
Abstract
Introduction
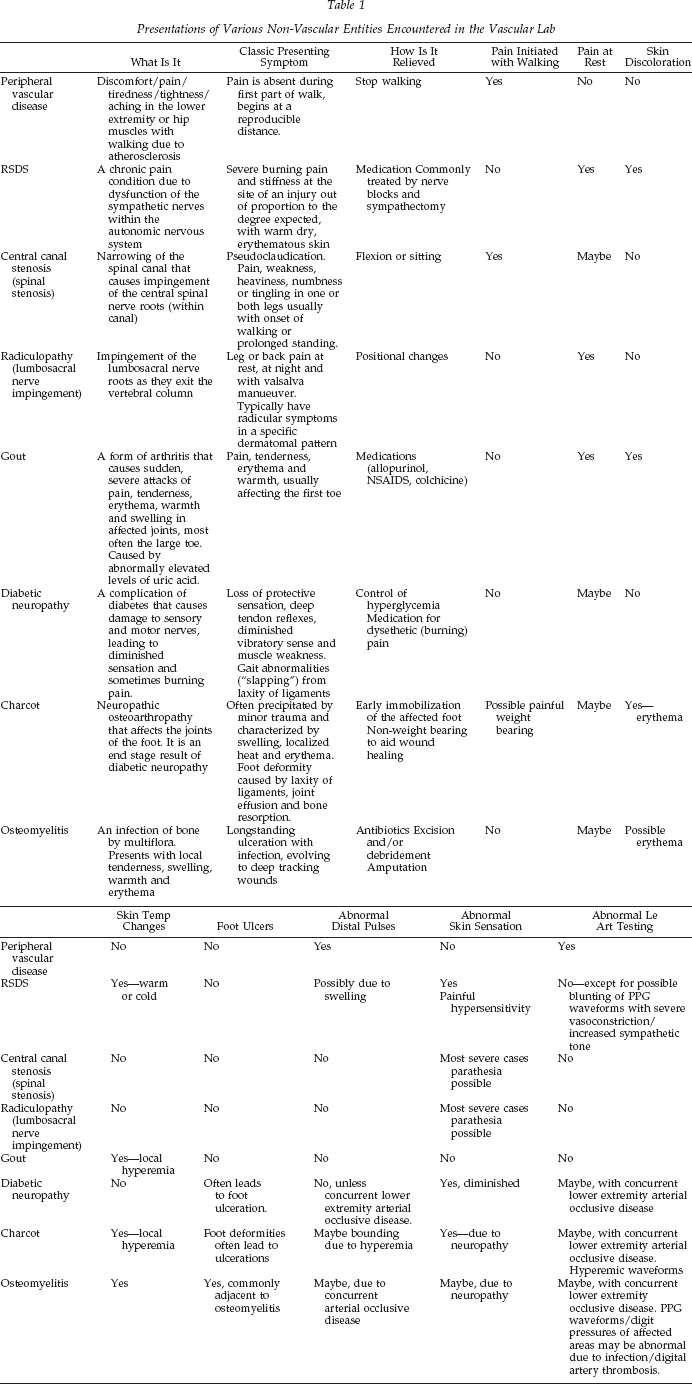
Noninvasive lower extremity arterial evaluations comprised 34% (1381/4104) of our vascular laboratory's patient volume in the year 2002. Often, patients presented with one or more symptoms suggestive of arterial disease; however, their vascular study results indicated a degree of arterial disease that was incongruent with their symptoms. It is necessary for the vascular technologist to understand the differential diagnoses that mimic the symptoms of arterial insufficiency. This clinical review describes other nonatherosclerotic disorders affecting the lower extremities. These include reflex sympathetic dystrophy syndrome (RSDS), lumbar spinal stenosis (LSS), gout, diabetic peripheral neuropathy, Charcot foot, and osteomyelitis (Table 1). Our goal is to briefly describe these clinical possibilities to enhance understanding.
