
Abstract
Casein phosphopeptide-amorphous calcium phosphate (CPP-ACP) slows the progression of caries and remineralizes enamel subsurface lesions. The aim of this study was to determine the ability of CPP-ACP to increase the incorporation of fluoride into plaque and to promote enamel remineralization in situ. Randomized, double-blind, cross-over studies involved mouthrinses and dentifrices containing CPP-ACP and fluoride. The mouthrinses were used for 60 sec, three times/day for 5 days, and supragingival plaque was collected and analyzed for F. The dentifrices were rinsed as a water slurry for 60 sec four times/day for 14 days in an in situ model. The addition of 2% CPP-ACP to the 450-ppm-F mouthrinse significantly increased the incorporation of fluoride into plaque. The dentifrice containing 2% CPP-ACP produced a level of remineralization similar to that achieved with a dentifrice containing 2800 ppm F. The dentifrice containing 2% CPP-ACP plus 1100 ppm F was superior to all other formulations.
INTRODUCTION
Fluoride-containing dentifrices and mouthrinses have been demonstrated to decrease caries experience significantly in randomized, controlled clinical trials (Biesbrock et al., 2001; Marinho et al., 2003). The efficacy of these oral care products has been attributed to their ability to incorporate fluoride ions into plaque and enamel, since several investigators have suggested an inverse relationship between plaque fluoride levels and caries incidence (Duckworth et al., 1992; Hartshorne et al., 1994; Lynch et al., 2004).
Fluoride ions in plaque immediately promote the formation of fluorapatite in the presence of the calcium and phosphate ions produced during demineralization of tooth enamel by plaque bacterial organic acids (ten Cate, 1999). This is now believed to be the major mechanism of fluoride action in preventing enamel demineralization (ten Cate, 1999; Lynch et al., 2004). However, fluoride ions can also promote the remineralization of previously demineralized enamel if salivary or plaque calcium and phosphate ions are available in adequate amounts when the fluoride is applied. For every 2 fluoride ions, 10 calcium ions and 6 phosphate ions are required to form one unit cell of fluorapatite [Ca10(PO4)6F2]. Hence, on topical application of fluoride ions, the availability of calcium and phosphate ions can be limiting for net enamel remineralization to occur, and this is exacerbated under xerostomic conditions.
Casein-phosphopeptide-stabilized amorphous calcium phosphate nanocomplexes (CPP-ACP) have been demonstrated to have anticariogenic activity in laboratory, animal, and human experiments (Reynolds et al., 1995, 2003; Shen et al., 2001; Iijima et al., 2004; Morgan et al., 2008). Casein phosphopeptides (CPP) containing the cluster sequence –Ser(P)-Ser(P)-Ser(P)-Glu-Glu- stabilize amorphous calcium phosphate in metastable solution (Cross et al., 2005).
The CPP-ACP nanocomplexes have been shown to reduce caries activity in a rat caries model, with CPP-ACP and fluoride exhibiting a synergistic effect (Reynolds et al., 1995). CPP-ACP also has been demonstrated to increase the levels of calcium and phosphate ions significantly in supragingival plaque, and to promote the remineralization of enamel subsurface lesions in situ (Reynolds et al., 2003). The synergistic effect of CPP-ACP and fluoride in reducing caries experience may be attributable to the formation of CPP-stabilized amorphous calcium fluoride phosphate (Cross et al., 2004), resulting in the increased incorporation of fluoride ions into plaque, together with increased concentrations of bioavailable calcium and phosphate ions.
The aim of the current study was to determine the ability of CPP-ACP in the presence of fluoride ions to increase the incorporation of fluoride into supragingival plaque and subsurface enamel, and to promote enamel remineralization in situ with acid-resistant mineral.
MATERIALS & METHODS
Participant Recruitment
The study was approved by The University of Melbourne Human Research Ethics Committee, and informed written consent was obtained from all participants. Fourteen healthy participants (seven males and seven females) were recruited from the staff and students (age 21 to 45 yrs) of the School of Dental Science. An intra-oral examination confirmed that each had at least 22 natural teeth, with no current caries activity, periodontal disease, or other oral pathology. None of the participants was using antibiotics or medications. The studies were conducted in Melbourne, with the reticulated water fluoridated at 1 ppm.
