
Abstract
Waveform analysis is inherent to nearly every procedure performed in the vascular laboratory, yet waveform terminology and definitions have not been standardized. A review of waveform literature notes that three terms have been used to classify Doppler waveforms in the peripheral arterial circulation—triphasic, biphasic, and monophasic. These terms, however, are briefly detailed, often contradictory, are substituted by alternative terminology and also used for classifying waveforms generated by plethysmographic devices. Because sonographers are the primary party in waveform classification, failing to address this issue will be most keenly felt in the future. In the advent of vascular ultrasound sonographers received an average of three years on-the-job training; today career option is no longer available and formal ultrasound education is mandatory. Furthermore, physicians and ancillary medical personnel are integrating ultrasound into their practices. A lack of waveform standards has the potential to stimulate inappropriate testing and is hindering the advancement of the vascular ultrasound profession.
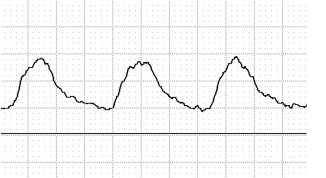
Imagine that you are a vascular sonographer who has worked for several employers. Currently, you are the lead sonographer at a small regional hospital and you are having a telephone conversation with a vascular surgeon concerning his patient's arterial physiological evaluation. You have informed the surgeon that his patient has multiphasic, continuous-wave (CW) Doppler waveforms in the common femoral artery, bilaterally, before treadmill exercise that became monophasic immediately after exercise (Figure 1A and B).

(A) Pretreadmill exercise, multiphasic triphasic common femoral artery, CW Doppler waveform with systolic forward flow, early diastolic flow reversal, and late diastolic forward flow. (B) Post-treadmill exercise, multiphasic, low-resistive common femoral artery, CW Doppler waveform following with pandiastolic forward flow above the zero-flow baseline.
The referring vascular physician sounds anything but happy with your waveform characterization impression and wants to know why you would describe blatantly triphasic waveforms as monophasic after exercise. “In our institution,” you reply, “our waveform classification protocol dictates that Doppler signals from peripheral arteries with diastolic flow reversal are to be referred to as multiphasic and waveforms without flow reversal are to be characterized as monophasic.”
“Are you telling me,” the vascular surgeon responds, incredulously, “my patient has an aortoiliac obstruction?”
“Sir, I'm not trying to diagnose anything,” you reply, trying to sound calmer than you feel.
You attempt to be diplomatic by explaining that although your institution has chosen to describe waveforms as multiphasic or monophasic, you have worked for other physicians that define the postexercise waveform as biphasic (Figure 1B) and use tardus parvus (Figure 2) to characterize waveforms found distal to a significant arterial obstruction.
Tardus parvus, low resistive, monophasic CW Doppler waveform with prolonged systolic upstroke, pandiastolic forward flow without diastolic flow reversal.
“What self-respecting vascular laboratory would describe waveforms distal to an arterial obstruction as tardus parvus?” screams the surgeon.
You bite your lip and swallow your pride, answering in a low professional tone. “A well- respected cardiologist I previously worked for described obstructive waveforms in this very manner.”
The vascular surgeon's expletive cannot be printed in this article, but his tirade ends with the following questions: “Are you even certified? What sort of drivel did they teach you in school?”
“Sir,” you reply curtly, “I am a registered vascular sonographer with a bachelor's degree from a nationally recognized vascular sonography program. I was taught that peripheral arterial waveforms with early diastolic flow reversal and late diastolic forward flow are defined as triphasic, and waveforms without the third, smaller forward flow component are to be characterized as biphasic (Figure 3). Furthermore, luminaries in my profession have taught me that waveforms similar to those found in your patient before exercise can be labeled triphasic or biphasic, depending on their audio signature, and are found in normal patients with a nonhemodynamically significant obstruction proximal to the point or in diseased patients with a significant obstruction distal to the point of Doppler insonation. 1 ”
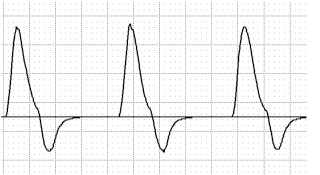
High resistive, biphasic CW Doppler waveform with systolic forward flow and early diastolic flow reversal below the zero flow baseline.
“And,” you add, your voice climbing two octaves, “current literature now suggests that we refer to these low-resistive biphasic waveforms as ‘atypical’.”
“You're insane!” are the last words you hear before the dial tone.
Although this scenario is both exaggerated and unlikely, it should not be considered unbelievable. Ironically, although waveform analysis is inherent to nearly every procedure we perform in the vascular laboratory, how we define and use this information is anything but universal. The fact of the matter is the characterization of peripheral arterial Doppler waveforms is heavily dependent on who you believe and whose work you reference.
