
Abstract
Presented is a case series of duplex ultrasound examination for evaluation of the hypothenar ulnar artery. Because of its superficial location, the distal ulnar artery is well characterized by duplex ultrasound. Aneurysm, thrombosis, and ectasia are the most common abnormal findings. The study is a single-center database query of all arterial duplex examinations performed from January 1, 2000 through December 31, 2006, and containing the words ulnar artery. A total of 2766 upper-extremity arterial duplex scans were queried yielding 155 scans meeting the search criteria. A total of 9 ulnar arteries were interrogated into the hypothenar area of the hand. Seven of them were abnormal, and 2 were follow-up studies of a patient who had undergone repair of bilateral ulnar artery aneurysms. Reported symptoms include pain, digital lesions, pallor or a pulsatile mass. Of the 7 abnormal ulnar arteries, 3 arteries were aneurysmal (diameter greater than 1.5 times the proximal segment), and 3 were ectatic (increase in diameter less than 1.5 times the proximal segment). Two arteries were tortuous, and one was occluded. All but one patient was a past or present smoker. All abnormalities were attributed to occupational repetitive trauma and one patient experienced a single traumatic event. The mean patient age was 42 years (median 37) and all were male. Of the 3 aneurysms, the largest was 17 mm and was associated with mural thrombus and a biphasic Doppler signal. The other 2 aneurysms were 5.0 and 6.9 mm with mural thrombus and triphasic Doppler signals. One patient underwent successful thrombolysis, 3 patients were followed conservatively, and 2 of the aneurysms and one of the thrombosed arteries were surgically repaired. Although abnormal findings of the distal ulnar artery are rare, they may be well visualized and characterized with duplex ultrasound. Duplex ultrasound is an ideal diagnostic modality for evaluation and follow-up of distal ulnar artery abnormalities in experienced vascular laboratories.
Introduction
Abnormal ultrasound findings of the ulnar artery are rare and almost exclusively reported in association with trauma. Aneurysmal dilation and thrombosis are the most common abnormal findings. Ulnar artery aneurysms usually are true aneurysms and are associated most often with occupational trauma, as in the hypothenar hammer syndrome. 1 Rarely described causes of ulnar artery aneurysm include atherosclerosis, HIV, congenital, and vasculitis-associated aneurysms.2–5
Diagnosis of ulnar artery abnormalities begins by obtaining and performing a detailed history and physical examination. History of either a single traumatic event or repetitive trauma to the hypothenar area of the hand is suggestive of the diagnosis. Patients may present with complaints of hand or digit pain, digital lesions, a pulsatile mass in the hypothenar region of the hand, or with a history of Raynaud phenomenon. The Allen's test, first described by Edgar V. Allen in 1929, may be performed to assess for patency of the ulnar artery. 6 This test is performed by having the patient make a fist while the technologist applies pressure over the radial and ulnar arteries to occlude them at the wrist. After the patient opens his or her hand, pressure over the ulnar artery is released and color is expected to return to the hand within seven seconds.
Patency of the radial artery may be assessed in a similar fashion and is called the reverse Allen's test for comparison. Noninvasive vascular laboratory testing, including pulse volume recordings and duplex ultrasound, can confirm the diagnosis and assist with characterization of the anatomy for planning the appropriate treatment. Arterial duplex ultrasound is an ideal diagnostic modality to assess the ulnar artery, given its superficial location in the palm and because it is quick, accurate and noninvasive. 7 Therapeutic options may vary depending on the precise location and nature of the abnormalities identified. Small aneurysms can be resected followed by end-to-end anastamosis. Vein patch, ligation, and interposition vein grafts have all been described.8,9 Thrombolytic therapy may be used when thrombosis of the artery is encountered and medical therapy with vasodilators is used to treat pain secondary to vasospasm.10,11
Methods
The present study is a single-center vascular laboratory database query identifying all reports containing the words ulnar artery from January 1, 2000 through January 15, 2007. A total of 2766 upper-extremity arterial duplex scans were queried, yielding 155 scans meeting the search criteria. The ultrasound reports of all 155 scans were personally reviewed. A total of 8 arteries were identified in which the ulnar artery was interrogated into the hypothenar area demonstrating aneurysm, tortuosity or thrombosis of the vessel. Images stored on the MagicView picture archiving and communication system (PACS) were reviewed. Data were collected directly from the images and from the patient's electronic medical record was recorded onto data collection sheets for each abnormal artery. All abnormalities were characterized with regard to affected side, vessel size, and presence of thrombosis, spectral Doppler analysis and velocities. Additional data collected included age, gender, occupation, suspected etiology, smoking status, pertinent medical history, symptoms, and therapeutic intervention used. All ultrasound scans were performed using either an Advanced Technologies Laboratory (ATL) 5000 (Bothell, WA) or a Phillips IU22 (Bothell, WA) ultrasound system.
