
Abstract
When screening seniors with a quick carotid scan (QCS) with ultrasound, one can discover the silent carotid artery disease (CAD) that is the leading cause of strokes and Medicare expenditures and allow preemptive management and stroke prevention. This is a discussion of the U.S. Preventive Services Task Force (USPSTF) recommendation against screening for CAD. The USPSTF recommended against screening the general population, but CAD and strokes occur predominantly in seniors. An incidence of 1% for 60% to 99% stenosing CAD in seniors was used, but the yield from 22,496 scans reported by the Society for Vascular Ultrasound was 7.5%. A 1% yield requires screening 1500 seniors to prevent 1 stroke, whereas a 7.5% yield requires only 200 scans. This disparity alone invalidates the USPSTF recommendation. Contrary to reports from the NIH, the USPSTF stated that CAD causes few strokes. The QCS was reported as not accurate, but the sensitivity was 93% in our laboratory and 97% at New York University. Risks incurred from screening were given as follow-up with angiography, which is now seldom used, and the risk of surgery, which was overstated. The USPSTF recommendation against screening for CAD, like those for reducing screening for breast and cervical cancer, is ill advised and should be reconsidered.
Introduction
Reducing health care expenditures is an important goal of health care reform. However, there has been concern that reducing or holding back certain expenditures could adversely affect care and increase rather that decrease the overall cost of some conditions. One such concern is that the recommendation of the U.S. Preventative Services Task Force (USPSTF) in 2007 against screening for carotid artery disease 1 would not only result in not preventing strokes but also thereby not reduce expenditures for strokes. This is similar to the concern regarding the recent USPSTF recommendation limiting mammograms 2 and that of the American College of Obstetrics and Gynecology (ACOG) limiting Pap smears. 3
Strokes are the third-leading cause of death and the leading cause of disability in the United States. There are more than 700,000 strokes annually, with 112,500 deaths and more than 262,500 cases with disability of a severity that requires long term institutionalization. 4 Because the care in nursing homes for these patients is expensive and averages 5 years, stroke is the leading line item expenditure for Medicare and amounts to more than 60 billion dollars annually. 5
Carotid artery disease (CAD) is the leading primary immediate cause of strokes and 80% of patients are asymptomatic before having a stroke. 6 However, it can be easily discovered by a simple, accurate, and inexpensive 5 minute image only ultrasound quick carotid scan (QCS).7,8 Once discovered, the CAD can be safely and effectively managed and potential strokes prevented. 9
The reasons put forth by the USPSTF for the recommendation against screening for CAD do not appear to be in concert with current evidence and have been questioned by spokespersons for the Society of Vascular Surgery (SVS). This is a presentation of the reasons put forth by the USPSTF in support of their recommendation against screening for CAD and a presentation of the evidence questioning the validity of those reasons. This is followed by a separate presentation of the evidence that screening seniors for CAD can result in both stroke prevention and cost reduction.
Presentation and Discussion of the U.S. Preventive Services Task Force Recommendation against Screening for Carotid Artery Disease
The reasons put forth by the USPSTF for their recommendation against screening for CAD 1 are presented below in italics with discussion of the evidence for or against those reasons following.
The USPSTF recommended against screening for CAD in the general population. CAD and strokes are uncommon in the general population but occur in seniors with logarithmic progression starting at age 60. 5 The question under consideration is not whether to screen the general population for CAD but whether to screen seniors for CAD.
The USPSTF used a 1% incidence of CAD for 60–99% stenosis in seniors for all calculations and estimates. But the yield from screening 22,496 seniors for 60–99% CAD by the SVS, Kaweah Delta District Hospital in Central California, New York University, and Madigan Army Medical Center was similar and averaged 7.5% (Table 1). 10 This error in the percent yield from screening and hence incidence of CAD used by the USPSTF for their calculations by itself invalidates their conclusions and recommendation. As will be shown subsequently, the 1% yield used by the USPSTF requires screening 1500 seniors to prevent one stroke, whereas the 7.5% yield found by the SVS, New York University, Kaweah Delta District Hospital, and Madigan Army Medical Center requires screening only 200 seniors to prevent one stroke.
