
Abstract
Introduction
Phlegmasia cerula dolens (PCD) is an uncommon complication of deep vein thrombosis (DVT), and involvement in the upper extremities is rare. We report a case in which color duplex ultrasound (CDU) was used to diagnose PCD in a patient with extensive upper extremity DVT.
Patient
A 57-year-old woman underwent an open lung biopsy. On the first postoperative day, she had right hand and forearm pain, edema, and cyanosis.
Findings
CDU revealedacute DVT in the right radial, ulnar, and brachial veins and extensive thrombosis of the right cephalic and basilic veins. Arterial signals recorded from the ipsilateral arteries were remarkable for pandiastolic flow reversal (PDFR). In contrast, arterial signals from the contralateral arm had a normal, triphasic pattern. Arteriography revealed patent arteries to the wrist and no flow present in the right hand.
Conclusions
This report demonstrates the sensitivity of CDU to arterial compromise associated with PCD in a case of upper extremity DVT. Vascular technologists should consider including arterial Doppler signals in their venous duplex protocols in cases of extensive deep and superficial vein thrombosis.
Background on Phlegmasia Cerula Dolens
Phlegmasia cerula dolens (PCD) is a devastating complication of deep vein thrombosis (DVT) that is associated with substantial morbidity and morality, including gangrene (50%), amputation (50%), and death (25%–48%). 1 Although PCD is estimated to complicate lower extremity DVT in 2%–10% of cases, it is rarely associated with DVT in the upper extremities. 2 Progression of PCD to gangrene in the upper extremities is exceptional; in fact, only 17 cases have been previously reported in the literature.2,3
The pathology of PCD is related to the total or near-total occlusion of venous drainage of an extremity that results in a rapid rise in venous pressure with resultant fluid extravastation into the tissues. In cases of lower extremity DVT, fluid losses as large as 6–10 liters leading to various degrees of shock have been reported in the literature. 4 The increase in venous pressure may reach 16–17 times the normal values, and the development of edema produces interstitial compartment pressures of 25–60 mmHg compared with a normal pressure of 0–10 mmHg.2,3 In PCD, hydrostatic pressure within the vessel falls caused by hypotension and tissue pressure increases because of edema, resulting in collapse of small arteries and distal ischemia. 4
Identification and treatment of this process in its earliest stages may avoid progression to gangrene. 3 At present, there are no parameters to measure the extent to which uncomplicated DVT begins to compromise arterial perfusion. Unfortunately, PCD is most often detected at its last stages when arterial Doppler signals are lost and irreversible tissue damage has occurred. 5 At present, the diagnosis of PCD is established by the clinical findings of edema, cyanosis, and pain in the presence of DVT. The symptoms of PCD are preceded by the more common uncomplicated DVT usually in the setting of one or more of the factors of Virchow's triad (hypercoagulability, venous stasis, and trauma). In PCD, the edema is usually massive, and the extremity will have a firm, tense quality. The pain experienced by the patient is agonizing but is usually less severe than that seen in primary arterial insufficiency. Cyanosis is present, beginning as a purplish hue to the skin starting distally and progressing proximally. This feature can be distinguished from arterial insufficiency by the presence of pulses, although they may be difficult to palpate because of edema.4,5
Unlike uncomplicated DVT, there is no standardized treatment for PCD. Steep limb elevation, anticoagulation, vasodilators, sympatholitics, sympathectomy, thrombolitic therapy, venous thrombectomy, fasciotomy, and amputation have all been reported. 6 The goal of treatment in all cases is to prevent embolization, thrombus propagation and to decrease compartment pressures, so arterial perfusion can be restored.
Case Report
A 57-year-old woman with systemic lupus erythematosus and a known hypercoagulable state underwent an uneventful open lung biopsy. Before surgery, her coumadin therapy was discontinued to allow sufficient time for her coagulation factors to fall within normal levels. On the first postoperative day, the right-hand IV site became infiltrated, and the catheter was removed. At this time the hand was noted to be swollen and cyanotic, and the patient reported difficulty moving her fingers. The radial pulse was palpable.
The patient was examined with CDU. On the right, the internal jugular, subclavian, and axillary veins were compressible and contained normal pulsatile flow patterns associated with upper extremity and central veins. In the brachial vein at the level of the antecubital fossa, nonocclusive thrombus was noted. The radial and ulnar veins were acutely dilated and noncompressible throughout their course, and there were no recordable spectral Doppler signals from either vein. Additional survey of the superficial system revealed occlusive thrombus in the cephalic and basilic veins extending from the wrist to the shoulder. On the left, the CDU examination was normal.
