
Abstract

Introduction
Venous duplex ultrasonography has rapidly become the diagnostic test of choice for acute deep venous thrombosis (DVT). Compared with venography, duplex has a mean sensitivity and specificity of 97% and 94%, with mean positive and negative predictive values of 97% and 98% for proximal DVT. 1 The accuracy, widespread availability, and noninvasive nature of venous duplex ultrasonography has led to progressively increased use over the past decade. Although the incidence of DVT in many validation studies was as high as 25%, the incidence in clinical practice has declined to <10% in many laboratories. 2 Criado and Burnham 3 have estimated that approximately seven venous duplex scans are performed for each DVT diagnosed. Unfortunately, it is not widely appreciated that both the sensitivity and positive predictive value of venous ultrasound depend on the pretest probability of disease. Although the sensitivity is >90% in patients with a high pretest probability of disease, it may be as low as 67% among those with a low pretest probability.4,5 In addition to the potential for diagnostic inaccuracy, the increased use has strained vascular laboratory resources, particularly after hours.
Education of referring practitioners is perhaps the most important measure in reducing the number of inappropriate ultrasound examinations. The value of clinical screening before duplex scanning is more clearly defined for symptomatic outpatients than for inpatients. The prevalence of positive outpatient studies increases from 2.1% among patients without swelling or thrombotic risk factors to 13% in those with thrombotic risk factors but no swelling and approximately 50% in patients with acute unilateral swelling. 5 Among outpatients, the negative predictive value of the absence of unilateral swelling or an existing thrombotic risk factor is >97%.3,5 Chronic unilateral swelling and bilateral swelling are associated with a significant prevalence of chronic findings, although an acute DVT may be found in <1%. 5 Other common indications for vascular laboratory referral, such as joint pain or cellulitis in the absence of thrombotic risk factors, are associated with an exceedingly low prevalence of acute DVT. 5 An accurate clinical history can eliminate the need for many negative studies.
Several strategies for objectively defining the pretest probability of DVT have been validated. Among these, the outpatient scoring system developed by Wells et al. 6 (see Table 1) is the most widely used strategy.
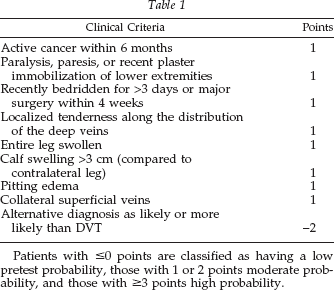
Patients with ≤0 points are classified as having a low pretest probability, those with 1 or 2 points moderate probability, and those with ≥3 points high probability.
Unfortunately, many patients with appropriate symptoms are seen after hours and require appropriate evaluation and management. There are potentially four means of managing such patients: (1) routine duplex ultrasonography, (2) routine treatment with a single dose of low molecular weight heparin followed by duplex ultrasonography during regular business hours, (3) D-dimer screening, and (4) combined strategies. The availability of the low molecular weight heparins makes possible short-term, outpatient treatment of those with a moderate or high probability while definitive diagnostic testing is awaited. Because the low molecular weight heparins are now widely accepted as safe and effective in the treatment of acute DVT, the major concern is the small risk of bleeding associated with a single dose of low molecular weight heparin. Although this risk is not well defined, it is certainly less than that associated with a standard 4-day to 5-day course of low molecular weight heparin. Such an algorithm is likely safe and warrants evaluation, although it is difficult to recommend in the absence of clinical trials.
Screening with D-dimer cross-linked fibrin degradation products can potentially be used to limit after hours examinations. Although sensitive for the diagnosis of venous thromboembolism, D-dimer measurements are quite nonspecific, and elevated levels may be associated with preeclampsia, malignancy, infection trauma, or recent surgery. The high sensitivity of D-dimer measurements makes it theoretically possible to exclude a diagnosis of DVT, although the low specificity and positive predictive value require confirmatory noninvasive testing for positive results. There are currently three methods of measuring D-dimer levels in blood: enzyme-linked immunosorbent assay (ELISA), latex agglutination, and whole blood agglutination assays. Several rapid ELISA assays are now available, returning results within 1 hr. From a practical standpoint, these rapid ELISA assays seem to have the best combination of convenience and sensitivity. However, all methods are somewhat limited by the extent of thrombosis, duration of symptoms, and the prior use of anticoagulants. Foremost among these are concerns that D-dimer measurements have a lower sensitivity for isolated calf vein thrombi. 7 D-dimer testing is probably most appropriate in outpatients with a low pretest probability of disease, in whom the negative predictive value is 99%–100%.
A combined strategy that uses an assessment of clinical probability, D-dimer testing, and venous ultrasound perhaps holds the greatest promise of safely limiting the number of negative ultrasound studies. Algorithms can be designed in which at least some patients can be initially managed on the basis of D-dimer results, with ultrasound confirmation as scheduling permits. Two recent studies have evaluated the usefulness of such algorithms in the emergency department setting.2,8 Both suggest that patients with a high pretest probability require duplex imaging, whereas patients with a low pretest probability and a negative D-dimer require no further testing. Unselected series have shown that 23%–50% of patients seen in the emergency department can be stratified into the low pretest probability group. 2 Unfortunately, these studies reach different conclusions with respect to moderate probability patients: one recommending routine duplex imaging and the other imaging only for those patients with a positive D-dimer. The former approach, although more conservative, reduced the number of required ultrasound studies by 23% at a significant cost savings. Although quite promising, all of these strategies require further validation, either in the literature or in the local institution.