Results
Of 155 ulnar artery duplex scans performed, 9 were scanned into the hand. Seven of these studies were performed as the result of pain, presence of a pulsatile mass, or as the result of symptoms involving the contralateral hand. Two arteries were evaluated as follow-up in a patient who had undergone surgical repair of bilateral ulnar artery aneurysms prior to the start of our query. Table 1 lists demographic and historical data pertaining to each case. Aneurysmal dilation, defined as 1.5 times the proximal segment, or ectasia, defined as enlargement of the vessel <1.5 times the proximal segment, was identified in 6 arteries. Two arteries were tortuous, and one was thrombosed.
Historical Data Table
Note: all subjects were men.
Aneurysm of the right and left ulnar artery was documented on duplex in 1999, before the start of our query. The present study was performed as a follow-up. His symptoms of numbness were resolved, and the artery appeared normal, without even postoperative changes visible.
HPL = hyperlipidemia, CCB = calcium channel blocker, R = right, L = left, N/A = not applicable.
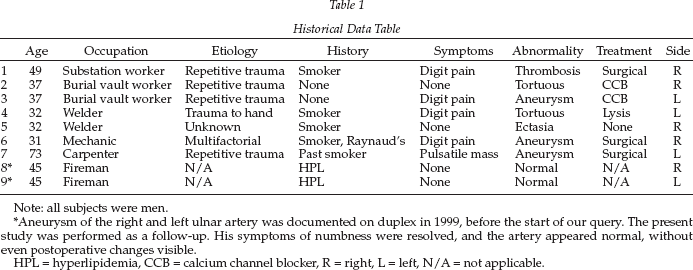
A tortuous or redundant hypothenar ulnar artery is illustrated using grayscale and color Doppler in Figure 1A and B. Figure 2 is an example of a partially thrombosed vessel with a kink noted, consistent with the patients reported history of striking his hand on a ceiling fan blade. All patients presented as the result of pain except for one, who presented because of an enlarging pulsatile mass. Four of seven were smokers, and one was a past smoker. All abnormalities were associated with an occupational history of repetitive trauma except for one, which was associated with a single traumatic event to the hand. Figure 3 illustrates a totally occluded right hypothenar ulnar artery in a patient with a reported history of using his right palm to pound pad locks as part of his work for 15 years. The mean age was 42 (median 37) and ranged from 31 to 73 years. All subjects were men.
(A) Longitudinal grayscale image of the left hypothenar ulnar artery. (B) Longitudinal color Doppler image of the right hypothenar ulnar artery in the same patient. In (A), grayscale imaging is used to enhance visualization of the vessel walls revealing the tortuous nature of the artery. (B) demonstrates corkscrew redundancy of the artery in the opposing hand. This patient reported a history of working with vibratory tools and presented with a cold blue left hand and painful digits.
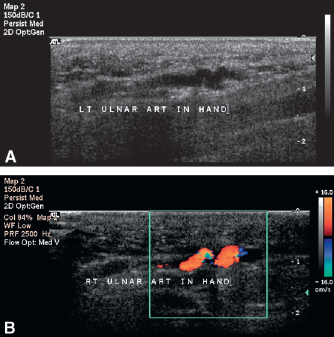
Shown is a longitudinal color Doppler image of the left hypothenar ulnar artery demonstrating a small kink in the artery, turbulent flow with color aliasing, and lack of color filling proximally, suggestive of partial thrombosis. This male patient reported hitting his left hand against a ceiling fan blade and presented with acute onset of cyanotic and painful digits.