Yield of CAD on Screening
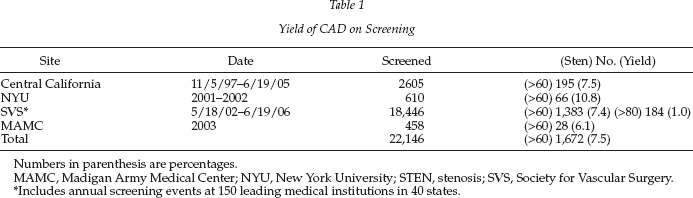
Numbers in parenthesis are percentages.
MAMC, Madigan Army Medical Center; NYU, New York University; STEN, stenosis; SVS, Society for Vascular Surgery.
Includes annual screening events at 150 leading medical institutions in 40 states.
The USPSTF stated that CAD causes few strokes. However, the National Institute of Health reported CAD as a dominant cause of strokes. 5 With a 7.5% incidence, 3 million of the 40 million senior Medicare recipients would have 60–99% carotid stenosis. At least two-thirds, or 2 million of these, would then be confirmed by follow-up studies. The stroke rate in the Asymptomatic Carotid Artery Stenosis study (ACAS)11,12 and in the more recent Asymptomnatic Carotid Surgery Trial study (ACST) 13 for 60–99% carotid stenosis with the best medical management at the time of the study was 11%, which would indicate that there is an at least 11% stroke rate for that degree of CAD without discovery or treatment. An 11% stroke rate in the 2 million seniors with confirmed 60–99% carotid stenosis would indicate that there are approximately 220,000 strokes annually as the result of CAD. This is 31% of the total of 700,000 strokes annually and is within the commonly held estimate that CAD causes 30–50% of strokes. Although this evidence-based estimate may not be exact, it is certainly in the right ball park and indicates that CAD is a major if not leading cause of strokes.
The USPSTF stated that the QCS was not accurate. However, the sensitivity of the QCS was 93% in our laboratory and 97% at New York University. 14
The USPSTF opined that carotid screening led to danger from the risk of conventional angiograms (CA) used to follow up those with positive screening scans and from the risk of unnecessary surgery resulting from false positive screening scans. However, initial follow-up of those with positive screening scans is accomplished with a full carotid artery ultrasound examination. This examination alone provides a full diagnosis in our experience in approximately 80% of cases. If additional examination is required, computed tomography or magnetic resonance angiography is generally all that is necessary, and a CA is used infrequently. The specificity of the QCS in our laboratory was 87% and at New York University was 93%, indicating that false-positive screening examinations are infrequent. Furthermore, they are readily corrected by the follow-up full carotid duplex examination and do not lead to unnecessary and potentially dangerous surgery.
Finally, the USPSTF stated that the stroke rate from carotid endarterectomy (CEA) was 3% at centers of excellence but greater generally at other sites and that this negated the value of screening. However, CEA is generally available with a perioperative stroke rate well less than 3%, and is quite widely so at 1% or less as reported by Cronenwett. 15 Matsen reported on 23,237 consecutive CEAs performed in Maryland with a 10-year stroke rate of 0.73% and of 51,331 in California with a stroke rate of 0.54%. 16 The authors’ 10-year stroke rate with CEA was 0.7%. Furthermore, by discovering silent stroke potential CAD, screening provides the opportunity to manage the disease with whatever is the best means available, whether it be surgery, stenting or medical management surely better than having the disease go unrecognized and untreated.