Presentations of Various Non-Vascular Entities Encountered in the Vascular Lab
Reflex Sympathetic Dystrophy Syndrome
Reflex sympathetic dystrophy syndrome (RSDS), or complex regional pain syndrome (CRPS), is a chronic pain condition that was first documented during the American Civil War. 1 RSDS and CRPS are two of the more common terms used to describe an often confusing disorder that consists of a myriad of seemingly unrelated symptoms. Misunderstanding of this problem is compounded not only by its multiple names, but also by poor understanding of its physiology and unclear diagnostic and treatment criteria.
RSDS is believed to be a dysfunction of the sympathetic nerves within the autonomic nervous system. Activation of the sympathetic nervous system after an injury is a normal adaptive response. The sympathetic nerves cause the blood vessels in the skin to contract, shunting blood flow to central organs and reducing blood loss from wounds. Normally, the sympathetic nervous system shuts down soon after an injury, but in individuals with RSDS it stays hyperactive. This “overactive” sympathetic nerve feedback causes dysfunction of somatic sensory nerves leading to “hypersensitivity” of affected regions and sustained sympathetic activity in segments of the spinal cord. It is theorized that this begins a vicious cycle of neural overactivity that can subsequently affect other areas of the body. The sympathetic nerve chain exists along the entire spinal cord and crosses the midline of the body, outside the spinal cord. This explains how symptoms can spread from one limb to another, on the same or contralateral side, and affect different areas of the trunk. 2
Many factors can precipitate RSDS including trauma (major and minor), myocardial infarction, surgery, spinal cord disorders, and strokes. Symptoms of RSDS can begin weeks to months after the precipitating event has occurred, often after the expected time for healing.
This syndrome has been called a “chameleon disease” because its varied symptoms change so rapidly and profoundly, often not following the textbook description. It presents a clinical puzzle that can be challenging to piece together. Unfortunately, it often goes unrecognized initially, when it can be most successfully treated. RSDS can mimic nerve entrapment syndromes, so this should be one of the first differential diagnoses to rule out. 3
The classic presenting symptoms of RSDS are severe burning pain and stiffness at the site of an injury with warm, dry, erythematous skin. The pain is out of proportion to the degree expected. The skin can rapidly change to become cyanotic, cool, and sweaty due to cutaneous arteriolar vasospasm. Localized edema, muscle spasm, increasing joint stiffness (from disuse), and patchy osteoporosis are other early symptoms. Rapid hair and nail growth and hypersensitivity to touch or cold may be present. Many of these symptoms are transient. These early symptoms are classified as stage I (Figure 1), or the acute phase of the syndrome, and can last from 6 weeks to 6 months, averaging 3 months. 4

Early presentation of RSDS in a female. Right foot with warm, dry, erythematous skin, and localized edema.
In stage II, also called the dystrophic stage (lasting 3–6 months), there is a marked increase in the pain, swelling, sensitivity to touch, and disuse of the affected area. Symptoms have often spread beyond the initial site. Other characteristics include skin coolness and cyanosis, decreased hair growth, brittle nails, and muscle atrophy. Spotty osteoporosis progresses to become severe and diffuse.
As the disease advances to stage III (atrophic stage), symptoms intensify. The pain may become intractable and symptoms irreversible. Muscle atrophy and joint contractions occur, and bone deossification is marked and diffuse. The pain may have spread to another limb, even on the contralateral side. 4
Early diagnosis and treatment is paramount with this disorder, as it is highly resistant to treatment in its later stages. The patient's history and physical exam are important components, along with eliminating other possible etiologies. Testing may include thermography, radiographs, bone scans, nerve blocks, 3D-CT scans, and electromyogram (EMG) nerve conduction studies.
If RSDS is correctly diagnosed and treated early, symptoms may resolve. In stages I and II, a series of chemical sympathetic blocks can help predict those patients who might benefit from surgical sympathectomy and can occasionally be curative. Physical therapy should be initiated as soon as possible to prevent contractures, avoid progression of osteoporosis, and help the patient to regain function. Those patients who have progressed to stage III are less likely to respond to sympathectomy. The longer treatment is delayed, the greater the chance the patient will suffer severe chronic pain and permanent disability. Avoiding immobilization as much as possible after an injury or surgery may help prevent RSDS.
