
Abstract
Introduction
Color duplex ultrasound (CDU) is used to document the location and severity of disease in the arterial system. The purpose of this study was to determine the prevalence, location, and severity of disease in the aorto-iliac arterial segment in patients with signs and symptoms of peripheral arterial disease and undergoing routine lower extremity arterial CDU evaluation.
Methods
The charts of 45 randomly selected patients with suspected lower extremity peripheral arterial disease (PAD) who were undergoing routine extremity arterial CDU testing were retrospectively reviewed. Disease processes of the aorto-iliac segment were grouped into four categories: ectatic aorta (EA), abdominal aortic aneurysm (AAA), non–hemodynamically significant plaque (NHSP), and hemodynamically significant plaque (HSP). Disease findings were based on internally validated CDU criteria. Findings were considered significant if the patient had AAA or HSP.
Results
Of the 45 records reviewed, 8 patients did not have an aorto-iliac evaluation based on testing protocols, and 11 were excluded for nonvisualization of the aorto-iliac segment due to bowel gas or body habitus. Of the 26 remaining patients, 4 patients presented with normal findings (15%), 14 with NHSP (54%), 8 with AAA (31%), 7 with HSP (27%), and 2 with EC of the aorta (8%). When grouped by significant findings, 4 patients presented with AAA and HSP (15%), 4 with AAA only (15%), and 3 with HSP (12%).
Conclusion
Findings of disease in the aorto-iliac segment were noted in 85% of the patients in this population. Significant disease was present in 42% of the patients in this population. Evaluation of the aorto-iliac segment with CDU in patients with suspected PAD appears to have a significant yield; however, further investigation with a larger patient population and a comparison to other testing modalities is necessary.
Introduction
Atherosclerosis is a systemic disease that causes narrowing of the arterial lumen and weakening of the arterial wall. Stenosis created by a narrowed arterial lumen may decrease blood flow and pressure to tissues distal to the obstruction to such an extent that pain or nonhealing wounds may limit the activities of the individual or threaten the viability of the affected limb. Aneurysmal dilatation due to weakened arterial walls can lead to arterial embolization from laminated thrombus or may rupture, causing severe disability or death.
Patients presenting to the vascular laboratory with signs and/or symptoms of peripheral vascular disease generally do not have atherosclerotic disease limited only to the lower extremity arterial tree. Often, abdominal aortic aneurysm (AAA) and subcritical or borderline hemodynamic lesions go undetected during physiologic testing, requiring more expensive imaging studies or risky invasive procedures.
For years, duplex ultrasonography has been used in the noninvasive vascular laboratory to screen for the presence of AAA.1,2 Studies have shown excellent correlation with arteriography in the detection of aorto-iliac lesions.3–5 Others studies have demonstrated little difference in the ability of ultrasound to detect AAA when compared with computed tomography (CT) imaging.
The purpose of this study was to determine the prevalence of atherosclerotic lesions and arterial dilatations in the aorto-iliac segment based solely on non-invasive color flow duplex imaging in patients presenting to the vascular laboratory for noninvasive lower extremity arterial testing due to suspected peripheral vascular disease.
Materials and Methods
The charts of 45 patients referred to the vascular laboratory for noninvasive lower extremity arterial testing were retrospectively reviewed. The population comprised 20 male and 25 female patients (mean age 72.4 years, range 46–86) with signs and/or symptoms of peripheral arterial disease (PAD). Signs and symptoms of PAD included intermittent claudication, ischemic rest pain, suspected acute arterial occlusion, previously documented PAD of the lower extremity, and gangrene. Based on laboratory testing protocols and algorithms, patients underwent one or more of the following tests: continuous wave Doppler waveform analysis, pre- and poststress ankle-brachial indices (ABI), toe-brachial indices (TBI) with photoplethysmographic digital waveform analysis, and duplex evaluation of the aorto-iliac and femoro-popliteal arterial segments. All patients were asked to have nothing to eat or drink after midnight prior to the evaluation.
All examinations were performed on HDI 3000 or HDI 5000 color flow duplex units (Advanced Technology Laboratories, Bothell, WA). The aorto-iliac duplex evaluations were performed using a low-frequency curved linear array probe (C4-2).
Patients on whom the aorto-iliac evaluation was performed were grouped according to the findings in the following manner: within normal limits (WNL), non–hemodynamically significant plaque (NHSP), hemodynamically significant plaque (HSP), ectatic aorta (EA), and abdominal aortic aneurysm (AAA). Definitions of the findings are listed in Table 1. Findings were further categorized into not significant (NHSP and EA) and significant (AAA and HSP). Not significant were considered those conditions that did not need immediate attention or follow-up evaluations; significant findings were those conditions that required either immediate attention or diligent follow-up toward eventual management of progressive conditions. Findings were also compared with the presenting symptoms at the time of the evaluation.
