
Abstract
Purpose
Patients with chronic venous insufficiency have been successfully treated with foam sclerotherapy. Reports of cerebral and respiratory symptoms after the foam procedure have been related to an open foramen ovale (PFO) between the right and left sides of the heart. This work evaluated the value of ultrasonography to demonstrate that bubbles may traverse a PFO and may be detected at the middle cerebral artery.
Methods
Patients describing cerebral or respiratory symptoms or suspected of having a PFO entered this study. Cerebral symptoms included visual disturbance, lightheadedness, dizziness and migraine. Respiratory problems included cough. A total of 20 patients had transthoracic echocardiography (TTE), and 12 had transcranial Doppler (TCD) of the middle cerebral artery.
Results
TTE detected bubbles in the left heart in 13 (65%) of 20 patients. The 12 TCDs were performed in nine patients with positive and three with negative TTE evaluation; five TCDs were positive for emboli at the middle cerebral artery. All five patients had positive transthoracic echocardiography.
Conclusions
This single-institution evaluation for quality control demonstrated that 1) patients with cerebral or respiratory symptoms after foam sclerotherapy may have PFO; and 2) patients with patent PFO may embolize the gas particles to the brain. Therefore, patients with known PFO must be evaluated before foam injection, and patients that are candidates for this treatment may have to be screened for PFO.
Introduction
In addition to classical junction ligation and stripping of the saphenous veins, thermal and chemical ablation have been added to the armamentarium for treatment of chronic, superficial, venous valvular insufficiency.1–4 Phlebectomy has become an ambulatory procedure. 5 Signs and symptoms 6 related to lower-extremity venous hypertension can be minimized or eradicated. The unacceptable presentations of telangectasias, reticular and varicose veins, edema, skin changes, and ulcers 6 can be vastly ameliorated. Thermal ablation, performed either with laser or radiofrequency energy, is better tolerated than stripping. 7 Liquid sclerotherapy, in the era of the catheter, has expanded toward chemical ablation of the saphenous veins. 8 Foam sclerotherapy has evolved as gases mixed with liquid have improved the sclerosing efficacy.9–18 Ultrasound-guided foam sclerotherapy (UGFS) has allowed the chemical ablation of veins unseen by the naked eye and has expanded the horizons of treatment. UGFS can be performed alone or as a complement to stripping, ambulatory phlebectomy, and/or thermal ablation. UGFS is a practical and relatively less expensive procedure.
Every new procedure, however, is carefully tested in every detail. Instead of relying solely on outside expertise and multicenter, international trials, the Morrison Vein Institute (MVI) has the philosophy to test every innovation in-house. Reports of cerebral and respiratory symptoms after the foam procedure have been related to a patent foramen ovale (PFO) or a right to left shunt in the heart. This work is a continuation of our initial report and includes additional patients and demonstrates the value of 1) ultrasonography to detect bubbles in the heart and 2) transcranial Doppler to detect emboli at the middle cerebral artery.
Methods
A routine to test for PFO is evolving. Subjects suspected of having PFO are tested before or during the first UGFS session. Other subjects are treated normally and are tested only if they develop symptoms. Therefore, the first UGFS is performed based on a PFO testing mentality. At MVI, testing includes transcutaneous ultrasound (US), transthoracic echo (TTE), and transcranial Doppler (TCD).
Patient Population
Patients describing cerebral or respiratory symptoms or suspected of having a PFO entered this study. Cerebral symptoms included visual disturbance, lightheadedness, dizziness and migraine. Respiratory problems included cough. A total of 20 patients had TTE and 12 had TCD of the middle cerebral artery (MCA).
Transthoracic Echo
Subjects were in lateral decubitus position facing the echocardiographer. A high-end Siemens/Acuson Sequoia scanner was used. The four chambers of the heart were insonated with a 3-MHz probe.
Transcranial Doppler
Blood flow through the middle cerebral artery (MCA) was monitored via a temporal window. A headset was used to hold the TCD transducers against the transtemporal window. A 2-MHz transducer connected to a Nicolet/Viasys unit was used to monitor MCA flow continuously. Not all patients had adequate bilateral monitoring.