Plaque Fluoride Study
The plaque fluoride study was a randomized, double-blind, three-way cross-over design involving 3 coded mouthrinses: (i) 2% w/v CPP-ACP (RecaldentTM, CASRN 691364-49-5) as supplied by Recaldent Pty Ltd (Melbourne, Australia) and 450 ppm F as NaF in de-ionized water; (ii) 450 ppm F as NaF in de-ionized water; and (iii) a placebo control rinse as de-ionized water. The rinses were adjusted to pH 7.0. Participants were supplied with the coded rinses in opaque plastic tubes and used 15 mL of each rinse for 60 sec 3 times a day—after breakfast, after lunch, and at night before sleeping—for 4 days; they kept a diary of mouthrinse use. On the fifth day, the rinse was used after breakfast, and supragingival plaque was collected 2–3 hrs later. Participants refrained from all oral hygiene procedures while using the rinses. Each participant crossed over to use each mouthrinse, with a four-week washout period between treatments. Supragingival plaque was collected from the buccal and lingual surfaces of all teeth and extracted as previously described (Reynolds et al., 2003). Fluoride ion concentration in the extracts was determined as described previously (Silva and Reynolds, 1996). The plaque fluoride levels were statistically analyzed by a non-parametric Friedman’s test with Wilcoxon Signed-ranks tests (Norusis, 1993).
Remineralization Study
A randomized, double-blind, five-way crossover remineralization study was conducted with 5 dentifrice slurries and an in situ appliance housing enamel slabs with subsurface lesions as previously described (Shen et al., 2001; Iijima et al., 2004). Dentifrices were prepared as coded products, and the base product contained sorbitol, silica, sodium lauryl sulphate, flavor, sodium carboxymethyl cellulose, titanium dioxide, xanthan gum, sodium saccharin, and water, pH 7.0. Five dentifrice formulations were prepared: (i) placebo, (ii) 1100 ppm fluoride as NaF, (iii) 2800 ppm fluoride as NaF, (iv) 2% CPP-ACP, and (v) 2% CPP-ACP plus 1100 ppm fluoride as NaF. Dentifrice slurries were prepared by the addition of 1 g of paste to 4 mL de-ionized water and vortex-mixing for 60 sec. Participants rinsed with the slurries for 60 sec 4 times per day for 14 days at the following times: 10:00 a.m., 11:30 a.m., 2:00 p.m., and 3:30 p.m. Participants were instructed not to eat or drink for at least 1 hr after each treatment. At the end of each treatment period, the enamel half-slabs were removed from the appliances and prepared for acid challenge as described previously (Iijima et al., 2004). The enamel half-slabs containing remineralized lesions and acid-challenged remineralized lesions were then paired with their control half-slabs containing the original demineralized lesions and embedded, sectioned, and microradiographed as described previously (Iijima et al., 2004). Microdensitometry was performed as described previously (Iijima et al., 2004). Data were statistically analyzed by repeated-measures ANOVA with a post hoc Scheffé test (Norusis, 1993).
Electron Microprobe Wavelength Dispersive Spectrometry
Enamel sections were embedded in epoxy resin on a specimen holder. The resin was flat-polished to expose the enamel sections and then further polished to optical smoothness. All samples and standards were coated with 20 nm of carbon by means of a Dynavac 300 (Dynovac Engineering Pty Ltd, Melbourne, Australia). The electron probe (8900R SuperProbe, JEOL, Tokyo, Japan) was operated at a 15 kV accelerating voltage, 12 nA specimen current, and 40° take-off angle. Fluoride x-ray intensities were measured by means of a spectrometer with a W/Si layered filter crystal. The standard was synthetic fluorapatite with a calcium-to-phosphorus ratio of 1.667 and a fluoride content of 3.70 wt%. Quantitative line scans for fluoride were collected across the enamel lesions, starting from the base of the lesion to the surface. The enamel fluoride levels were statistically analyzed by a one-way classification ANOVA with a post hoc Scheffé test (Norusis, 1993).