Presentation of Evidence that Screening for CAD Can Result in Stroke Prevention and Cost Reduction
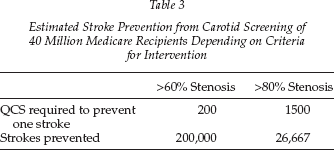
Stroke Prevention Evidence does indicate that screening seniors for CAD will prevent strokes. Table 2 shows the derivation of the number of quick carotid scans required to prevent one stroke on the basis of available data. From ACAS,11,12 we know that 11% of seniors with 60–99% CAD had strokes over a projected 5-year period even with the best medical management at the time of the study. It follows, therefore, that with no management at least 11% of seniors with 60–99% stenosis would have a stroke and that, subtracting perioperative risk, it would require 10 safely performed CEAs on such patients to prevent one stroke. It has been our experience that approximately two-thirds of the patients who are positive on a QCS come to CEA after full evaluation. 10 Therefore, screening must yield 15 patients to provide the 10 patients required for surgery to prevent one stroke. As was shown in Table 1, a QCS of 22,146 seniors resulted in a rather uniform yield of 7.5% with 60–99% CAD and 1% with 80–99% stenosis. Thus, with a 7.5% incidence for 60–99% stenosis, it requires screening 200 seniors to yield the 15 to prevent one stroke, and with a 1% incidence for 80–99% stenosis it requires screening 1500 seniors to yield the 15 and prevent one stroke. From these data, as shown in Table 3, it can be estimated that screening 40 million senior Medicare recipients for 60–99% CAD would prevent 200,000 strokes, but screening for only 80–99% disease would only prevent 26,667 strokes. Although there is a greater risk of stroke in the more stenotic group, many more seniors have 60–79% stenosis and the majority of strokes come from that group.
Quick Carotid Scans Needed to Prevent one Stroke
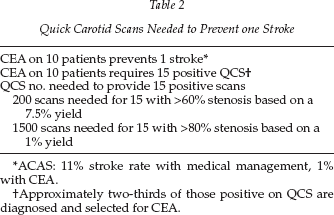
ACAS: 11% stroke rate with medical management, 1% with CEA.
Approximately two-thirds of those positive on QCS are diagnosed and selected for CEA.
Estimated Stroke Prevention from Carotid Screening of 40 Million Medicare Recipients Depending on Criteria for Intervention
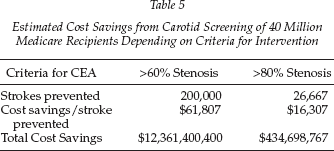
Cost Reduction Data do indicate that the stroke reduction effected by screening seniors for silent CAD would result in significant health care cost reduction.17–19 As shown in Table 4, the median direct medical costs of having a stroke is $147,000, and this is without including indirect costs such as lost productivity and family dislocation. 19 When one subtracts the cost of screening, evaluation of those positive on screening, and operative intervention from the direct cost of having a stroke, there is an overall saving of $61,807 in those with 60–99% stenosing CAD for every 200 seniors screened and for every stroke prevented. 10 Screening seniors only for 80–99% stenotic CAD, results in saving only $16,307 for every 1500 screened and for every stroke prevented. As shown in Table 5, when these cost savings are projected to the strokes preventable by screening 40 million senior Medicare recipients for 60–99% CAD, there is a potential saving of nearly 13 billion dollars.
Estimated Cost Savings from Carotid Screening and Prevention of One Stroke, Depending on Criteria for Intervention
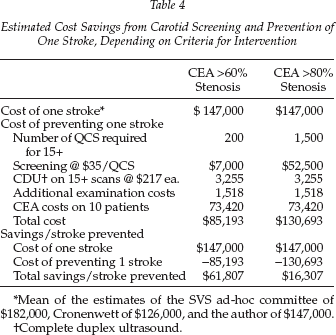
Mean of the estimates of the SVS ad-hoc committee of $182,000, Cronenwett of $126,000, and the author of $147,000.
Complete duplex ultrasound.
Estimated Cost Savings from Carotid Screening of 40 Million Medicare Recipients Depending on Criteria for Intervention
Discussion
Increasing emphasis is being given to the prevention of disease. At the same time, there is effort to reduce health care expenditures both for fiscal reasons and as one means of allowing the broadening of health care coverage. However, there is concern that some recent recommendations to reduce screening for prevention could be at least partially motivated by efforts to reduce health care expenditures and that this could not only adversely effect disease prevention but health care cost reduction as well. Examples of these recent recommendations are those of the USPSTF against screening for CAD and for reducing mammograms and that of the ACOG for reducing Pap smears.
Screening for Carotid Artery Disease
There is a perception among many clinicians, that with modern medical treatment, stroke incidence is declining and that proactive preventive measures are not necessary. However, strokes continue, with more than 700,000 occurring annually in the United States.
As we have shown, screening seniors for CAD can prevent strokes, our third-leading cause of death and the leading cause of disability, on an epidemiological scale and significantly reduce spending for strokes, the leading health care line item Medicare expenditure.
