
Abstract
Introduction
Pseudoaneurysm formation is a rare complication following carotid artery revascularization with a low estimated occurrence of 0.15 to 0.6%. This may result from percutaneous intervention, trauma, or infection. Patients may present with pain and swelling as well as a pulsatile cervical mass.
Case Report
A 56-year-old male with a history of multiple carotid endarterectomies and an interposition synthetic graft presented with a recurrent high-grade stenosis. The patient underwent a balloon angioplasty and stent placement in the internal carotid artery. Two months postintervention, the patient presented with swelling and tenderness at the incision site. Color duplex ultrasound (CDU) was performed, demonstrating a 1.7 × 1.8 cm perigraft collection without evidence of flow. The patient returned in 2 weeks with increased swelling and discomfort. This prompted a repeat CDU, demonstrating a 3.7 × 3.9 cm hypoechoic, perigraft collection, now doubled in size from the previous exam. An abscess was confirmed by needle aspiration and positive culture results. He was admitted and underwent 6 weeks of antibiotic therapy. Upon discharge, the patient returned for a follow-up CDU. A perigraft collection with arterial flow was now present that had not previously been noted. Angiography confirmed extraluminal flow at the level of the carotid stent. The patient underwent operative debridement with excision of the infected graft and repair of the pseudoaneurysm.
Conclusions
Carotid artery interventions have a very low incidence of infection. The occurrence of an infected or mycotic pseudoaneurysm following carotid intervention is extremely rare. CDU is a vital tool in detecting thrombosed versus active pseudoaneurysms, which may help guide appropriate therapeutic decisions.
Introduction
Carotid pseudoaneurysms generally occur as a result of an infection, trauma, surgical procedure, or suture failure.1,2 In 1888, Rudolph Matas reported the first successful pseudoaneurysm repair. 2 Pseudoaneurysm formation is rare, occurring in only 0.15%–0.60% of all carotid endarterectomies performed.2,3 Carotid pseudoaneurysms are twice as likely to occur with patch angioplasty, particularly when Dacron is used. 4 Prior to 1960 when silk sutures were used, the complication of pseudoaneurysm following revascularization was as high as 80%.2,3,5 The type of suture material and its durability are the determining factors in maintaining a strong union between the prosthetic graft and the site of anastomosis. 2 The rare occurrence of infection is attributed to the sterile nature of the surgical field. 5 When a foreign material such as a synthetic patch, Dacron, or polytetrafluoroethylene (PTFE) is used for repair; the incidence of infection is always greater. The term “mycotic pseudoaneurysm” refers to a false aneurysm that has formed secondary to an infection.6,7 Symptoms of pseudoaneurysm formation include pain and swelling, pulsatile cervical mass, and transient ischemic attack secondary to embolization. 3
Color duplex ultrasound (CDU) is a valuable tool in detecting the presence of flow in a pseudoaneurysm. This case study involves a mycotic carotid pseudoaneurysm detected by CDU 2 months postintervention and confirmed by pathology and angiography.
Case Report
This case involves a 56-year-old male presenting with a recurrent high-grade carotid stenosis despite multiple endarterectomies and ultimately a right internal carotid artery (ICA) Dacron interposition graft. Intervention involved a balloon angioplasty and stenting of the recurrent stenosis within the interposition graft. Two months postoperatively, the patient presented to the office with swelling and tenderness at the incision site. CDU was performed, demonstrating a patent carotid artery stent and interposition graft with normal hemodynamics. A 1.7 × 1.8 cm perigraft collection was identified without evidence of arterial flow. Within 2 weeks, the patient returned with increased swelling and discomfort at that location. A repeat CDU revealed the perigraft collection had enlarged in size to 3.7 × 3.9 cm. The collection was thoroughly interrogated using color and spectral Doppler without any discernible flow identified. A needle aspiration was performed, and surgical findings identified 1 ml of purulent material consistent with a non-maturing abscess. The patient was admitted to the hospital and treated with antibiotic therapy. Upon discharge, the patient returned for a follow-up CDU, which identified a slightly smaller, but persistent perigraft collection (Figures 1A and 1B). Spectral Doppler now confirmed a high resistant signal within the collection. This was highly suggestive of a carotid artery pseudoaneurysm at the level of the stent (Figure 2).
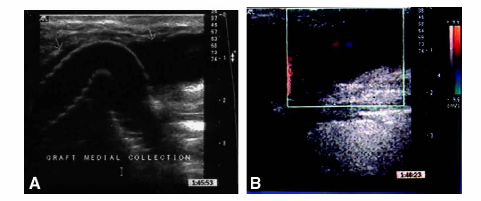
(a) Carotid interposition graft in gray scale. (b) Carotid interposition graft with color flow in perigraft collection.
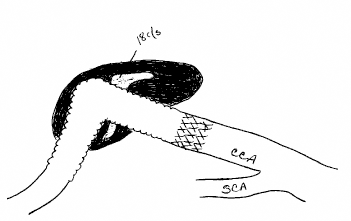
Sketch of pseudoaneurysm.
An angiogram was performed and confirmed extraluminal flow at the level of the carotid stent anastomosis (Figure 3). The patient underwent debriedment and excision of the infected graft and repair of the pseudoaneurysm. Carotid reconstruction of the common carotid artery to distal ICA greater saphenous vein bypass was completed.
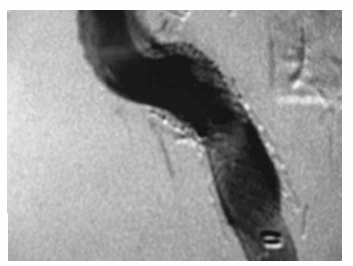
Angiographic demonstration of extraluminal flow.
The patient returned for a 3-month CDU and demonstrating no evidence of collection or abscess. The patient presented 3 months later with visual changes, left-side weakness, and syncope. Unfortunately, CDU at that time revealed a completely occluded right internal carotid artery reconstruction. As of April 2003, the patient's symptoms have resolved, and he is being followed conservatively.
Conclusions
CDU plays an important role in the postoperative surveillance of carotid intervention. Though the incidence of infection or pseudoaneurysm formation following carotid intervention is extremely rare, it is potentially a dangerous complication. If left untreated, the patient is at high risk for embolization. Resection and reconstruction with an autogenous vein interposition graft is usually the preferred method of treatment. 6 CDU is an accurate way to detect the presence of flow within a pseudoaneurysm and to note perigraft collections, which may represent infection.