
Abstract
Introduction
Hepatic artery aneurysm is a rare and life-threatening lesion. Patients with hepatic artery aneurysm are often asymptomatic, which makes diagnosis difficult. Early diagnosis is essential because of the high risk of rupture. The following case describes an incidental finding of a large hepatic artery aneurysm.
Methods
A 74-year-old woman presented to the vascular lab for a renal artery evaluation. The patient had hypertension and chronic renal failure with elevated blood urea nitrogen and creatinine. Evaluation of the abdominal aorta was also requested because of a palpable, pulsatile abdominal mass and abdominal bruit. The patient additionally stated epigastric and right upper quadrant pain for the previous 6 months.
Results
The renal arteries displayed normal flow velocities without evidence of stenosis. Bilateral kidneys did exhibit parenchymal disease. Examination of the abdominal aorta demonstrated an infrarenal abdominal aortic aneurysm measuring 6.4 cm. In the proximal abdomen, at the level of the patient's pain, a large 11-cm aneurysm was identified. because of the large size of the aneurysm causing displacement of the vasculature, the artery of origin was not positively identified. To further delineate this lesion, the patient underwent computed tomography and angiography; however, these were also unsuccessful. The patient was eventually brought to the operating room for surgical repair of this aneurysm as well as her infrarenal AAA. Intraoperatively, the aneurysm was found to be originating from the hepatic artery.
Conclusion
Although a rare finding, hepatic artery aneurysm can be identified and evaluated with ultrasound. Additional testing with computed tomography and angiography helps to define the arterial source and location of the aneurysm, as well as collateral flow to the liver if the hepatic artery is compromised. Once identified, these lesions need to be surgically or interventionally treated due to their high mortality rate.
Introduction
Hepatic artery aneurysm is a rare and potentially life-threatening lesion. The following case presents some of the imaging challenges with hepatic artery aneurysm and will be followed by a review of the literature. In this case study, a 74-year-old woman with hypertension and chronic renal failure was referred to the vascular lab for a renal artery examination. Abdominal aorta evaluation was also requested because of a palpable, pulsatile abdominal mass, abdominal bruit, and 6-month epigastric and right upper quadrant abdominal pain
Methods
The fasting patient was evaluated with the Acuson Sequoia 512 (Siemens Company, Redmond, CA) diagnostic ultrasound machine; using a 6-2 MHz curved transducer. B-mode imaging, color flow and spectral Doppler were all used during the examination. Routine renal artery and aortic duplex imaging were performed.
Results
The abdominal aorta was evaluated in transverse and longitudinal planes from the proximal to distal abdomen. The mid segment of the aorta demonstrated an infrarenal aneurysm measuring 6.4 cm in greatest diameter. The abdominal aorta was tortuous with 2 separate 90-degree bends in the proximal vessel (Figure 1).
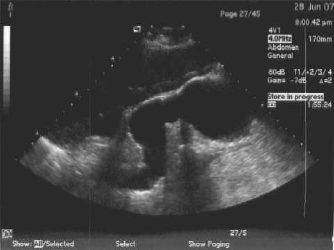
Image of the abdominal aorta demonstrates the infrarenal aneurysm and proximal tortuosity.
Attention was then turned to the proximal abdomen which demonstrated a large 10.9 × 11.0 cm pulsatile mass with a smooth outer border and contained mural thrombus (Figure 2). An inner chamber with irregular borders was visualized with active swirling blood flow (Figure 3). A single vessel into this aneurysm chamber was visualized, and bi-directional flow was obtained. The origin of this vessel was difficult to determine because of the displacement of the vasculature created by the aneurysm. The SMA, however, was ruled out as the arterial source.

The large aneurysm demonstrates a smooth outer border with an irregular inner chamber with mural thrombus.
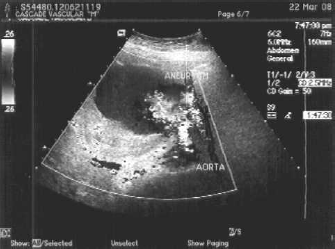
Swirling blood flow is detected within the aneurysm.
The renal artery duplex was then completed. The renal arteries displayed normal flow velocities without evidence of stenosis. Bilateral kidneys did exhibit resistive flow pattern, consistent with parenchymal disease.
A noncontrast CT was later performed showing a large 10.6 × 10.1 × 8.9-cm aneurysm (Figure 4). Because of the patient's renal failure, contrast injection was not performed. The arterial source was not positively identified, although it appeared to be related to one of the branches of the celiac artery.

Noncontrast CT of the abdomen shows a large aneurysm with wall calcifications.
A subsequent limited angiogram, because of the patient's renal failure, showed a patent celiac, left gastric, and splenic arteries and also a large amount of flow within the aneurysm, which was very slow to dissipate. The arterial source of the aneurysm was still not positively identified.
Because of continuing pain, the patient was thought to be at risk for aneurysm rupture and surgical repair was scheduled. Intraoperatively, the aneurysm was found to be originating from the hepatic artery. Outflow from the aneurysm into the hepatic artery was not identified. After gaining control of the aorta, the aneurysm was opened and thrombus within the aneurysm was evacuated. It was felt the patient had adequate collateral flow into the liver; therefore, the hepatic artery was ligated. The hepatic artery origin into the aneurysm cavity was oversewn, leaving the left gastric and splenic arteries intact.
