
Abstract
Case Report
A 49-year-old athletic male presented with a 3-year history of unrelenting left lower-extremity edema after a motor vehicle accident. He underwent a venous duplex ultrasound, which revealed distal left superficial femoral and popliteal deep venous thrombosis and multiple venous collaterals with arterial Doppler signals within the thrombus and vein wall at the level of the popliteal fossa. Doppler waveforms were highly suspicious for an arteriovenous fistula (AVF). Direct auscultation of the popliteal fossa revealed a continuous bruit. Magnetic resonance arteriography revealed early venous filling of the left femoral vein with multiple dilated veins in the region of the popliteal artery, consistent with AVF. The patient underwent surgical interruption of the AVF with significant resolution of the lower extremity edema.
Conclusion
In our experience, unusual Doppler waveform characteristics and multiple collateral vessels should alert the sonographer to the possibility of an AVF. This report exemplifies the role of Doppler ultrasound in the diagnosis of unrelenting and unexplained lower extremity edema.
Introduction
Traumatic arteriovenous fistulae are common sequelae and often are associated with limb edema, exertional limb discomfort, and/or symptoms suggestive of high-output congestive heart failure. Most small arteriovenous fistulae are asymptomatic and may only be discovered when an astute clinician notes an audible continuous bruit on direct auscultation. In this era of percutaneous endovascular revascularization procedures, the most common scenario for the discovery of a traumatic arteriovenous fistula (AVF) is after a percutaneous intervention. High-resolution color duplex ultrasonography is the ideal examination to identify and characterize the elusive AVF, including the feeding artery and outflow vein. We present a case of a healthy man who sought medical attention because of chronic dependent edema of the left lower extremity remote from major pelvic trauma.
Case Report
A 49-year-old physically fit (marathoner) gentleman presented to the Massachusetts General Hospital Vascular Center in May of 2007 complaining of chronic left lower extremity-dependent edema. In October 2004, he was involved in a motor vehicle accident while riding his bicycle. He sustained significant orthopedic trauma to his pelvis, a left olecranon fracture, left acetabular fracture with dislocation, closed head injury, and fifth lumbar vertebrae bipedicle fracture. He underwent numerous reconstructive surgeries and after extensive rehabilitation during the course of several months, he was able to resume exercise. Since the reconstructive surgeries, he has noted left leg-dependent edema for which he wears a compression stocking. He noted persistent painless edema that was worse without stocking. He noted no change in his edema despite being able to run several miles during the past 3 years. He had no previous known history of deep vein thrombosis and did not undergo any surveillance venous duplex ultrasonography during his hospitalization or rehabilitation. He did receive pharmacoprophylaxis for deep venous thrombosis after his trauma. He has no known history of previous heart disease or stroke. Physical examination revealed a healthy, white male with only mild pitting edema in his left mid calf without involvement of the ankle, foot or toes. No varicose veins or stasis pigmentation changes were noted bilaterally. No tenderness on deep palpation of the left thigh, calf or popliteal fossa. Pedal pulses were palpable and symmetric. There was leg circumference discrepancy, with the left calf and ankle measurement 0.5 cm larger than the right. Neurological examination and gait were normal.
Diagnostic Evaluation
In May 2007, the patient underwent a duplex ultrasound evaluation, including a venous reflux study, with the HDI 5000 digital ultrasound system from Advanced Technology Laboratories Ultrasound (Bothell, WA). There was mild deep venous insufficiency involving the common femoral veins bilaterally with chronic deep venous thrombosis (DVT) in the distal left femoral vein and proximal popliteal vein. The veins were not dilated, and there were no collateral veins noted during that examination (Figure 1A and 1B). The thrombus was echogenic. Quantitative complete blood count, D-dimer assay, and hypercoagulable studies were all normal.
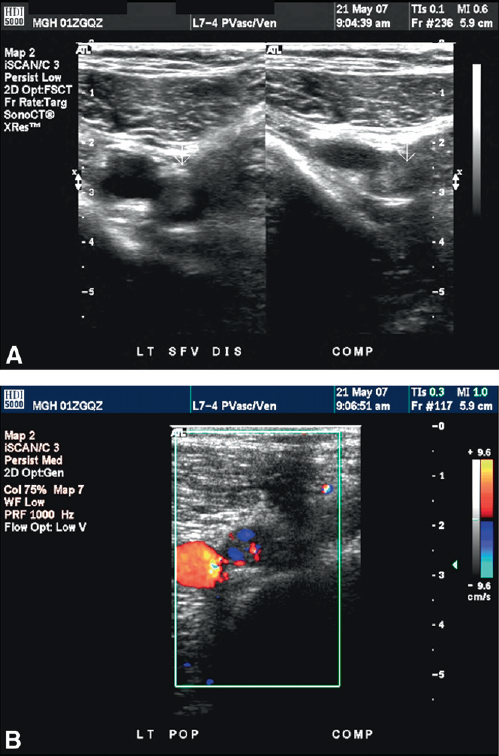
(A) Transverse duplex imaging of the distal left superficial femoral artery and superficial femoral vein with and without compression maneuver. Thrombus is seen in the vein. (B) Transverse color Doppler of the superficial femoral artery and vein showing organized thrombus and recanalization within the vein.
