
Abstract
Introduction
Thrombin injection for the treatment of arterial pseudoaneurysms has been performed safely and effectively for many years. These pseudoaneurysms typically develop after a performance of a percutaneous procedure that uses the common femoral artery for access. This technique has also been applied effectively for pseudoaneurysms arising from other arteries. This report presents the first use of thrombin injection technique with ultrasound guidance for ablation of a gluteal pseudoaneurysm.
Case Report
A 44-year-old man presented with complicated diverticulitis and was treated with two operations. Afterward, he had an infected pelvic fluid collection that was drained with computed tomography-guided, trans-gluteal approach. After drain removal, pain developed in the right buttock, and a gluteal pseudoaneurysm was diagnosed, which was successfully treated with an ultrasound-guided, thrombin injection.
Conclusions
Complications resulting from trans-gluteal drainage are unusual. Pain and hemorrhagic complications have been documented and are more common when a transpiriformis muscle approach is mandated by location of the fluid collection. Thrombin injection provided a rapid, safe, and effective treatment for this complication. This approach required no significant anesthesia and recovery was less than 2 days. Ultrasound demonstrated clearly that the gluteal fluid collection was a pseudoaneurysm and that it demonstrated characteristics favorable for thrombin injection.
Introduction
Ultrasound-guided thrombin injection for the definitive treatment of arterial pseudoaneurysm was first described by Liau et al. in 1997. 1 This procedure is most often used for pseudoaneurysms that arise from the common femoral artery after a percutaneous procedure. Alternatives for treatment of this entity include doing nothing, which puts the patient at risk for significant uncontrolled bleeding. Ultrasound-guided compression offers low risk for effective treatment but causes significant pain to the patient and puts the ultrasound technologist at risk for chronic injuries. In addition, the failure rate of this procedure can be high. 2 Surgery is very effective but is costly and conveys the highest risk to the patient for treatment of pseudoaneurysms. At our institution, thrombin injection is very effective (failure rate <1%), fast (total procedure time is typically less than 10 min), safe (no major complications, to date), and well-tolerated by both the patient and the technologist. A recent review article documents findings similar to these. 2
Computed tomographic (CT) guidance of transgluteal drainage of pelvic fluid collections was first described by Butch in 1986. 3 This type of procedure is performed percutaneously, and the operator typically drains infected pelvic collections that frequently develop after laparotomy, appendicitis, or diverticulitis. If successful, this drainage may allow the patient to avoid surgery altogether, or delay an operation until they have recovered from systemic effects of these infections. According to one source, they may comprise approximately 20% of all percutaneous drains that are placed to treat complications resulting from elective colorectal surgery. 4 Few complications resulting from this type of drain placement have been reported. 5 Pain is the most common complaint, and may indicate potential damage to significant nerves. Pain can develop at the time of placement or after the procedure. Hemorrhage and pseudoaneurysm formation also have been reported. 5 Bleeding complications are diagnosed by CT scan and typically develop from arterial transections caused by the needle, sheath, or drain passage. The bleeding usually occurs when the drain is removed because the initial arterial injury is tamponaded by the drain. This effect is released when the drain is removed, and a hematoma, pseudoaneurysm, or hemorrhage can result. These complications have been treated with angiography and coil embolization of the artery from which the bleeding arises. 6
Ultrasound-guided thrombin injection has been used in to treat pseudoaneurysms arising from arteries other than the common femoral. These reports include pseudoaneurysms arising from the radial, brachial, subclavian, and axillary arteries.7–10 The current report describes successful treatment of a gluteal pseudoaneurysm with thrombin injection. This pseudoaneurysm occurred after the removal of a transgluteal percutaneous drain, which was used to treat an infected pelvic fluid collection.