The infrarenal aortic aneurysm was then repaired with an aorto-biiliac arterial bypass. The patient tolerated the procedures well, and there were no intraoperative complications. The patient was discharged from the hospital on postoperative day 5 and remains well. Subsequent abdominal ultrasound and CT exams have shown the aneurysm sac to be gradually decreasing in size.
Discussion
Disease Process
Hepatic artery aneurysms are uncommon with an estimated incidence of less than 0.25%. 1 The hepatic artery is the fourth most common site of intra-abdominal aneurysm from any cause following the infrarenal aorta, iliac artery, and splenic artery.1,2 A total of 80% of hepatic artery aneurysms are extrahepatic and, of these, 63% affect the common hepatic artery.2–4 They are life-threatening lesions because free rupture occurs into the abdominal cavity and containment is unusual. 4 There are various etiologies for hepatic artery aneurysm. Historically, mycotic infection accounted for most hepatic artery aneurysms.1,3,4 Today, atherosclerosis, infection, and trauma account for most cases. 2 Less-common causes include polyarteritis nodosa, tuberculosis, periarterial inflammation (caused by cholecystitis or pancreatitis), fibromuscular dysplasia, trauma, surgery (orthotopic liver transplant or hepatic tumor embolization), and diagnostic instrumentation. 1 The average age of presentation is often in the late forth and fifth decades of life with 65% of cases reported in men. 2
Presentation
Hepatic artery aneurysms often are asymptomatic and are rarely palpable on physical examination. 3 Large aneurysms may be associated with a pulsatile mass and/or an abdominal bruit. 1 In 80% of cases, rupture of the aneurysm is the first clinical manifestation. 1 Of the patients who present with clinical symptoms, abdominal pain is found in 55%, with complaints often of vague right upper quadrant or epigastric pain.1,3,4 Gastrointestinal hemorrhage can occur up to 46% of symptomatic patients. 1 Rupture of hepatic artery aneurysms occurs into the hepatobiliary tract and the peritoneal cavity with equal frequency. 3 Rupture into bile ducts often is responsible for the characteristic findings of hematobilia. 3 The classic symptom triad of epigastric pain, hematobilia and obstructive jaundice is only present in up to 33% of cases.1,2,4
Diagnosis
Early diagnosis of hepatic artery aneurysm is essential because of the risk of rupture. Mortality associated with rupture continues to be exceedingly high. 3 In the past, the diagnosis of hepatic artery aneurysms was made most often at autopsy or at times of surgical exploration for major complications of these lesions. 3 Various diagnostic imaging modalities can be used to properly diagnose these aneurysms.
Ultrasound is an excellent noninvasive method in the evaluation of the liver and porta hepatis for the presence of these lesions. 1 The aneurysm can appear as a mixed echogenic mass with varying proportions of cystic and solid components, depending on the extent of thrombus. Calcifications can occasionally be seen in the wall of the aneurysm. 1 Doppler ultrasound can aid in differentiating vascular from other types of masses, as well as differentiating aneurysms from other vascular abnormalities, such as arteriovenous fistulas or malformations. 1 Doppler ultrasound plays a significant role in the follow-up of patients who undergo embolization. 1
Abdominal CT can demonstrate an aneurysm, although the artery of origin is not always clear. CT scans must be performed with a contrast medium for proper diagnosis. 2 Three-dimensional spiral CT may allow a definitive diagnosis to be made prior to angiography in some cases. 1
Angiography is desired to identify the location and define the precise vascular anatomy of the foregut and mid gut.3,4 The variability of arterial supply in this region makes angiography particularly important. 4 The use of angiography also can help to identify any other aneurysm (20% are multiple), delineate the feeding vessel, demonstrate any arterioportal fistula, and provide the anatomical information needed for surgery or embolization. 1
Treatment
Because of the high rate of spontaneous rupture, treatment of hepatic artery aneurysms greater than 2 cm in diameter is usually recommended. 5 The goal of treatment of extrahepatic aneurysms is to exclude or excise the aneurysm while preserving or restoring hepatic arterial blood flow. 4 Treatment is usually in the form of ligation and surgical correction for extrahepatic aneurysms and transcatheter embolization for intrahepatic aneurysms.1,2 Because of the extensive foregut collateral circulation to the liver through the gastroduodenal and right gastric arteries, adequate hepatic blood flow is usually maintained despite common hepatic artery interruption. 3 In addition, the portal vein supplies 70–75% of blood coming into the liver. This is usually sufficient to promote normal hepatic function in the event of hepatic artery occlusion. This dual blood supply makes hepatic infarction rare in the native liver. 6 However, if blood flow to the liver appears compromised, aneurysmorrhaphy or formal hepatic revascularization should be performed. 3 Non-surgical interventions such as embolization and stented graft insertion into the aneurysm sac have recently been applied in the treatment of visceral artery aneurysm. 5
Conclusion
Hepatic artery aneurysm is a rare finding and ultrasound is frequently a useful tool in detecting these lesions. The large aneurysm described created a challenging assessment of the anatomy and required other forms of evaluation to receive proper diagnosis and treatment.