RESULTS
Plaque Fluoride Study
Both fluoride rinses produced an increase in plaque fluoride levels (Table 1). The 450-ppm-fluoride rinse produced a plaque fluoride level that was nearly double that obtained with the placebo control rinse (Table 1). The addition of 2% CPP-ACP to the 450-ppm-fluoride rinse significantly increased the incorporation of fluoride ions into plaque, where the plaque fluoride level was over double that obtained with the fluoride-alone rinse (Table 1).
Remineralization Study
All dentifrice formulations replaced mineral in the enamel subsurface lesions in the in situ study (Table 2). Fluoride produced dose-related remineralization, with the 2800-ppm formulation replacing significantly more mineral than the 1100-ppm formulation, which replaced significantly more than the placebo control (Table 2). The dentifrice with 2% CPP-ACP produced a remineralization level similar to that produced by the 2800-ppm-fluoride formulation, and the dentifrice with 2% CPP-ACP plus 1100-ppm fluoride was superior to all other formulations (Table 2). Microradiography of the lesions after remineralization revealed that fluoride ion alone tended to promote remineralization of the surface layer, whereas CPP-ACP promoted remineralization, even in the presence of fluoride, throughout the body of the lesion (Fig.).
Acid challenge in vitro of the in situ-remineralized enamel slabs resulted in substantial loss of mineral from the placebo-treated slabs (Table 2). The residual remineralization after acid challenge was significantly greater for the dentifrice containing 2% CPP-ACP plus 1100 ppm fluoride when compared with all other dentifrice formulations (Table 2). Microradiography of the remineralized lesions after acid challenge revealed that the acid removed mineral predominantly underneath the remineralized zone (Fig.). Fluoride incorporated into the lesions was significantly higher for the ’2% CPP-ACP plus 1100-ppm-F’ dentifrice when compared with that containing 1100 ppm F alone (Table 3). Further, the measured fluoride level for the ’2% CPP-ACP plus 1100-ppm-F’ dentifrice was close to that predicted based on the assumption that the remineralized mineral was fluorapatite (Table 3).
DISCUSSION
The CPP stabilizes clusters of calcium, phosphate, and hydroxide ions as amorphous nanocomplexes (Cross et al., 2005) and localizes these ions at the tooth surface (Reynolds et al., 2003). In a recent mouthwash study, it was shown that CPP-ACP significantly increased the level of calcium and inorganic phosphate ions in supragingival plaque, with the CPP bound to the plaque matrix and onto the surface of bacteria (Reynolds et al., 2003). The CPP incorporated into plaque had a half-life of 1–2 hrs, consistent with previous studies showing breakdown of the CPP by bacterial peptidase and phosphatase activities (Reynolds and Riley, 1989; Reynolds et al., 2003). The increase in plaque calcium and inorganic phosphate levels by the use of CPP-ACP supports previous results (Rose, 2000a,b) showing that CPP-ACP binds to a model plaque in vitro with twice the affinity of free calcium ions, providing a large calcium reservoir.
The CPP also stabilizes calcium, phosphate, and fluoride ions as amorphous nanocomplexes (Cross et al., 2004). Therefore, the current results are consistent with the formation of these CPP-ACP/F nanocomplexes in the mouth-rinse/dentifrice formulations or in the mouth on application of the formulations and the localization of the nanocomplexes at the tooth surface. The current studies show that not only did CPP increase fluoride incorporation into plaque, but it also increased the incorporation of fluoride into subsurface enamel and substantially increased remineralization of subsurface lesions of enamel compared with fluoride alone. The in situ remineralization study demonstrated a dose response between fluoride concentration and remineralization of subsurface enamel lesions, with the 2800-ppm-F dentifrice producing 89% greater remineralization than that produced by the 1100-ppm-F dentifrice. This result is similar to that obtained in a randomized, double-blind clinical trial of the anti-caries efficacy of fluoride-containing dentifrices (Biesbrock et al., 2001). In that study, the investigators showed that a 2800-ppm-F dentifrice reduced caries experience by 20.4%, which was an 85% greater reduction than that obtained with a 1700-ppm-F paste. Recently, in a randomized, controlled, double-blind caries trial, Morgan et al.(2008) showed that CPP-ACP in a sugar-free gum significantly slowed the progression of caries in an optimally fluoridated environment. In the in situ trial presented here, the dentifrice containing 2% CPP-ACP was superior to the dentifrice containing 1100 ppm F, and produced a level of remineralization similar to that achieved with the 2800-ppm-F dentifrice. However, the dentifrice containing 2% CPP-ACP plus 1100 ppm F was superior to all other formulations.