Patients with RSDS will occasionally be referred to the vascular lab to rule out deep venous obstruction due to their symptoms of limb swelling, pain, and skin discoloration. Sometimes they are sent to rule out arterial insufficiency due to pain, skin coolness, cyanosis, and hair loss. Pulses may be nonpalpable due to edema. Noninvasive arterial and venous evaluations in this population will be within normal limits unless concurrent problems exist. RSDS does not affect deep veins or arteries enough to cause abnormal findings in the vascular lab. In early stage I, hyperemia may be evident, and cutaneous vasoconstriction in late stage I and beyond could conceivably cause some blunting of a digit arterial photoplethysmographic (PPG) waveform.
Lumbar Canal Stenosis
Lumbar canal stenosis is a narrowing of the spinal canal that can cause impingement of the spinal nerve roots in the central canal and/or lateral recess. Several factors in combination or alone can cause spinal stenosis, such as facet joint hypertrophy, ligamentum flavum thickening, and disc bulging and protrusion (Figure 2). The most common factor preceding spinal stenosis is degenerative spondylolisthesis. This is characterized by forward displacement of a vertebra due to disc and facet degeneration, causing reduction in the diameter of the spinal canal. Spinal stenosis can be classified by one of two methods, either by presumed etiology (congential or acquired) or by location (central or lateral recess stenosis). The majority of cases of spinal stenosis are acquired due to aging. 5 The prevalence of lumbar stenosis has been reported as ranging from 1.7% to 8% annually in the general population. 6
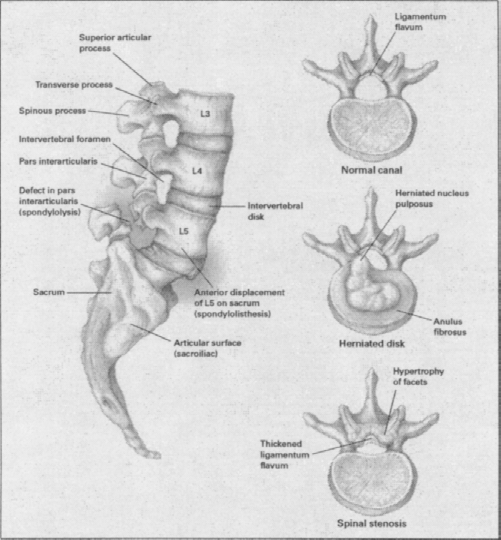
Anatomical presentations of lumbar canal stenosis.
Because central spinal stenosis is usually caused by degenerative changes, it typically affects persons over 50 years of age. The classic symptom of central canal stenosis is pseudoclaudication or neurogenic claudication. Patients usually complain of pain, weakness, heaviness, numbness, or tingling in both legs usually with walking (variable distances) or prolonged standing. The symptoms start immediately after beginning walking and are associated with back pain, although the leg symptoms are more pronounced than the back pain. The symptoms are relieved with sitting or flexed forward position. 5 Typically they can walk further with less pain in the forward flexed position, such as using a grocery cart.5,7 They can typically stand longer with less pain in a forward flex position with knees slightly bent (“simian stance”). Flexion or sitting will open up the spinal canal, thus relieving the symptoms. The association of the posture change to relief of symptoms is a key sign of pseudoclaudication. 5
Lumbosacral nerve impingement is most commonly acquired (due to aging) and occurs in younger patients (mean age 40). 5 The lateral recess is too narrow and causes pressure on the nerves as they exit the spine. The most frequent cause is a nerve root at the neural foramen. It can occur alone or in combination with central canal stenosis. 7 Though the symptoms of central canal stenosis and lumbosacral nerve impingement are similar, typically pseudoclaudication does not occur with lumbosacral nerve impingement. 5 The patient's peripheral symptoms are classically those of sciatica; pain in the lower back and hip, radiating down the back of the thigh into the leg. 7 Radicular symptoms can include weakness, pain, or loss of feeling in the area of the body to which the affected nerve goes. They often have pain at rest, at night, with valsalva maneuver.5,7
Clinical history and physical exam are the basis for diagnosis of spinal stenosis with imaging exams done for confirmation. MRI is the first modality of choice. It is noninvasive and has excellent resolution of neural and soft tissue. Myelogram followed by a CT (myelo-CT) is preferred when MRI is not available. Myelo-CT is done due to the fact that myelogram alone is not as sensitive as MRI and CT in diagnosing lumbar spinal stenosis. 5
The initial management of lumbar spinal stenosis may be nonsurgical. These include activity restrictions, physical therapy, analgesics, anti-inflammatory medications, lumbosacral orthoses, epidural injection, and calcitonin. Surgical treatment consists of decompressive laminectomy with or without fusion and laminotomy.5,7
It is important to know the difference between vascular claudication/atherosclerosis symptoms and symptoms caused by lumbar spinal stenosis. Though lumbar stenosis symptoms are similar to atherosclerosis, if the vascular technologist takes a careful history, the difference will come clear. Vascular technologists should be sure to document whether the symptoms start immediately with walking, prolonged standing, with positional changes; are the symptoms relieved by stopping, sitting, or flexing/bending.