Definitions for the Grouping of Findings
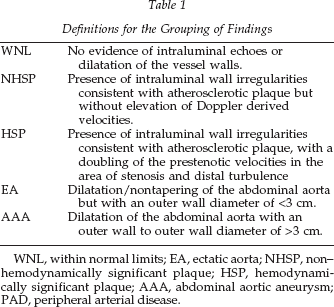
WNL, within normal limits; EA, ectatic aorta; NHSP, non– hemodynamically significant plaque; HSP, hemodynamically significant plaque; AAA, abdominal aortic aneurysm; PAD, peripheral arterial disease.
Findings were based solely on the duplex evaluation. In this patient population, and for the purpose of this study, findings were not confirmed by or compared with arteriography, CT, or magnetic resonance (MR) imaging. Additionally, findings were not compared with the physiologic test results of the lower extremity arterial duplex evaluation, patient gender, or risk factors for atherosclerosis.
Results
Patients on whom the aorto-iliac evaluation was not performed due to laboratory protocols (8), patients in whom the aorto-iliac findings were equivocal (3), and patients in whom the aorto-iliac segment was obscured by overlying bowel gas (8) were excluded from the study.
Of the 26 remaining patients, 4 (15%) were within normal limits, 14 (54%) had NHSP, 7 (27%) had HSP, 2 (8%) had EA, and 8 (31%) had AAA (Table 2). Some patients had more than one finding. Eighty-five percent (85%, 22/26) of this patient population had some finding consistent with atherosclerosis in the aorto-iliac segment. When findings were categorized by significance, significant findings were noted in 42% (11/26) of the patients in this study (Table 3).
Overall Findings
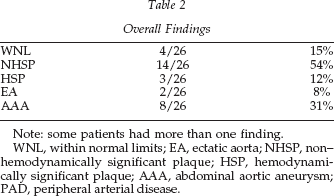
Note: some patients had more than one finding.
WNL, within normal limits; EA, ectatic aorta; NHSP, non– hemodynamically significant plaque; HSP, hemodynamically significant plaque; AAA, abdominal aortic aneurysm; PAD, peripheral arterial disease.
Significant Findings of Aortoiliac Disease in this Patient Population
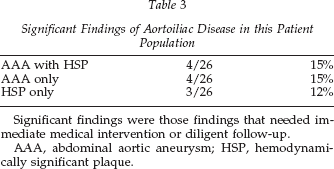
Significant findings were those findings that needed immediate medical intervention or diligent follow-up.
AAA, abdominal aortic aneurysm; HSP, hemodynamically significant plaque.
When compared with the patients’ symptoms upon presentation to the vascular laboratory, 16 patients presented with symptoms of claudication (61%), 4 had documented PVD without previous evaluation of the aorto-iliac segment (15%), 2 patients presented with gangrene (8%), 3 patients presented with suspected acute arterial occlusion (11%), and 1 patient presented with ischemic rest pain (4%).
Contrasting not significant and significant findings, 32% of patients presenting with claudication, 100% of patients presenting with PVD and rest pain, and 33% of patients presenting with suspected acute arterial occlusion had findings of either AAA or HSP, or both. Table 4 shows a breakdown of findings compared with clinical presentation.
Findings Compared to Clinical Presentation
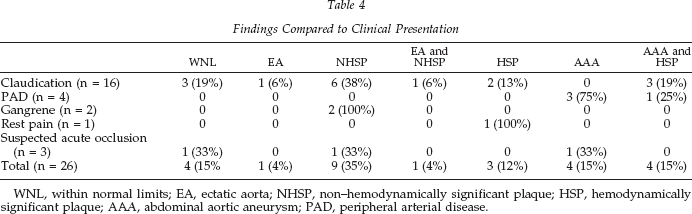
WNL, within normal limits; EA, ectatic aorta; NHSP, non–hemodynamically significant plaque; HSP, hemodynamically significant plaque; AAA, abdominal aortic aneurysm; PAD, peripheral arterial disease.
Discussion
Atherosclerosis, or arteriosclerosis obliterans disease (ASOD), is the most common cause of arterial occlusive disease in the United States. Atherosclerosis is responsible for the formation of arterial plaque, which narrows the vessel lumen, thereby limiting the supply of blood vital to the proper function of organs and tissues. Additionally, ASOD is associated with the presence of AAA in the majority (>90%) of patients.
Although ASOD is a widely distributed disease in the arterial tree, specific sites have a higher tendency toward development of disease than others. The aorto-iliac segment is second only to the superficial femoral artery at the level of the adductor canal in the formation of ASOD, with plaque in the aorto-iliac segment more common in nondiabetic patients. 6
Ultrasound evaluation of the aorto-iliac segment is considered by many to be a reliable, reproducible, risk-free, and relatively inexpensive method for detection of both AAA and arterial obstruction. Many studies have shown high sensitivity and specificity in the detection of aorto-iliac atherosclerosis and AAA. Currie et al. showed 91% sensitivity and 93% specificity, and conversely, Karacagil et al. demonstrated 93% sensitivity and 91% specificity in the ability of ultrasound to detect disease in the aorto-iliac segment when compared with arteriography.3,4 De Smet et al. also showed “excellent agreement (kappa 0.82) … between duplex … and arteriography.” 5 Arteriography, considered the gold standard for detection of stenosis, is unreliable in the detection of aneurysms due to the presence of laminated thrombus in many cases, substantially underestimating the size of the dilatation. Arteriography also carries the risk of complications not associated with ultrasound.
