
Abstract
Congenital anomalies of the aortic arch are rare, with very few cases reported in the literature. Congenital absence of the common carotid artery (CCA), with separate origins of the internal carotid artery (ICA) and external carotid artery (ECA) is a rare anomaly. This case illustrates a congenital anomaly in the development of the right carotid system. By use of duplex sonography, we report of the absence of the right CCA with separate ICA and ECA originating from the innominate artery.
Case Report
The patient is a 56-year-old woman, with no significant medical history. The patient was initially seen with complaints of left eye visual disturbances by an ophthalmologist. She described these changes as “black lines through water” and lasting for 10–15 min. She also complained of light sensitivity. The patient denied any dizziness, syncope, vertigo, or weakness of any extremity. Significant findings on physical examination were the presence of a right carotid bruit. The patient was referred for a carotid artery duplex examination.
A carotid duplex examination was performed with an ATL HDI 3500 (Bothell, WA) with a linear array 7-4 MHz transducer. Duplex examination of the right cervical carotid system demonstrated two parallel arteries with no hemodynamically significant plaque or stenosis (Figure 1). Tracing these vessels inferiorly suggested they originated from the innominate artery. Spectral Doppler ultrasonography of the more anterior artery demonstrated an external carotid artery (ECA)–type waveform. The ECA has a rapid upstroke and downstroke with a very low diastolic component, and a dicrotic notch is clearly seen (Figure 2). The more posterior artery displayed a typical internal carotid artery (ICA) waveform. The waveform of the ICA has a rapid upstroke and slight delay in the downstroke with a high diastolic component (Figure 3). When scanning caudally, both vessels originate at the innominate artery. The examination failed to demonstrate any right common carotid artery (CCA).
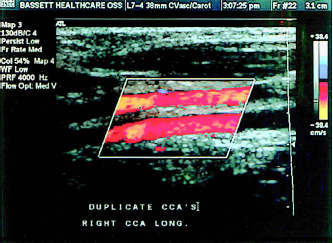
Duplex examination of the cervical carotid system demonstrating two parallel arteries.
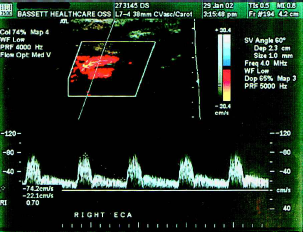
Spectral Doppler ultrasonography demonstrating an ECA waveform.
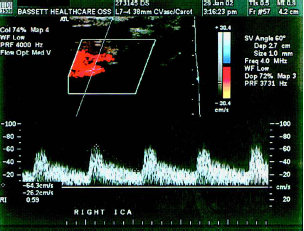
Spectral Doppler ultrasonography demonstrating an ICA waveform.
The right vertebral was imaged and demonstrated antegrade flow. Examination of the left cervical carotid system was unremarkable.
After the carotid duplex examination, a workup included an MRI/MRA of the brain. This examination demonstrated an aneurysm of the right posterior communicating artery. A further workup included an angiogram of the aortic and brachiocephalic trunk, which showed congenital absence of the right CCA, with the ECA and ICA originating from the innominate artery (Figure 4). The patient was eventually transferred to another institution for neurosurgical intervention.

Angiogram of the aortic and brachiocephalic trunk, displaying origin of the ECA and ICA from the innominate artery. (A) Innominate artery; (B) subclavian artery; (C) internal carotid artery; (D) external carotid artery.
Discussion
The ECA and ICA arising separately is a rare condition. This embryologic anomaly is also called absence of the CCA. The earliest reported case of the absence of the CCA is that of Malacarne in 1784. 1 He described the presence of a double aortic arch with a separate origin of the ECA and ICA on both sides in a cadaveric specimen. A book by Lie 2 in 1968 pertains to anomalies of the cervical carotid system.
During normal embryologic development, the ECA and the ICA arise from the third aortic arches. During the sixth to eighth weeks of embryologic development, the primitive aortic arch pattern of arteries is transformed into the basic adult arterial arrangement. 3 The final formation of the carotid artery is reached when the ductus caroticus is obliterated (Figure 5). That is the portion of the dorsal aorta between the third and fourth aortic arches. Because of the persistence of some portions of this system and the disappearance of others, it is understandable that anomalies do occur.
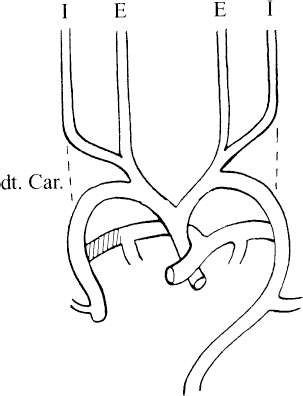
Embryologic development of the cervical carotid system with obliteration of the ductus caroticus (dotted line).
If the anomaly occurs on the right side, both the ICA and the ECA might arise separately from the innominate artery. The other possible formation is that the ICA might originate from the subclavian artery and the ECA from the innominate artery.
In this case report, the failure of the third and fourth aortic arches to divide resulted in a separate ICA and ECA with origins from the innominate artery (Figure 6). If the anomaly occurs on the left side, it is because of persistence of the ductus caroticus causing the ICA and ECA to arise separately from the aortic arch.
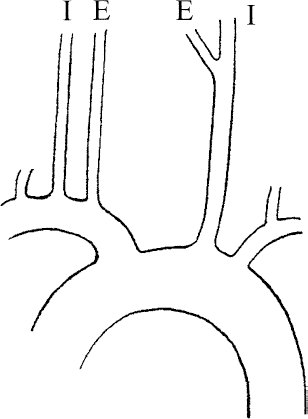
In our case, separate origins of the right ICA and ECA from the innominate artery resulting from persistent ductus caroticus.
The abnormality reported here is a rare congenital anomaly with a limited number of cases previously identified and even fewer angiographic reports in the literature.4–7 Woodruff et al. 8 described a similar case based on duplex and sonographic findings. Most recently, Jerius et al. 9 reported a case of separate origin of the right ECA from the innominate artery and right ICA from the subclavian artery. The patient also had a proximal occlusion of the right subclavian artery and occlusion of the left ICA, which resulted in a vertebrobasilar syndrome.
Salles-Cunha and Andros 10 published two other examples that expand the practical aspects that face a sonographer in the vascular laboratory. The first case is that of a congenitally absent internal carotid artery. In this case, duplex sonography demonstrated a single carotid artery in the neck. The waveform was characteristic of the ECA. Arteriography showed the origin of the ECA at the aortic arch and an absent ICA. The second case is that of an anomalous vertebral artery. Duplex sonography demonstrated two parallel vessels in the neck that originated from the subclavian artery. The larger vessel demonstrated flow characteristics of a CCA. The second, and smaller, vessel demonstrated flow velocities that mirrored those in the vertebral artery obtained between the vertebral transverse processes. The suggestion that this was an anomalous vertebral artery was further confirmed by tracing it into a vertebral artery foramen of a transverse process.
The absence of the CCA in our patient was identified by duplex scanning on the basis of two-dimensional imaging and the characteristic spectral waveforms observed from the ICA and ECA. Although many anomalies of the cervical carotid system might be readily identified during duplex scanning, technical limitations might prevent the identification of all. For example, the presence of a very low bifurcation might lead the sonographer into a false conclusion of an absent CCA. It is important to recognize anatomic variations of the cervical carotid system, because they might have an impact on patient treatment and surgical intervention. With the availability of modern, high-quality ultrasound systems, the ability of sonographers to detect anatomic anomalies is the best it has ever been. This often entails the use of two-dimensional imaging in conjunction with pulse-wave and color Doppler ultrasonography.