
Abstract
Introduction
Isolated aneurysms of the superficial femoral artery (SFA) are rare, and their etiology is not yet fully understood. Although not as common as abdominal aortic or popliteal artery aneurysms, they pose a serious threat of rupture and/or thrombosis. Because of their atypical presentation, they can be easily misdiagnosed.
Methods
A 58-year-old man presented with a painful lump over his left medial thigh, first noted 6 months previously. The patient was asymptomatic in regards to claudication. The findings of magnetic resonance imaging suggested a vascular mass versus pseudoaneurysm of the SFA. The patient was referred to the vascular laboratory and underwent duplex evaluation. This revealed an 8.3–cm long SFA aneurysm with a maximum diameter of 5.9 cm with extensive mural thrombus present. Angiography confirmed a true aneurysm, with an estimated length of 5 cm and luminal diameter of 2.5 cm.
Result
The patient underwent open aneurysmorrhaphy with a femoral to popliteal reverse saphenous vein bypass graft. Upon direct visualization, the aneurysm was estimated to measure 8 cm length and 6 cm in diameter. The patient recovered without incident and has normal ankle brachial indices.
Conclusion
True isolated aneurysms in the SFA are rare, and the exact cause is not yet known. Proper diagnosis and identification are crucial to patient outcome. In our case, duplex ultrasound yielded a more accurate measurement of the true aneurysm size when compared with the angiogram. This is attributable to the angiogram measuring the flow channel of the residual lumen while not visualizing the thrombus filled sac. Endovascular stent grafts or open repair with bypass grafts (vein or prosthetic) are the accepted methods of treatment with good patient outcome. Allowed to progress untreated, these aneurysms often rupture or thrombose, which can ultimately lead to limb loss. Because of the increased incidence of aneurysmal disease elsewhere in the body, these patients should undergo additional screening.
Introduction
An arterial aneurysm is defined as a dilation or bulge of the vessel wall. A true aneurysm involves the three layers of the arterial wall, the intima, media, and adventitia. False or “pseudo” aneurysms occur when the vessel wall is disrupted as the result of trauma or infection. In this case study we focus on a true aneurysm involving the superficial femoral artery (SFA). Isolated aneurysms of the SFA are rare, and their etiology is not yet fully understood. Although not as common as aneurysms of the abdominal aorta or popliteal artery, these aneurysms pose a serious risk to the patient. It is unclear whether they have more in common with abdominal aortic aneurysms and their threat of rupture, or with popliteal artery aneurysms and their tendency to embolize and thrombose. Because of their atypical presentation, they can be easily misdiagnosed.
Case Study
A 58-year-old man presented with an enlarging and sometimes painful lump over his left medial thigh, first noted 6 months previously. The patient did not use tobacco, had a history of hypertension and hypercholesterolemia, and a family history of hypertension and coronary artery disease. There was no family history of aneurysmal disease. The patient did not complain of claudication, and palpable pedal pulses were present. The findings of magnetic resonance imagining (MRI) suggested a vascular mass adjacent to the SFA versus pseudoaneurysm (Figure 1). The patient was referred to the outpatient vascular laboratory for duplex ultrasound to further delineate the mass. Ultrasound revealed an 8.3–cm long SFA aneurysm with a maximum diameter of 5.9 cm (Figure 2). Extensive intraluminal thrombus was noted with a patent flow channel (Figure 3). A 50–75% diameter reduction was identified at the proximal edge of the aneurysm. Ankle/brachial indices were within normal limits. A lower-extremity angiogram was performed that confirmed a true aneurysm, with an estimated length of 5 cm and diameter of 2.5 cm. (Figure 4). A 60% stenosis was identified at the origin of the aneurysm with two-vessel runoff to the foot. After surgical consultation, the patient opted for excision and bypass of the diseased artery. Upon direct visualization, the aneurysm was estimated to measure 8 cm in length and 6 cm in diameter (Figure 5).
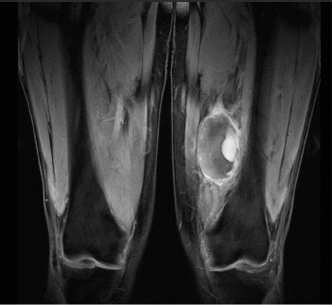
MRI showing vascular mass adjacent to SFA.

Ultrasound revealed an 8.3–cm long SFA aneurysm with a maximum diameter of 5.9 cm.
