
Abstract
Most medical conditions that occur in the popliteal fossa are symptomatic due to the compact anatomy of the area. Usually common problems behind the knee involve either the soft tissue, and/or vasculature and therefore are limited to several commonly known pathology and sequela. Complications behind the knee are mostly consistent in presentation due to a set of conditions, and are age/gender specific.
Ultrasound is a noninvasive (and for the most part) painless and inexpensive exam with a high sensitivity for identifying atypical structures behind the knee. This article draws attention to a rare mass in the popliteal space, which required an alternate approach to a set protocol in order to meet the specific symptoms of the patient. As a result, we were able to identify the vascular effect caused by this mass. In this particular situation, with the aid of another diagnostic modality, proper assessment of the structure was made possible. The findings were consistent with a ganglion, which is a relatively uncommon occurrence behind the knee.
Introduction
Ganglion is defined as a knotlike mass of nerve cells collected in groups outside the central nervous system. 1 Although ganglion cysts of the popliteal fossa are an uncommon finding, the reason for their origin in the cruciate ligaments is still unknown. Many theories have been proposed, including synovial herniation into ligament fibers, ectopic inclusion of synovial tissue, a posttraumatic connective degeneration, and, finally, the proliferation of totipotent mesenchymal cells. 2 The diagnosis of a ganglion cyst is possible by combining clinical examination with magnetic resonance imaging (MRI). Ganglion cysts have a well-defined, circumscribed outline and are localized along the ligament, usually in the dorsal aspect and/or in the popliteal tendon.
Ultrasound imaging is generally reliable and accurate in defining cystic structures behind the knee (e.g., Baker's cyst named for William Morrant Baker, who described eight cases of a synovial fluid sac outside of the joint in 1877). It is believed that the formation of Baker's cyst is a protective mechanism, by providing a path for excess knee joint fluid to drain instead of accumulating in the joint space and causing pressure injury. When using ultrasound imaging to differentiate between cystic and mass structures, cystic structures contain accumulations of fluid and are usually round/oval with a smooth surface, whereas mass structures contain cells that cluster together more densely than the surrounding tissue, creating an echodense interior that can be either homogeneous or heterogeneous.
The case presented in this report will draw special attention to the clinical/vascular consequences caused by a mass in the popliteal space.
Case Presentation
This case presentation involves a 44-year-old man with no previous health problems. His main complaint was cramping in the left calf and coldness in his foot, caused by bending his leg. The patient noticed these symptoms while spending time outside weeding and gardening. At the request of his physician, he arrived at a nearby hospital for an arterial ultrasound evaluation. The arterial testing, which included segmental pressure and pulse volume recording, demonstrated an ankle brachial index of 1.4 on the right and a 1.3 on the left. On the basis of these indices, the findings suggested normal peripheral arterial flow.
The patient sought a second vascular opinion, because his symptoms were not improving. His vascular specialist referred him to our facility for arterial duplex ultrasonography with special attention to the left popliteal fossa.
After eliciting a history, the examination began by having the patient lie on the examining table in the prone position with a rolled-up towel in the dorsum of the foot (causing a slight bend in the knee 10–20°), which eases the scanning of the popliteal space. The ultrasound equipment used was an ATL Ultrasound, HDI 3000 (Bothell, WA) with a 7.5-MHz linear array transducer.
The ultrasound study of the left leg demonstrated an oblong mass with well-circumscribed margins, adequate through transmission, and intracapsular echogenic speckles. The mass was located in the posteromedial apsect abutting the popliteal artery. The mass measures approximately 2 cm x 1 cm in the longitudinal axis and 1 cm x 1 cm in the transverse plane (see Figures 1 and 2). The contralateral popliteal space was essentially unremarkable.
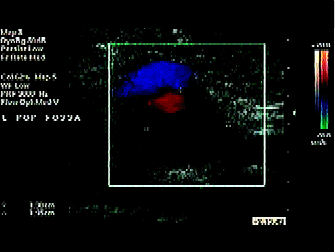
Sonographic image of left popliteal artery (long axis). The calipers measure the ganglion posterior to artery.
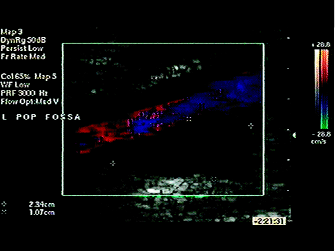
Sonographic image of left popliteal artery (transverse axis). The calipers measure the ganglion posterior to artery.
With the patient in the supine position and his leg abducted with a slight knee bend, a duplex image with Doppler tracing was recorded from the posterior tibial artery (at ankle level) and proved to be within normal limits.
Because his symptoms occurred when he was bending, the patient was directed to kneel upright (with back straight) on top of the examining table, a duplex scan of the posterior tibial artery at ankle level demonstrated no changes in the Doppler signal. As the patient sat slowly back on his legs, the Doppler signal and color flow disappeared, suggesting that maintaining this position would explain the calf pain (claudication) that he was experiencing.
As the patient returned to the original kneeling position, the Doppler signal reappeared. On the basis of the appearance of the returning waveform, this position caused a reactive hyperemic event. A venous examination revealed decreased venous return when knee flexion occurred.
A magnetic resonance imaging scan of the left knee revealed a lobulated mass in the posteromedial soft tissue abutting the anterior aspect of the artery. The mass demonstrates a low signal on the T1-weighted images and hyperintense on the T2-weighted images. This appearance is typical of a ganglion (see Figures 3 and 4).

MRI image of artery (sagital view). Ganglion visualized anterior to artery.

MRI image of popliteal fossa (transverse view). Ganglion, artery, and vein.
Surgical removal of the ganglion was done a few weeks later, and postoperatively the patient has been symptom free.
Discussion
Ganglion cyst is a relatively uncommon occurrence. A study by Bellelli et al. 2 reported only eight cases in a series of 1,600 knee MR examinations since 1994. Other cystic lesions found in the popliteal fossa include Baker's cyst, synovial pseudocyst, meniscal cyst, and ganglionic cyst. A nonatherosclerotic cause of peripheral occlusive disease is cystic adventitial disease (CAD). Cystic adventitial disease is a colleciton of gelatinous fluid in the tunica adventitia layer of the blood vessel wall. The most common site for this disease is in the popliteal artery as described by Eirup and Hierton in 1947. Usually men in the fourth or fifth decade of life are more likely to be affected and are seen with a sudden onset of intermittent claudication. Although the origins of the CAD are unknown, adventitial cysts are both biochemically and histologically similar to the ganglion. There are also vascular complications (e.g., popliteal aneurysm as described by Kotval et al.) 3 Another vascular complication is popliteal entrapment, which was described by T. P. Anderson Stuart in 1879 as a variant of the popliteal artery. This is an uncommon condition usually affecting young otherwise healthy athletic men who are pain free at rest but have aching and numbness develop in the foot after exercise.
The diagnosis of a popliteal ganglion by use of ultrasonography is highly unusual. However, knowledge of the sonographic characteristics of a Baker's cyst may help rule out this simple cyst and suggest additional examinations. This case report draws attention to the clinical history, unique patient complaint, alteration of traditional ultrasound protocol to allow for specific conditions, differential diagnosis, and integration of different diagnostic modalities to produce an accurate assessment of the problem and recommend the most appropriate treatment.