Methods
A 44-year-old man was diagnosed with diverticulitis. He had abdominal pain, which prompted evaluation with a CT scan. Free air was identified, but his symptoms improved with conservative management (oral antibiotics and bowel rest). Barium enema was subsequently performed to confirm significant diverticula's in the sigmoid colon. Elective sigmoid colectomy was recommended and eventually performed. He initially recovered uneventfully, but several weeks after surgery, he developed a small bowel obstruction. This did not improve after nasogastric suctioning and bowel rest. Another laparotomy was performed, and significant adhesions were lysed and an ileostomy was performed. After this operation, he developed systemic symptoms of infection. A CT scan demonstrated a significant pelvic fluid collection. This collection was drained with the use of a transgluteal, CT-guided approach. The drain was left in place for 2 weeks and removed once the fluid collection had resolved. The patient experienced right buttock pain immediately after drain removal. Follow-up CT scan demonstrated a fluid collection with in the piriformis muscle (Figure 1). Intravenous contrast was used for this study, but active flow in this collection was not demonstrated. At this point, he was referred to our vascular surgery clinic for evaluation. Ultrasound investigation demonstrated active arterial flow in this collection (Figure 2). A long neck, emanating from a gluteal artery was demonstrated (Figure 3). Informed and written consent was obtained for thrombin injection. Alternative treatments were offered, including serial imaging of this pseudoaneurysm, ultrasound-guided compression, coil embolization, and surgical ablation of the pseudoaneurysm.

A large, complex fluid collection is identified in the right piriformis muscle.

Color flow imaging of the fluid collection pictured in Figure 1 demonstrates arterial flow.
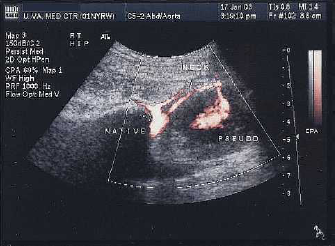
Color flow imaging demonstrates flow through the neck of the pseudoaneurysm and the proximity of the native gluteal artery.
The patient was placed in a prone position. The right buttock and flank were prepped and draped. A sterile cover was placed over the ultrasound probe. The technologist and surgeon wore sterile gloves. B-mode ultrasound was used to identify the needle tip as it entered into the pseudoaneurysm. Color flow imaging was then used as a small amount of topical, rehydrated thrombin was gently injected.
Results
Flow in pseudoaneurysm ceased abruptly. The patient noted immediate improvement in his pain. The native arteries were imaged and found to be patent and functioning normally. The patient was admitted to the hospital for 4 hr of bed rest after the procedure and 23 hr of observation. The next morning, the fluid collection was imaged again, and no flow was demonstrated in the pseudoaneurysm. The patient was discharged home, and follow-up was arranged by his local surgeon.
Discussion
Transgluteal, CT-guided drainage has provided a minimally invasive option for drainage of pelvic fluid collections for 20 years. 5 A very short list of complications has been reported with this approach. However, placement of the drain through the piriformis muscle has been documented to carry a greater rate of complications. 5 Pain and hemorrhagic complications have resulted when the location of the fluid collection mandates access through this muscle. The patient described in this report had a collection that needed to be approached through the piriformis muscle, and he did have a subsequent bleeding complication. To our knowledge, this is the first report of percutaneous, ultrasound-guided, thrombin injection utilization for treatment of this complication. Previous reports have documented successful treatment of this complication with angiography and embolization. 6 Thrombin injection, however, may offer a more limited risk profile and equivalent efficacy.
The CT examination after the formation of a pseudoaneurysm did not clearly demonstrate flow in the piriformis muscle collection. Ultimately, ultrasound examination, which demonstrates real-time flow, clearly identified the collection as a pseudoaneurysm. In addition to being critical for the safe treatment of this entity, ultrasound evaluation was the only imaging technique used that determined a firm diagnosis and clearly demonstrated a neck from the native artery. This important anatomic finding allowed us to offer thrombin injection with confidence that we would have success and avoid complication.
Thrombin injection has provided less-invasive and effective treatment for arterial pseudoaneurysms. 2 Ultrasound guidance was added to this procedure in 1997 with Liau et al.'s report. 1 This combination of percutaneous treatment for pseudoaneurysms and real-time imaging can allow clinicians to treat pseudoaneurysms in locations other than the femoral artery. The use of thrombin injection for complications of percutaneous procedures performed utilizing the arteries of the upper extremity has been reported.7–10 Treatment for hemorrhagic complications of transgluteal drains has also been reported, but angiography and percutaneous embolization were used to treat the pseudoaneurysms in those cases. 6
Footnotes
Acknowledgment
We recognize Karen V. Knight, MSLS, Medical Education Librarian, University of Virginia, Claude Moore Health Sciences Library. She performed all of the MEDLINE® (Medical Literature Analysis and Retrieval System Online) searches related to this work.