of all women, and especially those of child-bearing age, resident in the United Kingdom have some periodontal pockets, but the majority of these are shallow (Todd and Lader, 1991). Our study demonstrated that 44% had at least one sextant displaying CPITN 4, corresponding to severe periodontal disease. However, Miyazaki et al. (1991) reported that 31% of the pregnant women in a Japanese population had periodontal pockets of 4 or 5 mm, results similar to the data in the present work.
Meanwhile, the etiology of preterm birth remains poorly understood. Genito-urinary infections have been implicated as a main risk factor in 15 to 25% of preterm deliveries (Minkoff et al., 1984; Romero and Mazor, 1988; Brocklehurst, 1999). Despite genito-urinary infections generally responding to treatment with metronidazole, erythromycin, and or clindamycin (Hauth et al., 1995; Joesoef and Schmid, 1995), this has not always resulted in a reduction in preterm birth rate, except for women with a previous history of preterm birth (McDonald et al., 1991; Brocklehurst, 1999).
Differences between the study populations in our study and that of Offenbacher and colleagues include ethnic mix and age. The North Carolina study consisted of 124 women who were slightly younger on average, especially the cases (22 yrs old). Fifty-eight percent were Black, and the subjects were drawn from the Prenatal Care Clinic or within three days postpartum and then examined in a research dental clinic. Our study was much larger (743 women), and subjects were recruited from a predominantly Bangladeshi (53%) community residing in East London. We believed that it was important to recruit mothers prior to their discharge from hospital, to avoid losing them because of family commitments. We think it unlikely that differences between the study populations are the main explanation for the differences between the results of our study and that of Offenbacher et al. We know of no a priori hypothesis which suggests that an association between periodontal disease and premature low birthweight would be found in particular ethnic groups, and we found no evidence of such an association when we examined the major ethnic groups in our study separately. As outlined earlier, there remain several plausible biological mechanisms through which periodontal disease could cause PLBW, perhaps in the presence of other specific genetic and environmental factors. A clearer understanding of these mechanisms would be helpful in the design of future studies.
It is noteworthy that reported associations between periodontal disease and the risk of coronary heart disease have not been confirmed consistently in subsequent, larger studies (Seymour and Steele, 1998). As noted by Hujoel et al. (2000), failure to control adequately for potential confounding factors may be one reason for inconsistencies between the results of different studies. If associations between periodontal disease and other diseases are more moderate than had been thought, then large, well-controlled epidemiological studies will be needed to study these issues, and randomized trials of treatment of periodontal disease may be necessary to establish causal relationships.
While we cannot explain the inconsistency between studies, our results exclude any substantial association between clinical indices of periodontal disease and premature low birthweight. The United States National Institutes of Health has reported that up to 18% of preterm low birthweight may be attributed to periodontal disease, which may thus account for a significant proportion of the $5.5 billion annual hospital costs associated with care of small babies. Our results suggest that it is unlikely that maternal periodontal disease accounts for a substantial proportion of the costs of premature baby care in the United Kingdom, and that these initial estimates from the USA may be too high.
In conclusion, this study finds no association between any of the clinical measures of maternal periodontal disease and PLBW infants. While it remains important for health care workers to promote good oral health, our results do not support a specific drive to improve the periodontal health of pregnant women as a means of improving pregnancy outcomes. It would seem that it is not necessary to target women of child-bearing age who exhibit periodontal disease with any additional oral hygiene measures other than those generally applied during pregnancy.
Demographic Details of Study Population Including Main Risk Factors
Correlations between Mean Pocket Depth and Mean Attachment Level, Measured on the Labor Ward and at Six-week Follow-up
Association between Premature Low Birthweight and Measures of Periodontal Status
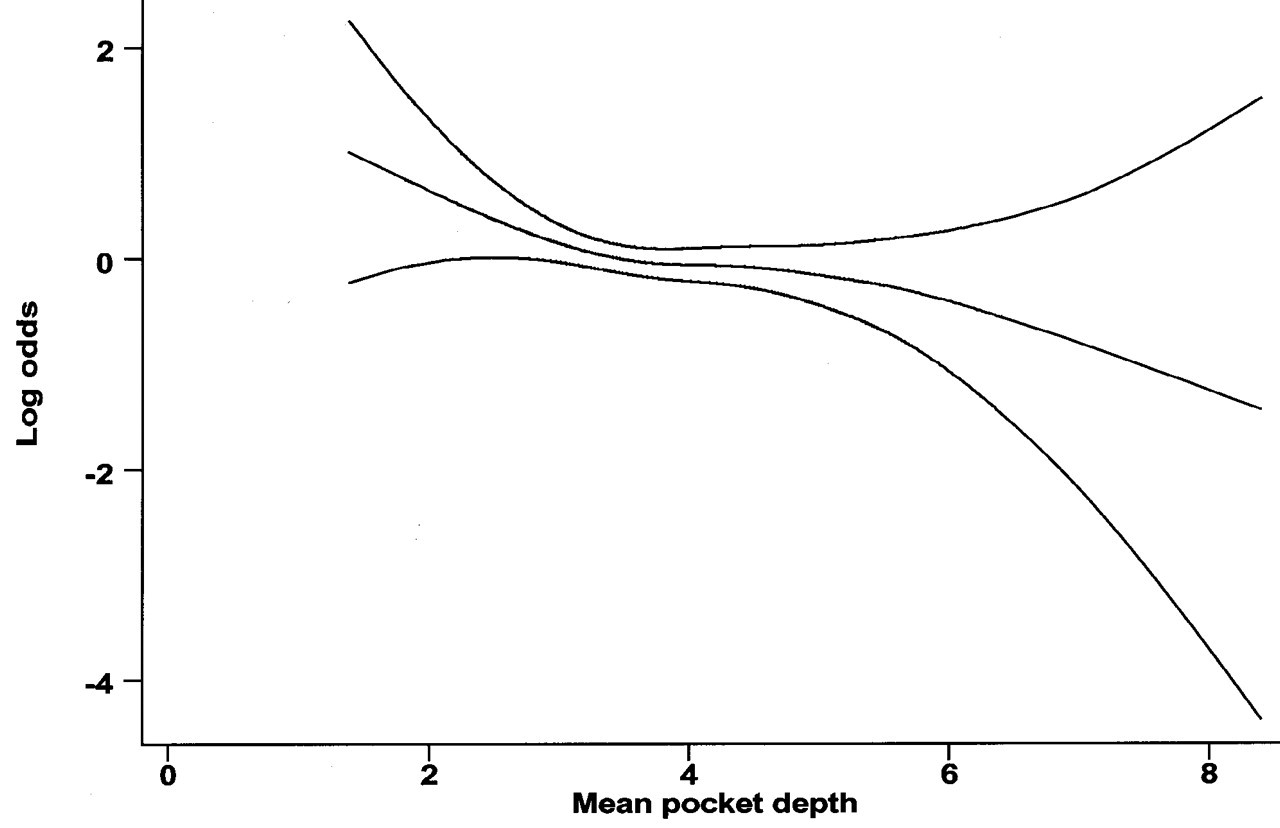
Relationship between increasing mean pocket depth and log odds of periodontal disease, estimated based on a generalized additive model with 3 degrees of freedom.
Footnotes
Acknowledgements
Ms. D. Eustace and Ms. B. Purkayastha assisted with the clinical examinations. We acknowledge the advice of Professor F. Hughes on the periodontal measurements and thank the staff of the Women's Services Unit of Barts and the London NHS Trust for their contribution to the study. The study was funded by the NHS Executive Research and Development Programme, Mother and Child Health, MCH 5-54.