
Abstract
Background
The internal mammary artery (IMA) is the preferred conduit for coronary artery bypass grafting because of its improved long-term patency. Duplex IMA mapping may be requested as a component of preoperative assessment. We reviewed our institutional experience with IMA mapping procedures and determined expected values for IMA size and Doppler parameters.
Methods
Query was sent to the Cleveland Clinic Non-Invasive Vascular Laboratory database for all bilateral IMA mapping procedures performed from January 1, 2005 to June 30, 2007. Examinations were performed by the use of high-resolution B-mode and Doppler ultrasound. Mean values for IMA dimensions and Doppler parameters were determined along with reference ranges (mean ± 2 standard deviations).
Results
A total of 949 patients were identified. Mean age was 69.6 years, and 64.7% were men. Patients with significant subclavian stenosis were excluded from the primary analysis. Mean values and reference ranges for right and left IMA size and Doppler parameters are presented in tabular format. Bilateral IMAs were larger in men compared with women (p < 0.0001). The mean right IMA diameter was larger than left (p < 0.001). The presence of subclavian artery stenosis was associated with smaller vessel diameter and increased peak systolic velocity.
Conclusion
We report a range of expected values for preoperative IMA mapping procedures. These data may be used for development of laboratory diagnostic criteria or incorporated into future research on IMA duplex ultrasound for postoperative surveillance.
Introduction
The internal mammary artery (IMA), particularly the left IMA, is the preferred conduit for coronary artery bypass grafting (CABG) because of its excellent long-term patency and patient outcomes.1,2 Duplex IMA mapping may be requested for preoperative assessment. Previous studies have demonstrated the possibility of direct visualization of the IMA by the use of color duplex ultrasound in nearly all cases. 3 Duplex ultrasound has been demonstrated to be valid compared with angiography in preoperative assessment of the IMA. 4 Most of the current data regarding IMA diameter and velocity criteria are driven from studies that included a small number of patients either for preoperative IMA assessment or postoperative graft surveillance.4–9 Of note, these studies used different imaging modalities, including duplex ultrasound, echocardiography, intraoperative ultrasound, conventional angiography, and magnetic resonance imaging (MRI).4–9
Our vascular laboratory routinely performs IMA mapping procedures at the request of the cardiac surgical team. Currently there are no uniform criteria for IMA mapping that can be used to facilitate standardized evaluation. We reviewed our experience with IMA mapping procedures to determine an expected range of vessel diameter and velocity values.
Methods
Ultrasound Protocol
We performed a query of the Cleveland Clinic Non-Invasive Vascular Laboratory database for all bilateral IMA mapping performed January 1, 2005 to June 30, 2007. Examinations were performed by the use of high-resolution B-mode and Doppler ultrasound with a high-frequency linear array transducer and a standardized IMA mapping protocol. A parasternal and intercostal approach is used to identify the vessels (Figure 1). Spectral Doppler evaluation is performed at proximal, mid, and distal mammary artery segments in the longitudinal plane (Figure 2). Of note, mirror image artifact is a common finding in the IMA, and Doppler sampling must be performed with caution (Figure 3). 10 Anteroposterior diameter measurements of the mammary arteries are obtained in the longitudinal plane (Figure 4). Because of the small size of the IMA and the appearance of the surrounding tissues, accurate measurement is more successful in the longitudinal plane than the transverse plane. All measurements are entered into the database by the technologists at the conclusion of the study and reviewed and confirmed by the reading staff physician.

Technique for scanning the internal mammary artery from the parasternal anterior chest wall approach. The vessel is scanned in a longitudinal plane.
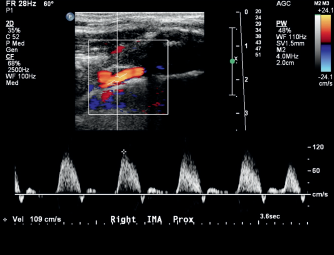
Pulsed Doppler waveform of the internal mammary artery demonstrating a normal triphasic pattern.
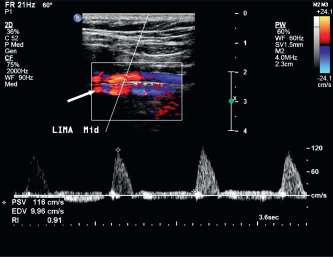
Color Doppler image of the IMA demonstrating mirror image artifact (arrow), a common finding in IMA mapping procedures. Mirror image artifact is caused by the presence of a strong reflector (in this case the sternum). The reflected image appears as an identical copy of the imaged structure. This second copy usually appears deeper to the true image. 10
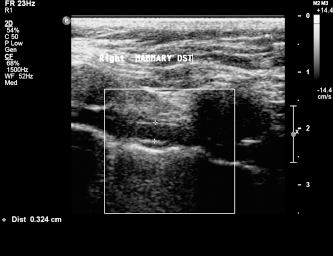
Grayscale image of the internal mammary artery demonstrating the technique for anterior-posterior diameter measurement.