The addition of 2% CPP-ACP to the 1100-ppm-F dentifrice increased enamel subsurface remineralization by 156% relative to that produced by the 1100-ppm-F-alone dentifrice. The CPP-ACP also increased F uptake into the subsurface enamel lesion by 30% relative to the 1100-ppm-F-alone dentifrice. Interestingly, the fluoride uptake from the 1100-ppm-F dentifrice into the subsurface lesion was greater than that predicted from the amount of subsurface enamel remineralization observed. This result suggests that remineralization in the subsurface lesion with the 1100-ppm-F dentifrice was calcium- and/or phosphate-limited, such that not all the fluoride ions that diffused into the subsurface lesion were incorporated into a mineral phase. This excess fluoride would presumably stay as fluoride ions in the lesion fluid and perhaps be adsorbed onto crystallites, as has been proposed (Arends and Christoffersen, 1990).
These results highlight the importance of the availability of calcium and phosphate ions for net remineralization to occur when topical fluorides are applied. The presence of 2% CPP-ACP with 1100 ppm F in the dentifrice would have co-localized calcium and phosphate ions with fluoride ions at the tooth surface, presumably as CPP-ACP/F nanocomplexes (Cross et al., 2004). This increased concentration of calcium, phosphate, and fluoride ions at the tooth surface would drive diffusion into the enamel, producing higher activities of the ions in the subsurface lesion fluid, resulting in higher levels of remineralization and fluoride incorporation into the mineral phase. The analysis of the incorporated fluoride confirmed greater incorporation of fluoride in the presence of CPP-ACP and an incorporation very close to the level predicted if the mineral phase produced was fluorapatite. Acid challenge of the remineralized lesions confirmed the relatively lower solubility of the remineralized zone after remineralization with 2% CPP-ACP plus 1100 ppm F, also being consistent with the deposited mineral being fluorapatite.
Microradiography of the remineralized lesions demonstrated that the fluoride-alone dentifrices (1100 ppm F and 2800 ppm F) remineralized predominantly in the surface layer, whereas the 2% CPP-ACP dentifrice and the ’2% CPP-ACP plus 1100-ppm-F’ dentifrice produced a more homogenous remineralization throughout the body of the lesion. This result is consistent with the unstabilized nature of calcium, phosphate, and fluoride ions. At the enamel surface, when fluoride ions come into contact with free calcium and phosphate ions, fluorapatite would rapidly form in the surface layer. However, in the presence of CPP, which prevents rapid transformation of the calcium phosphate phases (Cross et al., 2005), the ions would be stabilized and maintained in a form that would drive diffusion down activity gradients into the subsurface lesion. Hence, the ability to deliver calcium, phosphate, and fluoride ions in the correct molar ratio deep into the subsurface lesion may be attributable to the ability of the CPP to localize and stabilize the ions at the tooth surface in the correct molar ratio [Ca:PO4:F = 5:3:1] (Cross et al., 2004).
In conclusion, these results suggest that ’CPP-ACP plus fluoride’ products may be superior in reducing caries risk compared with fluoride-alone products.