Despite recommendations to proceed with anticoagulation, the patient opted against this recommendation. The patient returned 9 days later for a repeat duplex ultrasound examination with Philips IU-22 duplex ultrasound scanner (Philips Medical, Bothell, WA). It demonstrated a persistent distal left femoral vein and popliteal vein DVT (Figure 2A). There was Doppler evidence of early recanalization in the popliteal vein along with what appeared to be a few collateral veins in the region of the distal superficial femoral vein, which were not noted on the previous exam (Figure 2B). The patient was treated with thigh high compression stockings and was scheduled for an office visit in 3 months with a repeat duplex ultrasound.
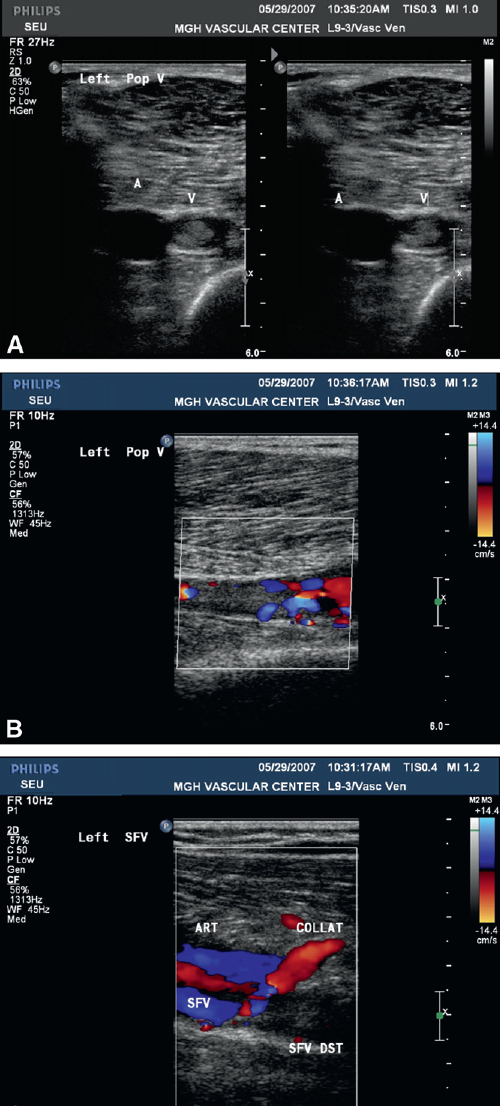
(A)Transverse duplex imaging of the distal left superficial femoral artery and superficial femoral vein with and without compression maneuver. (B) Longitudinal color Doppler of the superficial femoral artery and vein showing organized thrombus and recanalization within the vein and the vein wall. (C) Color Doppler of the extensive collateralization as a result of chronic venous obstruction (distal superficial femoral vein)
Persistent DVT was noted in the distal left superficial femoral vein and popliteal vein. Newly appreciated were multiple superficial venous collaterals with arterial Doppler signals in the region of the popliteal fossa within the thrombus and vein wall (Figure 2C). The Doppler waveform characteristics were highly suspicious of multiple arteriovenous malformations at the level of the distal superficial femoral vein and in the popliteal fossa. (Figure 3A and 3B). Interestingly, on direct auscultation of the popliteal fossa with a stethoscope, a continuous systolic/diastolic bruit was easily noted. Gadolinium-enhanced magnetic resonance arteriography revealed early venous filling of the left femoral vein and multiple dilated varicose veins that were in the region of the popliteal artery (Figure 4) consistent with a post-traumatic obscure AVF.