Because of the potential for alterations in IMA size and flow with contralateral IMA harvest, we included only subjects with both IMA in place who had not yet undergone CABG with IMA conduit. 7 Similarly, because of the potential for hemodynamically significant subclavian stenosis to cause alterations in IMA flow (Figure 5), only patients who had a carotid artery duplex study within 30 days of the IMA mapping study were included in the study. Our carotid arterial duplex protocol routinely incorporates assessment of the bilateral proximal subclavian arteries and the innominate artery and is frequently performed on the same day as IMA mapping in preoperative patients. Patients with evidence of subclavian stenosis were excluded from the primary analysis of IMA diameter and Doppler parameters.
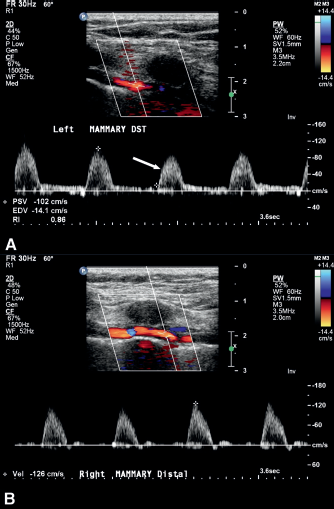
(A) Pulsed Doppler waveform of the left IMA demonstrating a delayed upstroke (arrow) in a patient with known left subclavian artery stenosis. The contralateral side with normal waveform is shown in (B).
Analysis
IMA diameter at proximal, mid, and distal vessel were analyzed, along with average IMA diameter (mean of the 3 measurements along the IMA length). The maximal peak systolic velocity (PSV) and end diastolic velocity (EDV) along the length of the IMA was used for analysis (i.e., greatest of the 3 measurements of proximal, mid, and distal vessel). For purposes of the primary analysis to define expected range of vessel size and Doppler parameters, patients with evidence of significant subclavian artery stenosis, as determined by the carotid duplex study, were excluded. Mean values (with standard deviation) for the IMA diameter and Doppler parameters and reference ranges (mean ± 2 standard deviations) were determined and presented in tabular format by gender and site (right vs. left). The effect of gender on vessel diameter and Doppler parameters was explored using the independent sample t test. The difference between size and Doppler parameters of the right versus left side was determined using the paired t test. All statistical analyses were performed by the use of the SPSS statistical software (SPSS Version 14. Chicago, IL).
Results
We identified 949 patients during the study period. The mean age was 69.6 years (range 36–93 years), and 64.7% were men. Thirty-nine patients with evidence of significant subclavian stenosis were excluded from the primary analysis of vessel size and Doppler parameters. The findings are summarized in Tables 1 and 2. For all patients, the right IMA mean diameter was 3.19 ± 0.56 mm; left IMA mean diameter was 3.11 ± 0.54 mm. The difference in mean diameter by site was statistically significant (p < 0.0001). Mean right PSV was 108.7 ± 28.6 cm/sec and left PSV was 106.3 ± 29.2 cm/ sec. The small difference in right versus left PSV achieved statistical significance (p = 0.003) and was attributable to the smaller diameter of the left IMA. There was no significant difference in EDV by site. Mean IMA diameter and velocity varied by gender. All IMA diameters were larger in men compared with women (p < 0.0001). The mean PSV was greater in women compared with men (p < 0.001), again attributable to smaller average diameter in women. The mean EDV was also slightly greater in women compared with men (p < 0.001).
IMA Diameter by Vessel Site and Patient Gender
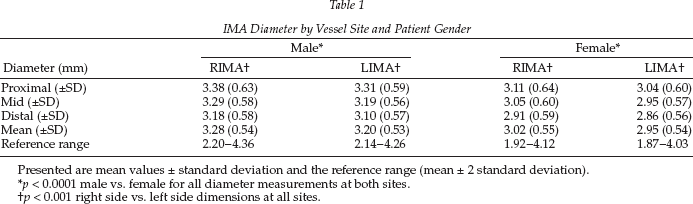
Presented are mean values ± standard deviation and the reference range (mean ± 2 standard deviation).
p < 0.0001 male vs. female for all diameter measurements at both sites.
p < 0.001 right side vs. left side dimensions at all sites.