Fluoride Levels in Supragingival Plaque after Treatment with Various Mouthrinses
Percentage Remineralization of Enamel Subsurface Lesions by Various Dentifrice Formulations Followed by Acid Challenge
Predicted and Measured Fluoride Levels in the Remineralized Lesions
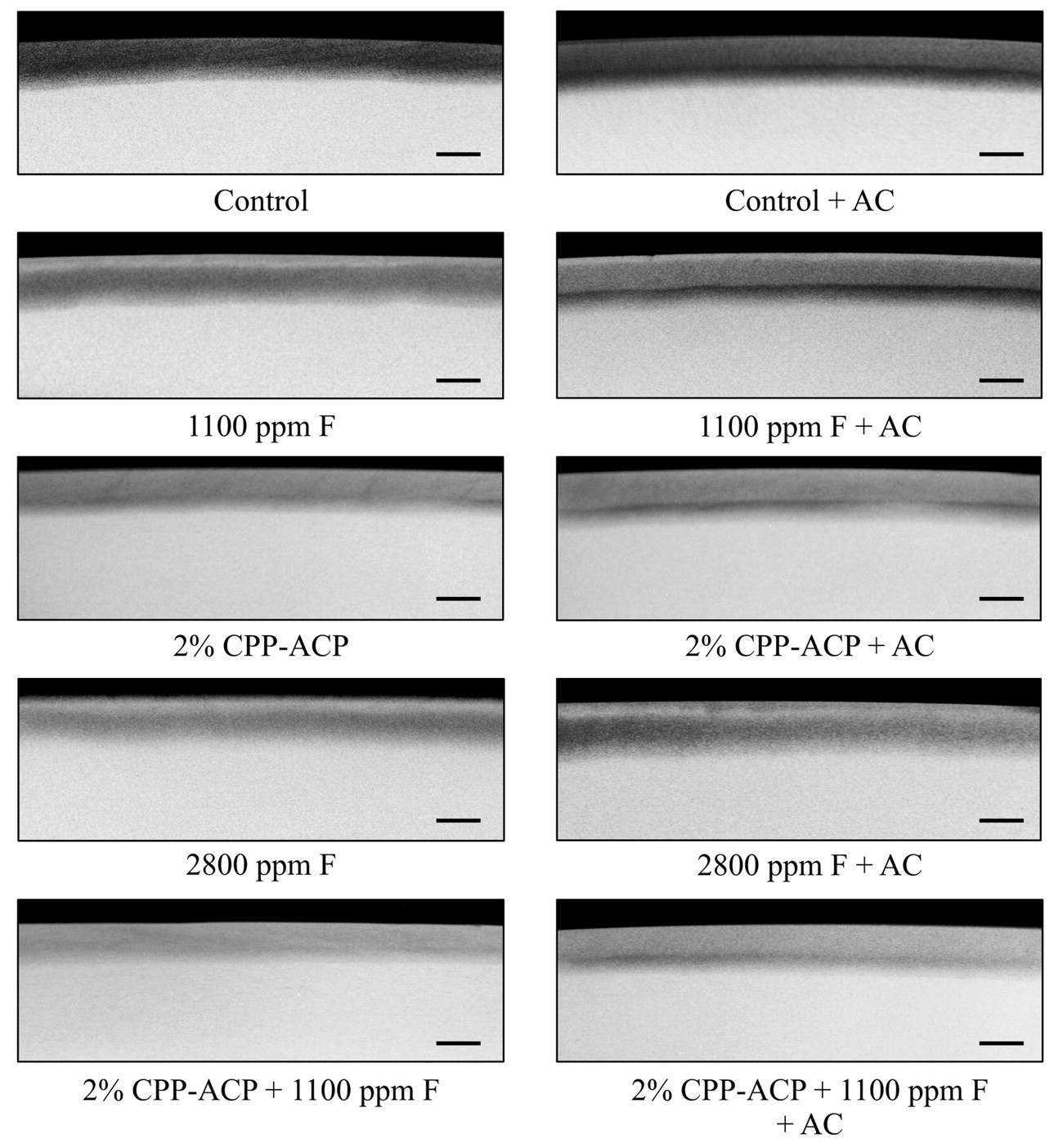
Representative microradiographs of enamel subsurface lesions after remineralization in situ and acid challenge (AC) in vitro. The scale bar indicates 100 μm.
Footnotes
Notes
Acknowledgements
This study was supported by the Australian National Health and Medical Research Council Project Grant 400299.