Foam Preparation
The foam was prepared using the two-syringe, three-way stopcock method described by Tessari et al. 19 The liquid, polidocanol diluted to 1%, was mixed with either air or carbon dioxide. The foam was injected distally first, most commonly in superficial tributaries of the calf. The small saphenous vein was also treated by UGFS. One or two injections were done during these PFO evaluation sessions. Several patients were asked to perform a calf pump exercise to promote progression of the foam to the heart for PFO evaluation.
Results
Timing between injection and detection of bubbles in the right heart varied between 9 and 59 seconds. TTE detected bubbles in the left heart in 13 (65%) of 20 patients (Figure 1). These 13 patients reported the following symptoms: migraine (n = 5), visual disturbance (2), cough (2), lightheadedness (1), sore throat (1), dizziness (1), chest tightness (1), and possible transient ischemic attack (1). The 7 patients without bubbles in the left heart reported visual disturbance (n = 2), migraine (1), shortness of breath (1), dizziness (1), and numbness (1). The 12 TCD were performed in 9 patients with positive and 3 with negative TTE evaluation; five TCDs were positive for emboli at the MCA (Figure 2). All five patients had positive TTE. Four of these patients reported lightheadedness, sore throat, cough and chest tightness, and migraine.

Transthoracic echocardiographic (TTE) detection of bubbles in the heart after ultrasound-guided foam sclerotherapy (UGFS) of leg veins.
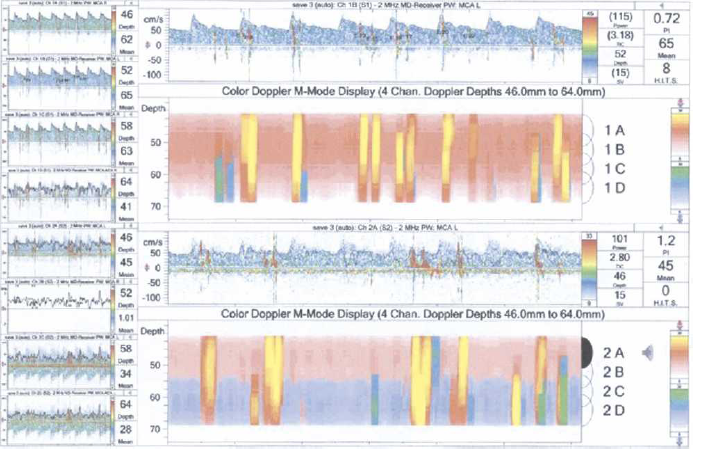
Transcranial Doppler (TCD) detection of gas emboli in the middle cerebral artery after ultrasound-guided foam sclerotherapy (UGFS) of leg veins.
Discussion
The MVI program for evaluation of new procedures has demonstrated that foam propagates from the site of injection to the deep veins and to the right heart. Epidemiological data indicate that about one-fifth to one-quarter of the general population may have a patent foramen ovale in the heart. 20 A select group of patients with greater probability of having a PFO was entered in this study. The incidence of bubbles in the left heart was about three times greater than expected for the general population. About half of the patients with a positive TTE had the findings confirmed by TCD. As experience is gained with this monitoring technique, one expects a higher detection rate. Nevertheless, one should not expect that all bubble pathways go through the middle cerebral artery of one side or another. The TCD did not contradict a negative finding by TTE. Although a slight majority of patients reported symptoms of one degree or another, the numbers and the consistency were not enough for an evaluation at this stage.
This study was intended to test for PFO. Therefore, patients were injected without elevation of the legs and were asked to exercise the calf muscles. Leg elevation is being prescribed based on the concept that bubbles go up against the forces of gravity. In contrast, however, the hypothesis exists that bubbles mix with blood, and if blood moves toward the heart, then foam also moves toward the heart.
Testing every patient for PFO is too cumbersome, often unproductive, and unaffordable. Therefore, protocols are being developed to select patients for PFO diagnostic evaluation. This examination requires foam injection for the TTE to be more efficient and more sensitive than color flow TTE alone. The bubbles are more readily detected by US. Selection of these patients is being done either by past clinical history or by clinical response to the first therapeutic foam injections.
In summary, this quality control program demonstrated that sclerosing foam left the superficial veins and navigated toward the heart after the usual flow of blood. Foam reaching the right heart may traverse to the left heart and may be detected at the middle cerebral artery. Awareness of the practicing physician must be enhanced to recognize patients with past story of PFO, or to detect the early signs and symptoms of an active right to left shunt early during UGFS.