Spectral Doppler signals recorded from the arteries of the right arm revealed an abnormally high resistant pattern. The waveform was characterized by a normal brisk forward flow component in systole with sustained reversed diastolic flow or pandiastolic flow reversal (PDFR). PDFR was documented in the radial and ulnar arteries and as high as the axillary artery (Figure 1 A, B). In contrast, arterial Doppler signals recorded from the unaffected arm revealed a normal triphasic pattern, (Figure 1 C). The attending physician was immediately notified about the presence and extent of the deep and superficial vein thrombosis. He was also informed that the unusual arterial signals recorded in this patient represented arterial compromise to the limb secondary to the venous process.
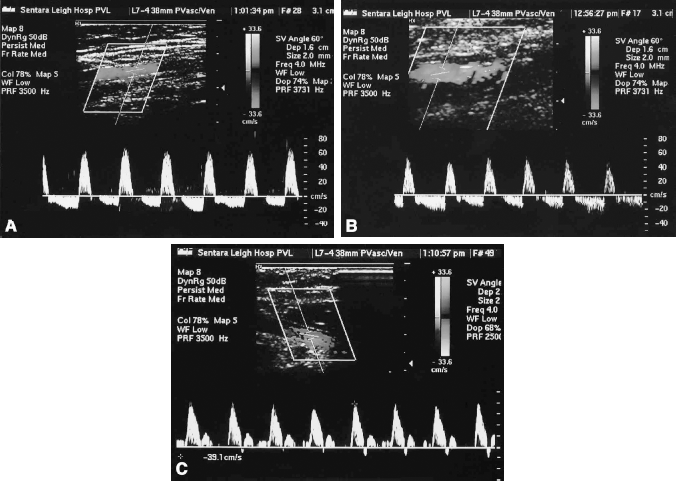
Spectral Doppler waveform from the right radial artery (A) and the right brachial artery (B) demonstrating PDFR during the initial study. Spectral Doppler from the contralateral brachial artery demonstrating a normal triphasic pattern (C).
Treatment for this patient included immediate elevation of the arm, anticoagulation, and emergency fasciotomies of the forearm and hand. Initially, there was improved capillary refill and less rigidity of the arm because of reduced compartment pressures. However, over the course of the next several days, cyanosis recurred, and the patient experienced a decrease in her hand range of motion. Arteriography revealed a patent right axillary, brachial, radial, and ulnar artery (Figure 2 A). There was no arterial flow, however, below the level of the wrist (Figure 2 B). Despite an aggressive treatment regimen, the patient continued to experience uncontrollable pain and gangrene of the hand and wrist developed. One week after the discovery of the DVT, an amputation of the hand and wrist was performed. Repeat CDU showed almost complete recanalization of the venous thrombosis and the PDFR arterial Doppler signals were replaced by a hyperemic triphasic pattern (Figure 3).
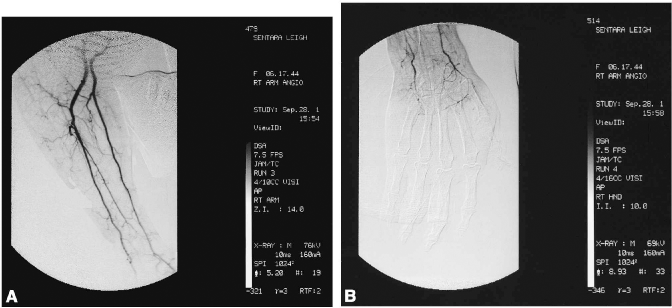
Angiogram shows a patent subclavian, axillary, and brachial artery (A). The radial and ulnar arteries both fill but abruptly end at the wrist with no flow to the hand (B).
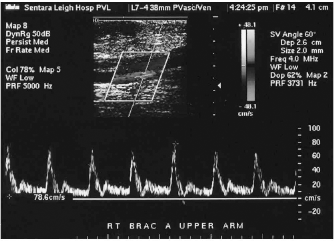
Follow-up CDU after amputation of the right hand showed recanalization of the DVT and loss of the PDFR. The forward diastolic flow represented a hyperemic state.
Discussion
CDU has long been recognized as an accurate diagnostic tool in detecting DVT. This case report demonstrates the usefulness of CDU to detect not only DVT but also the early hemodynamic changes associated with arterial compromise in PCD. The unique arterial waveform with PDFR noted in this patient with PCD has also been reported in other high resistant states including renal vein thrombosis, increased intracranial pressure, and compartment syndrome.7–9 In each of these conditions, the extreme elevation in tissue/interstitial pressures exceeds diastolic pressure causing reversal of flow throughout the diastolic interval of an arterial Doppler signal. The PDFR signal represented the loss of normal arteriovenous pressure gradients necessary for proper perfusion of tissues. This process can be exacerbated during hypotension.
In our vascular laboratory, the venous duplex protocol has been modified to include arterial duplex waveforms from a limb that exhibits extensive deep and superficial vein thrombosis. When encountered with extensive venous thrombosis, PDFR represents hemodynamic changes consistent with arterial compromise. The technologist can then alert the physician to the presence of a complicated DVT early in the course of PCD, before Doppler signals and pulses are lost, at which time the process of ischemia may still be reversible.