Gout
Gout is a form of arthritis that causes sudden severe attacks of pain, tenderness, redness, warmth, and swelling in some joints with the large toe most frequently affected. 8
Hippocrates first described gout in the fifth-century B.C. Approximately 1 million people in the United States suffer from attacks of gout. 8 Gout is more common in men than in women. It usually attacks males between the ages of 30 and 50. In women, gout attacks usually occur after menopause. Certain medical conditions and treatments can increase the risk of gout. Untreated high blood pressure, diabetes, hypertension, hyperlipidemia, and arteriosclerosis are risk factors. Obesity, surgery, severe illness and immobility can lead to increases in uric acid. Plasma urate concentration is the single most important determinate of the risk of developing gout. 9
Gout is characterized by abnormally elevated levels of uric acid in the blood. It is often related to an inherited abnormality in the body's ability to process uric acid. Uric acid is a breakdown product of purines, which are part of many foods we eat (organ meats, fish, and poultry). Normally, the uric acid dissolves in the blood and passes through the kidneys into the urine. Uric acid not excreted can build up, forming sharp needle-like crystals in a joint or surrounding tissue (Figure 3). 8
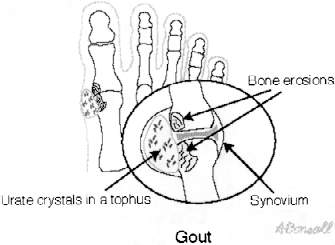
The joint inflammation is precipitated by deposits of uric acid crystals in the joint fluid (synovial fluid). 1996–2003, MedicineNet, Inc. All rights reserved.
Gouty arthritis is usually an extremely painful attack with rapid onset of joint inflammation (Figure 4). 10 The joint inflammation is precipitated by deposits of uric acid crystals in the joint fluid (synovial fluid) and joint lining (synovial lining). Intense joint inflammation occurs as white blood cells engulf the uric acid crystals and release chemicals of inflammation, causing pain, heat and redness of the joint tissues and chills, shivers, and fever. 8

Gout most often affects the great toe charcterized by severe pain, swelling, and erythema of the joint. Merck Research Laboratories. 1992:1343–1349.
The diagnosis is usually made from the history and physical examination.
Hyperuricemia is due to overproduction or under-excretion of urate. A 24-hr measurement of urate and creatinine clearances while on a normal diet and again after 5 days on a low purine diet can aid in detecting hyperuricemia. Fluid withdraw (joint aspiration) can be used in larger joints to detect crystals of uric acid within the WBC in the affected joint. During the early acute attacks, the only radiographic abnormalities are those consequent upon the soft tissue swelling that results from the intense articular inflammation and related soft tissue edema. Occasionally, tophi will exhibit calcification. Late in the disease, radiographs demonstrate extensive erosive damage, which may result in loss of joint space. 9
Treatment consists of termination of the acute attack with nonsteroidal anti-inflammatory drugs to help relieve symptoms or prescribed steroidal anti-inflammatory drugs such as prednisone. Prevention of future attacks is by daily prophylactic use of colchicine to reduce the crystal-induced inflammation or other medications (allopurinol) that slow the production and speed the elimination of uric acid.