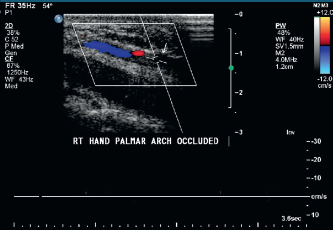
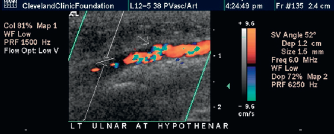
Shown is a longitudinal color and pulsed-wave Doppler image demonstrating occlusion in the right ulnar artery palmar arch evidenced by lack of color filling and absence of a Doppler spectral waveform. This patient presented with the sudden onset of right hand and digit pain and discoloration. He reported a 15-year history of working at electrical substations pounding pad locks with his right palm.
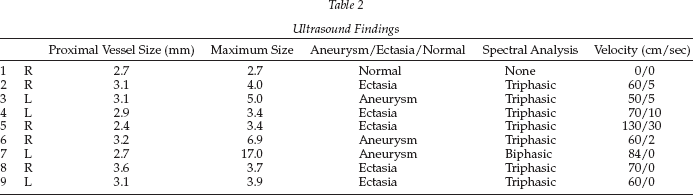
Of the 3 aneurysms, the largest was 16.8 mm, associated with mural thrombus and a biphasic Doppler signal. Figure 4 is a measurement of a normal appearing distal ulnar artery. Figure 5 illustrates the same vessel at the level of the hypothenar eminence of the hand. The artery is dilated to a maximum dimension of 16.8 mm in transverse compared with the normal segment of the artery that measured just 2.7 mm. The length of the defect was 3.6 cm (Figure 6A) and appeared to contain mural thrombus. Color Doppler illustrated a swirling pattern of flow (Figure 6B). The spectral Doppler waveform of the normal vessel is illustrated in Figure 7A. Note the typical high resistive, triphasic pattern expected in a muscular branch artery. Figure 7, panel B illustrates the spectral Doppler waveform of the same artery with the aneurysmal segment. Loss of the flow reversal component of the signal and filling in of the acoustic window is observed. The other two aneurysms were 5.0 and 6.9 mm with mural thrombus and triphasic Doppler signals. Additional ultrasound findings of each case are detailed in Table 2.
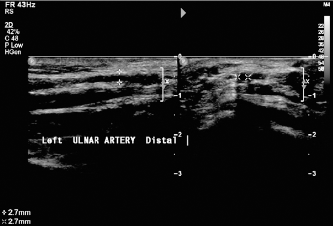
Shown is a split screen grayscale image of the left ulnar artery at the wrist just proximal to the hypothenar eminence. On the left is a longitudinal view with an anterioposterior measurement of 0.27 cm. On the right is a transverse view with width measurement of 0.27 cm.
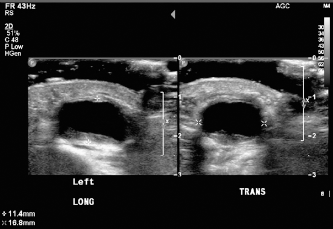
Shown is a split-screen grayscale image of a dilated segment of the left ulnar artery at the level of the hypothenar eminence. This is the same artery as shown in Figure 4. On the left is a longitudinal view with an anterioposterior measurement of 1.14 cm and on the right is a transverse view with a width measurement of 1.68 cm.
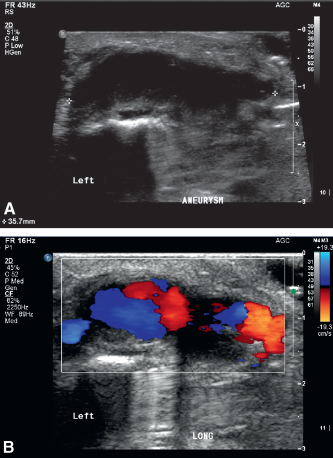
(A) Shown is a longitudinal grayscale image of the left hypothenar ulnar artery illustrating aneurysmal dilation and measuring 3.6 cm in length. (B) Shown is a longitudinal color Doppler image of the same segment of vessel as in (A). Color Doppler illustrates more clearly the irregularity of the vessel walls and the loss of laminar flow replaced by a swirling pattern within the aneurysm.