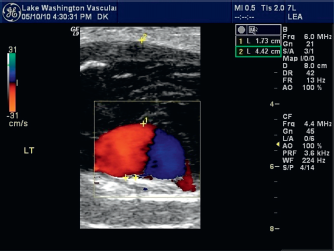
Ultrasound showing patent flow channel with extensive intramural thrombus.

Angiogram of aneurysm, with an estimated length of 5 cm and diameter of 2.5 cm.
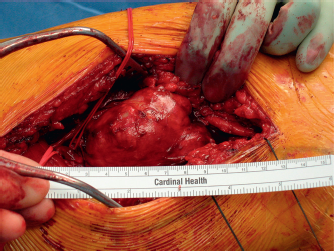
Direct visualization of aneurysm.
It was thought that the angiogram underestimated the true diameter because of the amount of thrombus present in the aneurysmal sac. The aneurysm was excised and was bypassed with a distal superficial femoral to above knee popliteal artery reverse saphenous vein bypass graft (Figure 6). At 6 months postoperatively, the patient is asymptomatic with normal ankle/arm indices.
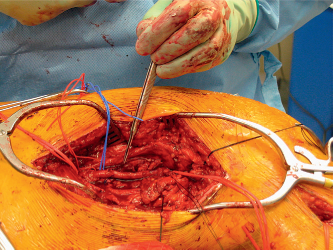
Distal superficial femoral to above knee popliteal artery reverse saphenous vein bypass graft.
Discussion
Much is known about abdominal aortic aneurysms because of their prevalence. However, with SFA aneurysms being a much more elusive disease process, the data are somewhat sparse. Atherosclerosis has often been thought to be the inciting factor of lower-extremity aneurysms. Although, recent research has suggested that aneurysmal disease and atherosclerosis are two distinct entities that often occur in tandem. A genetic predisposition has also been cited. 1 SFA aneurysms tend to effect elderly men more often than women. 2 A review of the available case studies and literature noted a mean age of 75.7, of which 87% were male. 1 Most often patients with SFA aneurysms present with a thigh mass with or without localized pain. 1 Intermittent claudication and/or limb ischemia may be present if the lesion has completely occluded or has showered emboli to the distal runoff.
Identification of a SFA aneurysm can be obtained via MRI, angiogram, or duplex ultrasound. Unfortunately, these aneurysms can mimic soft-tissue tumors on MRI, depending upon the amount of thrombus and its age. If a biopsy were performed, it could prove to be fatal. 3 Angiography is a great tool to assess distal runoff and plan graft placement but it can underestimate the true diameter of the aneurysm if there is a large thrombus filled sac. If an aneurysm has completely thrombosed, it could appear as an occluded vessel as opposed to an occluded aneurysm. In one such instance, the diagnosis of a SFA aneurysm was made only after an above knee amputation. 4 Duplex ultrasound has the advantage of visualizing the hemodynamic flow, aneurysm size, presence of thrombus, and residual lumen. SFA aneurysms tend to be localized to the mid-segment of the vessel and rarely extend into the adductor canal. However, involvement of the entire vessel has been noted. 1 The deeper location of the aneurysm often prevents early identification and patients are often symptomatic by the time they present.
Exclusion of the aneurysm and the reestablishment of distal flow are the principle treatment goals. Surgical excision of the aneurysm followed by a femoral to popliteal bypass graft is the preferred method of treatment. A review of the literature has revealed that vein grafts have been used more often than prosthetic material. Endovascular interventions, although suitable, were not commonly used. 1
Conclusion
Although seemingly rare, SFA aneurysms pose a significant risk for ischemia and limb loss. The key factor in identifying this disease process is effective and high-quality imaging. Duplex ultrasound provides both an anatomic and a hemodynamic evaluation of the arterial system and can provide relevant information in the treatment of this disease process. In our case, duplex ultrasound yielded a more accurate measurement of the true aneurysm size when compared with the angiogram. This is attributable to the angiogram measuring the flow channel of the residual lumen while not visualizing the thrombus-filled sac. However, multiple imaging modalities are often used in concert to provide comprehensive patient care. Allowed to progress untreated, these aneurysms often rupture or thrombose, which can ultimately lead to limb loss. Because of the increased incidence of aneurysmal disease elsewhere in the body, these patients should undergo additional screening.