The association between gout and vascular disease is most likely dependent on several factors other than hyperuricemia, particularly hypertension, obesity, and platelet adhesiveness. 9
Charcot Foot
Charcot foot is the term used to describe the end-stage neuropathic osteoarthropathy that affects the joints of the foot (Figure 5). 11 This is a rapidly progressive, degenerative arthritis that results from damaged sensory and motor nerves causing diminished sensation, muscular weakness, and vasodilatation. Decreased sensation allows foot trauma to go undetected and untreated, leading to ligament slackness, bone and cartilage damage, and, ultimately, foot deformity. The bones most often affected are the metatarsals and the tarsals. If this process is not detected and treated early, foot deformities can lead to nonhealing ulcerations and sometimes amputation. 12

Early presentation of Charcot foot.
Jean-Martin Charcot (1825–1893), a French physician credited for creating the foundations of neurology, gave his name to this disorder but was not the first to describe it. In 1703, Musgrave described the condition as a complication of tertiary syphilis. Charcot foot is no longer commonly seen associated with syphilis since the development of penicillin. 13
Today, Charcot foot is usually seen in diabetic patients with long-standing neuropathy. Approximately half of all people with diabetes for 20 years will have evidence of peripheral neuropathy. 14
The exact etiology of the Charcot process is incompletely understood, but underlying neuropathy is always present. It is common belief that neurovascular and neurotraumatic factors are involved. 13
The neurovascular theory postulates that hyperemia, caused by loss of sympathetic tone and constrictive control of blood vessels (vasodilatation), leads to resorption of bone, causing it to become osteopenic. This leads to the bones becoming weak and easily susceptible to fractures. 13
The neurotraumatic theory exposes that due to sensory neuropathy, the patient is unaware of the stress placed on their feet with normal activity, which results in trauma that starts the inflammatory process. The precipitating event could be as seemingly innocuous as striking the floor too hard with ambulation. Approximately 50% of patients with Charcot will recall a foot trauma. 15
Charcot is an end-stage presentation of diabetic neuropathy. The etiology of neuropathy is not completely understood, but chronic hyperglycemia is believed to be the major factor. Understanding diabetic pathophysiologic foot alterations is helpful in understanding the Charcot foot.
As diabetic neuropathy symptoms progress, the patient experiences worsening peripheral paresthesias and loss of motor nerve function that leads to weakness in the intrinsic muscles of the foot. This process, along with decreased proprioception, leads to foot architecture deformities. Common foot architectural changes are “clawing of the toes,” collapse of the arch, and prominent metatarsal heads, with proximal migration of the metatarsal fat pads. 14
These foot deformities disrupt normal weight distribution with walking. Often, the protruding metatarsal heads, especially the first metatarsal, become the primary weight-bearing surface. This problem leads to ligamentous disruption, joint dislocations, bony fractures, and ulcer formation. 16
Neuropathic ulcers are difficult to heal and can rapidly develop infection because the patient does not experience normal pain due to decreased sensation. Complications include cellulitis, gangrene, osteomyelitis, and, worst of all, multiple organism foot sepsis. It is not uncommon for treatment to require amputation of part of the foot or leg. 16
Diagnosis of Charcot is generally made by the classical clinical presentation of a swollen and warm foot, possibly with erythema. Pain may be present but is usually less than would be expected from the degree of swelling due to the presence of neuropathy. In its earliest stage, Charcot may present with only localized low-grade swelling and heat. Pedal pulses can sometimes be bounding due to hyperemia.13,17
Although the etiology of Charcot foot is argued, most authors agree that there are three stages to its presentation. 12 Stage I is the acute inflammatory response to a fracture. At this stage, the destructive process can be halted with immobilization.