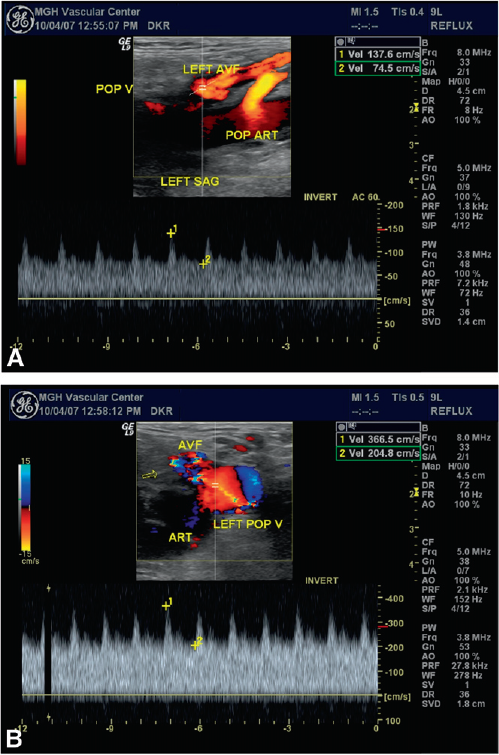
(A) Color power Doppler angiography showing the arteriovenous malformation between the distal superficial femoral artery and the distal superficial femoral vein. (B) Pulsed-wave Doppler showing the arterialization of the distal superficial femoral vein.

Magnetic resonance angiography demonstrating early venous phase in the distal superficial femoral vein.
Clinical Course
The patient was referred to vascular surgery for elective repair of this traumatic popliteal AVF. In December 2007, he underwent exploration of the left popliteal artery (retrogeniculate popliteal artery) with interruption of the traumatic AVF. As the result of significant scarring and possible trauma to the adjoining nerves, a conservative approach to exploration of the aneurysmal popliteal cavity was used. The completion arteriogram revealed a widely patent popliteal artery with a clinically insignificant communication between a small genicular branch draining into a small tributary of the main popliteal vein (Figure 5).

Postsurgical arteriogram demonstrating widely patent popliteal artery with a residual but clinically insignificant communication to the superficial femoral vein via the genicular tributary.
The patient recovered without complication. Three weeks later, he returned for follow-up and reported significant improvement. He had been wearing a compression stocking on his left leg and elevating the leg whenever possible. Trivial distal left calf edema was noted on examination with easily palpable pedal pulses.
In February 2008, the patient returned for a follow-up visit. The preoperatively noted low flow pulsatile bruit in the left popliteal fossa and distal left posterior thigh was no longer audible. Venous duplex ultrasonography showed persistent venous thrombosis of the distal left femoral vein and popliteal vein with recanalization of flow within the left popliteal DVT. There were no distal superficial femoral vein AVF present, but multiple small caliber but clinically insignificant arteriovenous communications were noted in the popliteal fossa consistent with the postoperative angiogram (Figure 6).
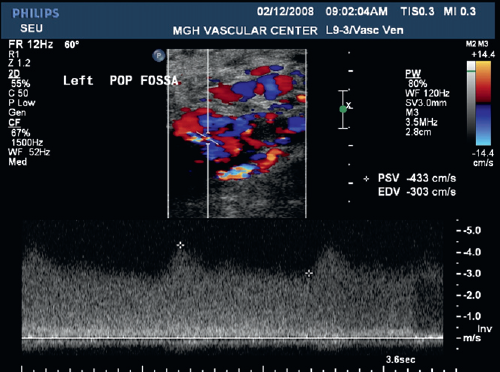
Postsurgical Doppler ultrasound demonstrating widely patent popliteal artery with a residual but clinically insignificant communication to the superficial femoral vein as demonstrated by an arterialized venous flow pattern.
Discussion
Duplex ultrasonography has been used for many years to evaluate lower-extremity edema. This case represents the most common indication (lower-extremity edema) for referral to the vascular diagnostic laboratory. Common findings include acute or remote deep vein thrombosis, venous valvular incompetence, varicose veins with associated superficial thrombophlebitis, and popliteal cysts. 1 The unique aspect of the latent presentation of AVF is not usually suspected and can be overlooked unless the technologist maintains a high index of suspicion.
It is important for the vascular technologist to use equipment and technique to uncover uncommon anatomic findings. 2 The unusual findings of multiple venous collaterals with arterial Doppler signals within the thrombus and vein wall in this case suggested an arteriovenous fistula. In one recent report, in which the authors had initially inspired the technologists and led to the diagnosis of this case, 3 the author described an interesting finding of arterial neovascularization within a venous thrombus (less than 1 year old) and vein wall of patients with proximal deep vein thrombosis, sometimes marked enough to appear as small AVF. In our case, subsequent ultrasound examinations revealed Doppler waveform characteristics that were suspicious for an AVF. The patient went on to have magnetic resonance arteriography, which confirmed the findings. 4
Conclusion
Our case demonstrates an unusual late manifestation of trauma and supports the strategy of serial venous duplex ultrasonography which, in this case, led to the diagnosis of traumatic arteriovenous fistula. 5 It is critical for the vascular technologist to posses thorough knowledge of normal and abnormal anatomy as the foundation for identifying unusual pathologies, and technologists must persist when an examination is not straightforward to confirm a diagnosis.