In an historical review of major waveform research publications, book chapters and Doppler equipment manuals it was shown that three terms have been used to classify CW and pulsed-wave Doppler waveforms in the peripheral arterial circulation—triphasic, biphasic, and monophasic. These terms, however, are rarely discussed in great detail, and often vague or contradictory descriptors of waveform morphology are used. 2
In 94 educational and scientific publications reviewed between 1967 and 2006, nearly 10% failed to define any of these three terms. Triphasic was directly defined in 69%, monophasic in 59%, but only 36% of these publications defined the biphasic descriptor. Although 47% of the periodicals reviewed associated waveforms with pandiastolic forward flow as monophasic, half ignored the issue of pandiastolic flow altogether, and one author portrayed waveforms with this characteristic as both monophasic and biphasic. 3
This review also noted that multiphasic was a common substitute for triphasic, that biphasic could be depicted with and without diastolic flow reversal, and that tardus parvus was a substitute for monophasic and used to characterize waveforms with a significant arterial obstruction proximal to the point of Doppler interrogation. To complicate these issues further, biphasic was used to characterize both normal and abnormal waveforms, which may in part explain why the majority of the publications reviewed in this study omitted or ignored this descriptor. Finally, although these three terms were originally developed for use with Doppler devices, they have also been used to classify plethysmographic waveforms.
How has such confusion and contradiction gone unchecked for so long? That's a very good question, but a question that does not have a very clear answer.
In my opinion, there are a number of possibilities. First, as noted in preceding articles in this issue, these terms were originally developed for audio, nondirectional Doppler devices, yet bidirectional devices and the zero-crossing recorder quickly followed strictly audio technology. The audio component was supplanted and became secondary to the visual component. As waveform graphics became the primary interpretive focus, the original audio descriptors were never standardized to reflect these changes. Experts began to use these three descriptors indiscriminately and modified them to fit their belief. Research has reinforced earlier modifications and spawned new ones. Low-resistive “biphasic” waveforms were analyzed in the same statistical category as monophasic and “biphasic” became associated with diseased (abnormal) vessels. More recently, “biphasic” waveforms with diastolic flow reversal (normal) and “biphasic” low-resistive (abnormal) were analyzed separately. Analyzing biphasic, low resistive and monophasic waveforms as a single group and then separating biphasic into high- and low-resistive categories may explain why this waveform (Figure 1B) has been used to identify significant arterial disease above and below the point of Doppler insonation.
Failing to address waveform standardization could also be linked with the development and ever-increasing reliance on duplex imaging technology. The interpretive paradigm shifted once again—from audio to visual, to emphasizing velocity changes before and at the point of maximum stenosis. Duplex technology became our diagnostic instrument of choice, and physiological testing became secondary and largely ignored. Vascular laboratory testing guidelines issued as recently as 2006 by the American Society of Echocardiography and the Society of Vascular Medicine and Biology 4 omitted CW Doppler waveform analysis entirely. These guidelines emphasize velocity ratios, use biphasic to describe spectral waveforms without diastolic flow reversal, and replace monophasic with the term parvus et tardus. Ironically, with declining reimbursement, physiological testing devices, including CW Doppler, are experiencing a resurgence in use.
Am I over-Shakespearean and making much ado about nothing? After all, has a lack of waveforms standards had any clinical impact? Furthermore, if these issues have gone largely unnoticed and unaddressed for more than four decades, why should we be concerned about them now?
I believe we need to address these issues because sonographers, not physicians, are the primary responsible party in waveform characterization. Numerous research publications substantiate this argument, as well as a recent survey of more than 314 ultrasound professionals.
Sonographers scored significantly greater “correct” waveform characterization scores than physicians or students. 5 It must be noted, however, that additional research into this topic suggests that, depending on whom you reference, triphasic, biphasic and monophasic can be used interchangeably. Judging the “correctness” of waveform classification, or whether one individual is more correct than another, may be an impossible task.
Assuming, however, that my original premise is correct, and sonographers are indeed the primary responsible party for waveform characterization, our profession's lack of waveform standards may be most keenly felt in the future. In the early days of our profession, the average vascular sonographer had approximately 3 years of on-the-job training. Today, that option is not available for new American Registry of Diagnostic Medical Sonographers-registered vascular technologists. On-the-job training is now defined as a short course or workshop and the emphasis is on education and the degreed sonographer.
Finally, the American College of Physicians is advocating that ultrasound equipment be integrated into primary care offices throughout our country. 6 Furthermore, we are seeing more referrals to the vascular laboratory without a previous examination by a physician. 7 If biphasic can also mean monophasic, if triphasic defines low as well as high resistive waveforms, if physicians are relying on sonographers to characterize normal or abnormal blood flow, will the potential for inappropriate testing be more, or less, likely?
One of the pioneers of the Society for Vascular Ultrasound and lead educators of Doppler waveform analysis, Dr. Robert Barnes, stated that standardization was crucial to advancing the vascular ultrasound profession. Confusion regarding Doppler waveform characterization is a glaring example of our failure to confront and act on that challenge.