
Abstract
Background
Neurofibromatosis (NF) is a common genetic disorder responsible for the development of neuroectodermal tumors throughout the body. Although vascular involvement with these growths is uncommon, arteriovenous malformations, aneurysms, stenosis, and occlusions have been reported. We report a case of a patient with NF who presented with a ruptured internal carotid artery aneurysm and then developed a common carotid pseudoaneurysm with subsequent hemorrhage during repair. The use of duplex ultrasound (DU) in the initial diagnosis and follow-up management of this patient will be discussed.
Case Report
A 31 year-old man with a history of NF presented to the emergency department with pharyngitis and right neck swelling. The initial DU revealed a 2.4-cm distal right internal carotid artery (RICA) aneurysm, which was treated with a covered stent. On the first postoperative day, a new wall irregularity in the right common carotid artery measuring 1.6 cm and a high resistant Doppler signal in the RICA suggesting distal occlusion were demonstrated by DU. A transcranial duplex supported the ICA occlusion by demonstrating cross filling from the left to the right through the anterior communicating artery. Because of increased neck swelling, DU was repeated on the third day. At the site of the previously noted CCA irregularity, a 3.4-cm pseudoaneurysm had developed. During attempted repair in the endovascular suite, the patient developed massive hemorrhage. To control bleeding, intravascular coils were used to occlude the right external carotid artery, RICA, and right common carotid artery. An intraoperative DU confirmed the successful occlusion of the carotid vessels.
Conclusion
DU provided an accurate initial and follow-up diagnosis of the carotid aneurysms in a patient with vascular complications from NF.
Background on Neurofibromatosis
Neurofibromatosis (NF; also known as von Recklinghausen's disease) is a genetic disease affecting 1 in 3000–4000 people 1 . Approximately 50% of the patients, however, do not have family history of NF, and instead the disease is caused by a new genetic mutation. 2 The features of NF were first described by a German pathologist, Friedrich von Recklinghausen, in 1882 and are characterized by nerve tumor growths. Neuromas arise in or can attach to nerve trunks anywhere in the body. These growths are caused by abnormalities in the neuroectodermal layer during the embryonic stage, which is responsible for the formation of the epidermis and epidermic tissues, such as nail, hair skin, the nervous system, glands of the skin, and external sense organs. 3 Therefore, the disease presents with an extremely variable and unpredictable course. Clinical manifestations include café au lait spots, axillary freckling, ocular Lisch nodules, skeletal abormalities, and multiple neurofibromas. 2
One of the less appreciated but potentially significant complications of NF involves the vascular system. Autopsy reports from patients with NF (who died from other causes) cite the presence of vasculopathy in 44% of these patients. 4 Because vascular complications in patients with NF are rare, a standardized classification system does not exist, and the histological causes have been subject to some controversy. 5 Vascular lesions may involve stenosis, occlusion, aneurysms, and arteriovenous fistula formation. These abnormalities can occur in the aorta, renal arteries, mesenteric, and intracranial or extracranial cerebral arteries. The most common anomaly involves gradual narrowing of an artery with eventual occlusion, 6 which frequently is reported as stenosis involving the origin of the renal arteries and may cause hypertension and can exacerbate the formation of aneurysm. 7 Similar lesions are also infrequently encountered with an appearance similar to Moyamoya. This stenosis occurs gradually, allowing for extensive collateralization, which gives the classic radiological appearance of “a puff of smoke.” Aneurysms typically arise in the larger cerebral arteries and primarily involve the ICA, middle cerebral, anterior communicating, and basilar. 8 There have also been a few reports of aneurysm formation in the cervical vertebral, mesenteric, aorta, and renal arteries. 2
Case Report
A 31-year-old man with known NF presented to the emergency room complaining of right neck pain and swelling that had been present for 1 week and worsened during the previous 12 hours. His family history was significant for NF, and he had some scattered cutaneous neurofibromas. He had been seen earlier by his primary physician and was receiving antibiotics for pharyngitis. This report describes how duplex ultrasound (DU) was used as the primary diagnostic and follow-up imaging modality for this NF patient who developed serious vascular complications.
Hospital Course
The initial DU revealed aneurysmal dilatation of the cervical right internal carotid artery (RICA) measuring 2.4 cm (Figure 1). Imaging and spectral Doppler of the right common carotid artery (RCCA), right external carotid artery, and vertebral arteries were normal. Lateral to the RCCA, there was a heterogeneous collection identified by B-mode ultrasound that was consistent with a hematoma. Computed tomography confirmed these findings but suggested that the RICA aneurysm was ruptured (Figure 2). The RICA aneurysm was treated emergently with an endovascular covered stent. Postdeployment angiography revealed successful exclusion of the aneurysm (Figure 3A and 3B).

Initial presentation day 1. Gray-scale image of the RICA aneurysm in a transverse view.
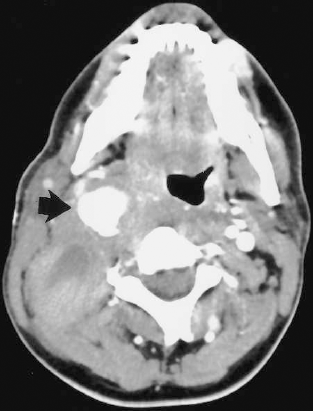
Initial presentation day 1. Computed tomography image of the RICA aneurysm (black arrow) suggests the aneurysm ruptured.