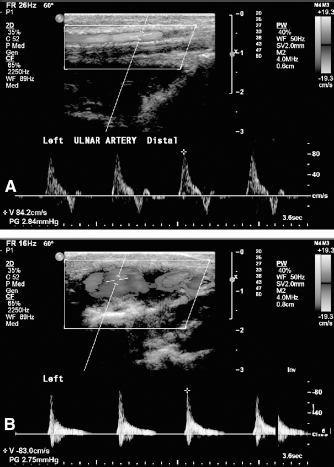
(A) Shown is a longitudinal image with a normal segment of the distal ulnar artery with a typical triphasic high resistive Doppler signal with an open acoustic window. (B) Shown is a segment of the same vessel within the hypothenar eminence of the hand. Note the loss of the flow reversal component of the triphasic signal and filling in of the acoustic window.
Ultrasound Findings
Three arteries were treated with conservative medical therapy consisting of calcium channel blocker (vasodilator) therapy or observation. The artery, which had thrombosed as the result of a single traumatic event, underwent successful thrombolysis without the need for surgical intervention. The remaining 3 arteries underwent surgical repair. One underwent palmar arch bypass, another underwent resection with vein grafting and one underwent resection with end-to-end anastamosis.
Discussion
Evaluation of the ulnar artery into the hypothenar eminence with ultrasound is rarely performed. The present study illustrates the usefulness of ultrasound with regard to identifying the artery and investigating and characterizing abnormalities. Ultrasound was able to identify several specific abnormalities including ectasia, tortuosity, aneurysm, and thrombosis. Flow can be assessed to identify total occlusion of a vessel versus partial thrombosis. The noninvasive nature, ease of use, and accessibility of the vessel lends itself well to short interval follow up during treatment in the case of Thrombolytic therapy and for long term surveillance after surgical as well as conservative treatment options.
When performing these unusual studies, it is important for the sonographer to choose the appropriate ultrasound transducer and perform a study that provides information pertaining to change in vessel size, tortuosity, presence of thrombus or intimal damage, and spectral Doppler information including the presence or absence of flow. Images should be obtained using both color and grayscale modes. Color is helpful to identify direction of flow and absence of color filling in the case of partial or complete thrombosis. When an occlusion is identified color power angiography should be used to rule out minimal flow that may not be seen with standard color Doppler. Grayscale imaging helps to identify vessel wall abnormalities and allows for better characterization of thrombus when present. It is important to ensure proper measurements are obtained at the proximal normal segment of the vessel in both the transverse and anterior-posterior views. We considered the vessel at the level of the wrist, or just proximal to any pathology identified as the normal segment of the artery. Calipers should be placed on the outer walls of the vessel to provide the most accurate measurement. The vessel should taper to a smaller size as it is viewed more distally. It should be noted if it becomes larger as this may indicate an ectatic vessel. If it enlarges to more than 1.5 times the proximal segment then it should be identified as aneurysmal.
In the current series, linear 8–4 MHz, linear 7–4 MHz, and linear 12–5 MHz transducers were used to interrogate the ulnar artery. The greater frequency transducer was used to achieve the highest image quality for evaluating superficial structures. This allows for detailed images of the intima, intraluminal echogenic material and for clear visualization of the adventitia for proper measurements.
Although symptoms may be present on just one side, the contralateral side was often evaluated to serve as a baseline reference. Interestingly, disease was often discovered in the contralateral asymptomatic side (four of the six patients presented). For this reason, we suggest interrogating both ulnar arteries especially if occupational repetitive trauma is suspected to be the etiology.
Conclusion
Abnormal findings of the distal palmar ulnar artery are rare and are well visualized and characterized with duplex ultrasound because of its superficial location. The most common abnormalities are aneurysm, ectasia, tortuosity and thrombosis. These findings are most often seen in men as a result of either occupational repetitive trauma or less commonly after a single traumatic event. Although the age range varies from the early 30's to the seventh decade, most patients are in their late 30s or 40s. The presence of painful digits is the most common reason for referral. In some cases, scanning the asymptomatic contralateral artery will uncover similar abnormalities. Duplex ultrasound is an ideal diagnostic modality for the initial evaluation and for follow-up of abnormalities involving the distal ulnar artery.