IMA Velocity Parameters by Vessel Site and Patient Gender
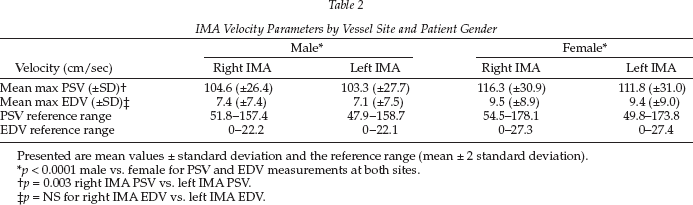
Presented are mean values ± standard deviation and the reference range (mean ± 2 standard deviation).
p < 0.0001 male vs. female for PSV and EDV measurements at both sites.
p = 0.003 right IMA PSV vs. left IMA PSV.
p = NS for right IMA EDV vs. left IMA EDV.
We studied the effects of subclavian stenosis on IMA vessel diameter and Doppler parameters. Among the 39 subjects with evidence of significant subclavian stenosis by duplex ultrasound, mean IMA diameter in both the left and right IMA was smaller than among the 910 patients without subclavian stenosis (right IMA 2.99 vs. 3.19, p = 0.027; left IMA 2.97 vs. 3.11, p = 0.10). Of note, this difference did not achieve statistical significance in the left IMA, likely as the result of the small sample size. In the patients with subclavian artery disease, the presence of subclavian artery stenosis was also associated with a difference in PSV (right IMA PSV 124.3 vs. 108.7, p = 0.001; left IMA PSV 114.8 cm/ sec vs. 106.3 cm/sec, p = 0.78). Again, this difference was caused by smaller IMA diameter associated with subclavian stenosis. A small difference in EDV did not achieve statistical significance.
The reference ranges for IMA dimension and velocities were determined and are reported in Tables 1 and 2 by vessel site and gender. With combining male and female patients (without subclavian stenosis) for purposes of simplified diagnostic criteria, proposed reference ranges for IMA parameters are as follows: right IMA diameter (2.08–4.30 mm), left IMA diameter (2.03–4.20 mm), right maximal PSV (51.4–165.9 cm/ sec), left maximal PSV (48.0–164.6 cm/sec). The reference range for maximum EDV for both the right and the left IMA was (0–24.2 cm/sec).
Discussion
IMA is the preferred conduit for CABG, with excellent early and long-term patency rates and favorable patient outcome compared with venous grafts.1,2,11–13 Studies have also shown that the survival benefit increases with time, suggesting that conduit selection is an important factor in that survival advantage.1,2,11–13 Because of the large number of CABG procedures performed annually and the importance of the IMA as a graft, there is a need for standardized preoperative IMA ultrasound evaluation. There may also be an emerging role for long-term postoperative ultrasound follow-up of IMA grafts as the result of prolonged life expectancy and the fact that angiographic long-term follow-up is expensive, invasive, and unwarranted in asymptomatic patients. 14
Recently, some investigators have reported on the use of Doppler ultrasound for postoperative IMA graft surveillance.7,8,15 These studies have shown consistent results comparing the preoperative and postoperative IMA flow patterns and velocities.7,15 The postoperative changes demonstrate a change in the Doppler flow pattern from a high to low resistance signal with decrease in PSV and increase in EDV. It has been proposed that these findings could be used to develop standardized methodology for long-term postoperative follow-up of IMA grafts with duplex ultrasound. 8
In our article, we define ranges of expected values for IMA diameter and velocity. Our data demonstrate a larger right than left IMA mean diameter and a gender difference in diameter and velocity parameters. The differences in velocities were driven by the smaller IMA diameters in women. We confirmed our hypothesis that the presence of subclavian artery stenosis would be associated with changes in IMA size (small diameter) and flow (increased PSV).
Our study was designed for the purpose of proposing preoperative IMA diameter and velocity criteria to provide more objective data regarding IMA quality as a graft. These data can be used to standardize preoperative IMA assessment protocols and may also be of use in the development of techniques for postoperative IMA follow up.
To our knowledge, our study is the largest of its kind in providing significant data regarding expected diameter and velocity parameters for the IMA. The primary limitations of our study are the lack of a normal healthy control group and the absence of angiographic correlation. Although this deficiency could be addressed in subsequent studies evaluating healthy volunteers and reviewing angiographic correlations, we feel such projects are likely to be of little value as the native IMA is rarely affected by atherosclerosis, and healthy young volunteers, by definition, rarely need CABG. We have attempted to control for the effect of atherosclerotic vascular disease by eliminating patients with subclavian stenosis from the primary diameter and Doppler analysis. The fact that our results are based on a single institution experience may also limit the ability to generalize our findings.
Conclusion
Duplex ultrasound is a reliable diagnostic tool with an outstanding safety profile that can be used for pre-operative mapping of the IMA to evaluate conduit before CABG. We report a range of expected values for preoperative IMA mapping procedures. These data may be used for development of laboratory diagnostic criteria or incorporated into future research on IMA duplex for postoperative graft surveillance.