Initial angiogram day 1. (A) Angiogram of the ruptured RICA aneurysm. (B) Postdeployment angiography with successful exclusion of the aneurysm.
On day 2, a second DU was performed. Although gray-scale and Doppler could not penetrate the stent material, spectral Doppler signals in the ICA immediately proximal to the stent were high resistant, suggesting a distal occlusion (Figure 4). Additionally, gray scale showed a focal dilation of the distal RCCA measuring 1.6cm by 1.4cm (Figure 5). Transcranial Doppler performed on the same day revealed retrograde right anterior cerebral artery (ACA) flow by color Doppler (Figure 6). Spectral analysis confirmed retrograde right ACA flow through a patent anterior communicating artery. This cross filling supported the extracranial DU examination.
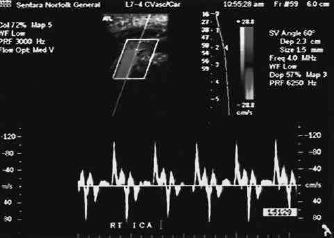
Day 2. Spectral Doppler in the RICA proximal to the stent is high resistant suggesting distal occlusion.

Day 2. Gray-scale finding of the distal RCCA focal dilatation.
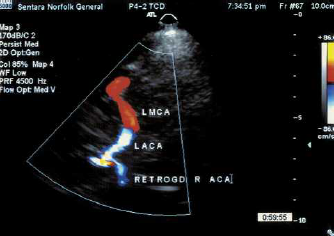
Day 2. A TCD supports the extracranial finding of RICA occlusion with cross filling from the left to the right. Color Doppler shows the retrograde right ACA.
Because of increased neck swelling, we performed DU again on the third postoperative day. Gray-scale imaging revealed significant expansion of the RCCA into a pseudoaneurysm that now measured 3.4 by 1.9 cm (Figure 7). The neck of the pseudoaneurysm measured 1.6 cm across and the dome contained flow by color and spectral Doppler imaging. In the RICA stent, which could now be penetrated by color and spectral Doppler, there were systolic blips still suggesting a distal RICA occlusion.

Day 3. Gray scale image of the RCCA pseudoaneurysm at the previous site of the dilatation.
The patient was taken to the endovascular suite for repair of the RCCA pseudoaneurysm. Complications occurred early in the procedure because of hemorrhage, and the patient was intubated to preserve his airway. Owing to the inability to control bleeding, the RCCA, RICA, and external carotid artery were occluded with intravascular coils (Figure 8). DU showed complete occlusion of the vessels by gray scale, color, and spectral Doppler imaging.

Day 3. Angiography shows the RCCA pseudoaneurysm (large black arrow), the RICA covered stent (curved arrow), and the coils in the proximal and distal ICA as well as the ECA (open black arrow).
The patient recovered from this procedure without neurological deficits and was transferred from the intensive care unit to a step down unit 14 days after his admission. Unfortunately, 5 days later, he sustained a cardiac arrest and could not be resuscitated. An autopsy revealed that the cause of death was a massive hemorrhage from a ruptured right subclavian aneurysm.
Discussion
Although the association between NF and vascular disease is uncommon, it is well recognized. Reubi pioneered the histological study of NF patients with vascular complications in 1945 by describing 3 types of lesions involving arteries less than 1 mm in diameter. 9 In 1973, Sayler and Sayler suggested that the proliferation of Schwann cells caused all the vascular complications and classified them into 4 groups. 10 In 1974, Greene et al. described 2 basic types of lesions associated with NF. The small vessels contain aggregates of smooth muscle cells causing mesodermal dysplasia, whereas the large vessels contain perivascular neurofibromas that result in degenerative changes of the adjacent vessel wall. 11
NF patients with vascular involvement are known to have fragility of the vessel wall and extensive vascularity in the surrounding neurofibromatous tissue. 3 Therefore, vascular complications are unpredictable and may manifest with varying degrees of severity. In our patient, these characteristics and the distal cervical location of the RICA aneurysm made open repair potentially disastrous. Although a few reports of covered stent grafts in the internal carotid arteries have been published, they report a risk of embolization or graft occlusion, as seen in our patient.12,13 In our case, the cause of the occlusion was not clear. Fortunately, with sufficient collateralization through the Circle of Willis he did not suffer any neurological defect.
One of the most surprising elements of this case was the rapid development of the RCCA pseudoaneurysm over the course of 48 hours that formed without a known injury. This demonstrates the fragile nature of the artery. However, it is possible that the passing of catheters and stents during his first intervention was sufficient to injure the artery and initiate the formation of the pseudoaneurysm.
A common clinical problem in the management of NF patients with vascular disease is severe bleeding. A hemorrhage can occur perioperatively as the result of loss of arterial wall integrity from necrotic and friable vessels. 3 In our patient, it is likely that these types of alterations in the artery wall were responsible for the development of the RICA aneurysm, its rupture, and the subsequent development of the RCCA and subclavian artery aneurysms. In the end, intravascular coiling was used to thrombose the entire right carotid system.
We believe that the right neck hematoma was most likely the result of the RICA rupture. Its homogenous echo content indicated that it occurred with close timing to the initial rupture, furthermore, there was no expansion during subsequent DU imaging and its presence was confirmed by the initial computed tomography and at autopsy.
The cause of the lethal right subclavian artery aneurysm and rupture are unknown. However, like the RCCA pseudoaneurysm, it developed rapidly and was not appreciated on the baseline angiogram. Unfortunately with NF, there are no clinical characteristics that can help predict which patients might deteriorate suddenly. Deaths caused by vascular disease occur, on average, 9 years earlier in patients with NF when compared with the overall population. 1
In summary, NF can be responsible for vascular complications that may develop suddenly and result in an unpredictable course. Our case demonstrates how DU can play an important role in the diagnosis and follow-up care of these rare and often deadly complications in patients with NF.