To effect primary stroke prevention now, it is imperative to find the silent CAD that is the immediate cause of the majority of strokes and manage it safely and effectively preemptively before the stroke occurs. Although reduction of secondary risk factors is important, compliance is uncertain and must be performed over many years to reduce the immediate causes of stroke and result in stroke prevention. To prevent strokes now and in the current generation of seniors, emphasis must be placed on finding and treating the immediate causes of strokes, the silent time bombs that seniors now carry and that can cause strokes at any time.
Many clinicians do not recommend screening and treating asymptomatic CAD. Because 80% of strokes occur without warning in asymptomatic patients, strokes can only be significantly reduced by finding and treating this asymptomatic disease prior to the stroke. It is also recommended by many that only CAD that produces >80% stenosis be treated. But as shown, the majority of strokes occur in patients with 60–79% stenosing disease and strokes can only be significantly reduced by managing all the stroke potential CAD, that is disease that is 60–99% stenosing, by the best means available.
The caveat is, of course, that the management must be done safely with an at least <3%, or better yet, 1% or less stroke rate. Whichever management modality is best should be used—surgery, stenting, or medical management. The deciding criteria in evaluating these treatment modalities should be which treatment has the lowest stroke rate. It is strokes that we are trying to reduce and avoid causing by treatment and strokes are the most important consideration. Of lesser concern are asymptomatic and questionable elevations in troponins or changes in the EKG, which are often lumped together with stroke rates in comparative evaluations of treatments.
Mammograms
During the same weeks in which health care reform dominated the news in the spring of 2010, the USPSTF recommended changing the starting age for screening mammograms for most women from age 40 to age 50 and doing them every other year rather than annually. 2 The reasons for the change were given as anxiety in some screened, unnecessary biopsies and surgery in those having false-positive screens, and fewer malignancies in the 40- to 50-year age group than those older. Cost reduction was not agreed to as a primary reason for the change.
The reasons for concern over this change are that breast cancer causes more than 40,000 deaths in the United States annually, and in women 40–50 years of age screening mammograms have reduced the mortality 15% and have saved 30 life years/1000. Although death caused by breast cancer is less common in those younger than 50, it is more profound because of life and family considerations.
The American Cancer Society (ACS) did not agree with the recommendation of the USPSTF to reduce screening mammograms. It is not clear whether Medicare and insurance coverage and reimbursement will be affected.
Papanicolaou “Pap” Smear
During that same period, ACOG announced a change in the recommendation for initiating the Papanicolaou “Pap” smears from a time 3 years after the onset of sexual activity in women to no earlier than age 21. 3 In addition, it was recommended that the frequency of the Pap smear be changed from annually to every 2 to 3 years depending on a number of factors. The reasons given for the change were the infrequency of cancer of the cervix in the age group 16–19 as well as the need for follow up laboratory examinations and operative procedures for false-positive smears. Once again, cost reduction was not agreed to as a major reason for the recommendation for change.
Before the Pap Smear, cancer of the cervix was the most deadly of all cancers for women. Since the advent of the Pap Smear in the mid-1900s with the support of the ACS, death from cancer of the cervix has been reduced more than 90% and is now rare. There is concern over this recent recommendation of ACOG, and the ACS did not concur in the recommendation.
Conclusions
The evidence put forth by the USPSTF against screening for carotid artery disease is flawed, and the recommendation should be reconsidered. The screening scan for carotid artery disease is rapid, simple, inexpensive, and accurate and can lead to preemptive management of the CAD, which is the leading cause of strokes and of health care expenditures. If the recent recommendations to reduce mammograms and Pap smears were determined by a similar flawed methodology, they should also be reconsidered. The proximity of the announcements regarding mammograms and Pap smears to the recent debate over health care reform and the attempts at expenditure reduction give concern over the part that fiscal considerations may have played in these decisions. The recommendation against carotid artery screening is particularly untenable in that the screening would not only prevent strokes but reduce health care expenditures as well. Furthermore, no additional invasive tests or surgery are needed for follow-up of those positive on screening for CAD such as is the case for mammography and Pap smears.