Color flow duplex imaging has been reported to be a valid screening method for AAA in several studies,7,8 with low interobserver variability. 9 Ultrasound generally underestimates the size of AAA in smaller aneurysms when compared with CT imaging 10 ; however, the differences in measurements between color duplex ultrasound (CDU) and CT were not significant. 11 A reason for the difference in measurements between the modalities may be the way in which the images are measured. Because CT uses perpendicular image slices to measure structure dimensions, any deviation in the course of the vessels due to tortuosity or displacement, which generally occurs in aneurysms, may result in measurements larger than those obtained by CDU. Standardizing the methods by which CDU images are obtained may reduce the variability of measurements compared with CT.
Indirect physiologic testing using segmental arterial pressures and volume pulse recordings (VPR) has been shown effective in isolating the level of arterial obstruction in the lower extremity; however, this has not been as effective at isolating aorto-iliac disease. Improperly sized or placed cuffs can produce an artifact that erroneously elevates pressures or improperly displays VPR waveforms. Decreased thigh pressures may also reflect the presence of superficial femoral or deep femoral arterial disease; falsely leading to the assumption that aorto-iliac disease is present. Indirect arterial testing modalities are also incapable of differentiating between severe stenosis and occlusion or documenting the presence of AAA. 6
Detection of AAA can be performed through the use of several methods, including physical examination, CT, and magnetic resonance MR imaging, and even X-ray, in addition to ultrasound.
Physical examination for AAA is reliable in subjects with abdominal girth <100 cm and in whom the AAA is rather large. This method of detection is subjective with relatively low sensitivity and positive predictive values. 2 CT and MR imaging are highly accurate in detecting the size and location of AAA; however, the time needed to perform the exams, cost of the procedures, and the potential exposure to ionizing radiation may make use of these modalities prohibitive. The use of X-ray to detect AAA relies on the presence of calcium in the aneurysm wall, and many false positive results have occurred as a result of tortuosity.
Of the 45 patients who were initially included in this study, 11/45 (24%) were excluded due to equivocal findings secondary to technical difficulties from overlying bowel gas (8/45, 18%) or poor technique (3/45, 7%). Changes in patient fasting, patient positioning, or sonographer technique could significantly improve the ability to visualize adequately the aorto-iliac segment.
In this patient population, there was a high yield of findings consistent with the presence of atherosclerosis (85%). Forty-two percent of the patients in this study demonstrated significant findings that may warrant intervention or observation for disease progression. Of the other 43% of patients with not significant findings of ASOD, mild atherosclerotic plaque or ectasia of the abdominal aorta may progress at some point to require intervention.
Recent studies espouse the benefits of AAA screening programs; however, most studies had randomly selected patients based on age, gender, and ability to participate, not based on suspected atherosclerotic disease.12,13 This study shows a much higher yield of AAA in patients with signs or symptoms of lower extremity ASOD (n = 8; 31%) than those in the screening studies (approximately 5% for both studies). Although AAA screening of particular patient populations has been shown effective at reducing the risk of disability and death from AAA, this study demonstrates the importance of evaluation of the aorto-iliac segment in patients at higher risk for atherosclerosis. By including duplex evaluation of the aorto-iliac segment, the vascular laboratory was able to isolate the location and severity of atherosclerotic disease in this patient population.
Based on patient symptoms, only those with gangrene (n = 2) had no evidence of significant findings of aorto-iliac disease; however, both patients did have plaque associated with atherosclerosis. Further review of the patients’ records revealed both patients to have diabetes, although this was not a parameter investigated thoroughly in this study. Eighty-one percent of patients with symptoms of intermittent claudication had findings consistent with ASOD, with 32% demonstrating significant findings. This is significant, as many of the patients presenting to the vascular laboratory for noninvasive lower extremity arterial testing describe claudication symptoms. Because most claudicants are not in jeopardy of limb loss, the findings of aorto-iliac disease, particularly AAA, may have gone undetected, delaying intervention or follow-up until an adverse event occurred.
Conclusion
Direct visualization of the aorto-iliac segment with color flow duplex imaging demonstrates a high yield of significant and not significant atherosclerotic disease in patients with signs and symptoms of lower extremity arterial occlusive disease. A prospective study comparing symptoms, risk factors, and the results of noninvasive and invasive testing modalities may further assist in the development of algorithms for investigating the aorto-iliac segment during non-invasive lower extremity arterial testing.