Stage II is marked by persistent hyperemia and inflammation that leads to progressive bone weakening. During this stage, there is absorption of small fragments of bone and fusing of larger pieces to joint surfaces causing ankylosis. Stage III is the chronic, or “cool,” phase of the process. Remodeling of the foot by healing and new bone formation marks this period. 12
Testing for this disease includes radiographs, MRI, CT, bone scans, blood work, and, occasionally, bone biopsy. A handheld infrared temperature scanner used to compare the temperature of the affected foot to the contralateral side may enhance early diagnosis. This temperature testing may also be useful in monitoring disease progression. 17
The most successful treatment consists of early immobilization of the foot with serial casting for 3 to 6 months and non–weight bearing. 18 Surgical reconstruction is sometimes needed.
Prevention of the devastating consequences of Charcot can be facilitated by educating people with diabetes to wear stabilizing, protective footwear and immediately report any foot trauma, especially if it is associated with increased foot swelling and heat.
Practioners less familiar with Charcot may refer patients to the vascular lab. This disease commonly presents with symptoms suggestive of infection or cellulitis. Peripheral vascular disease in patients with long-standing diabetes may give abnormal noninvasive vascular testing results.
Treatment of the diabetic foot is best accomplished by early recognition of neuropathy and use of protective footwear. These shoes are designed to prevent ulcer formation by “off-loading” and protection of “pressure points” with extra padding. When ulcers do occur, early treatment can greatly minimize complications. Reinforcing to patients the importance of daily foot inspection and the need to immediately report any compromise in skin integrity, especially when erythema is present, can enhance this.
Osteomyelitis
Osteomyelitis is an infection of the bone that occurs most frequently in the lower extremities by direct or, less commonly, indirect invasion (by a bloodborne organism). Persons with diabetes are generally more prone to infections than nondiabetic people. An ulceration is usually a painless sore at the bottom of the foot or top of the toes, resulting from excessive pressure at that site. Ulcers frequently underlie a pre-existing corn or callous that is allowed to build too thickly. Trauma from heat, cold, shoe pressure, or penetration from a sharp object are also potential causes. Neuropathy allows the lesion to develop because normal warning sense of pain has been lost and the ulcer goes unrecognized. Continued pressure/walking on the injured skin creates even further damage and worsens the ulcer. The open sore will frequently become infected and may even penetrate to bone. Due to deficiencies in the ability of white blood cells to defend against invading bacteria, diabetics have more difficulty in dealing with and mounting an immune response to the infection. Infections often worsen or may go undetected, especially in the presence of diabetic neuropathy. Infection of bone is accompanied by occlusion of blood vessels, which causes bone necrosis and local spread of infection.
Neuropathy can consist of three phases:
Sensory neuropathy: a loss of sensation; the patient is incapable of sensing pain or pressure. 19
Motor neuropathy: the loss of intrinsic muscles, resulting in a misshapened foot or toes. 19
Autonomic neuropathy: the loss of autonomic system functions, which results in the absence of sweat and oil production leaving the skin dry and nonelastic. 19
The onset of neuropathy may be gradual in the diabetic, with the exact cause not known. Symptoms may include numbness, tingling, burning, and a pins-and-needles sensation. A sudden onset of neuropathy is more frequently painful, and when the pain abates, there is a sensory loss.
Clinical signs are generally a fever, acute illness, local tenderness, swelling, and warmth. There may or may not be drainage. Lab work may reveal positive blood culture, and white blood cells may or may not be elevated. The erythrocyte sedimentation rate and C-reative protein may be elevated. Radiographic signs generally show in 12–21 days after signs and symptoms appear. The infection may be detected earlier by MRI or bone scans.
Evaluation generally consists of a neurological, skeletal, and vascular examination.
Treatment consists of antibiotic therapy, usually excisional debridement or limited forefoot amputations and occasionally vascularized soft tissue coverage (preferably with muscle flap). Stability of the bone must also be restored if infection has led to bone loss and or non-union.
Conclusions
Clinical symptoms associated with numerous disease processes can mimic arterial insufficiency. The vascular technologist's expertise in understanding differential diagnosis can be an important contribution to aide the clinical team in solving the diagnostic riddle.
Footnotes
Acknowledgments
We express our appreciation to J. Bernard, DPM, Chief of Podiatry, and D. Swihart, PhD, DMin, MSN, CS, APRN, BC for their clinical contributions with Charcot and RSDS, respectively, and J. Brann for clerical support.