
Abstract
Celiac trunk aneurysms are a rare and unusual pathology, accounting for roughly 4% of all splanchnic aneurysms; fewer than 180 cases have been reported since 1745. Early recognition of splanchnic aneurysms is crucial because of the operative mortality rate associated with ruptured splanchnic aneurysms. Duplex ultrasound in this case study has proven to be sensitive and specific in the detection of celiac aneurysms.
Introduction
Duplex ultrasound in the detection and diagnosis of visceral vascular pathology is widely accepted as a front-line screening tool despite varying degrees of sensitivity and specificity in visceral vascular ultrasounds. 7 In this case, we used duplex ultrasound to rule out gut ischemia by surveying the splanchnic circulation at protocol specific sites. During the visceral vascular ultrasound examination, the celiac artery was suspected to be aneurysmal, and alternative radiographic confirmation and correlation was sought.
Case History
A 72-year-old African-American woman presented to the noninvasive vascular laboratory with an extensive history of peripheral vascular and cardiac disease. The patient was recently found to be in atrial fibrillation, hypertensive, and have a history of renal artery stenosis. She now presents with dull postprandial pain and unexplained weight loss of 10 pounds over the last 2 months. A mesenteric duplex was ordered to rule out gut ischemia secondary to mesenteric insufficiency.
Imaging Findings
Duplex Ultrasound
Ultrasound Imaging was performed on GE Vivid 7 scanner with the use of a curved array probe (1–4 MHZ). The patient was negative for significant celiac artery (CA), superior mesenteric artery (SMA), and inferior mesenteric artery (IMA) stenosis. However, the proximal to mid-portion of the CA was noted to be heavily calcific and aneurysmal, with a maximal diameter measuring 2.7 cm × 2.6 cm by duplex ultrasound (Figures 5 and 6). There was also aneurysmal flow separation noted within the spectral Doppler and novel aneurysmal color Doppler swirl (Figure 4). Computed tomography angiography (CTA) of her abdomen was ordered to confirm and correlate duplex findings and the possibility of other splanchnic involvement.

CTA of celiac aneurysm.
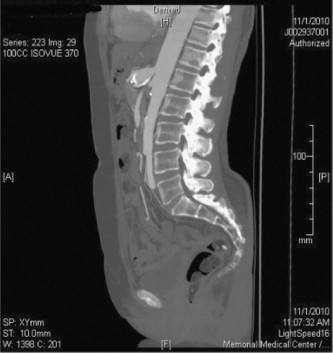
CTA of celiac aneurysm.
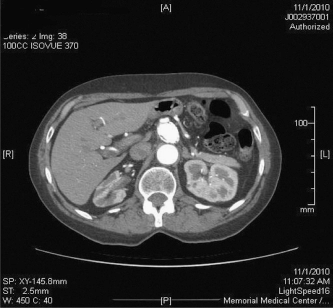
CTA of celiac aneurysm.
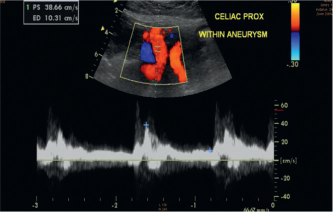
Duplex ultrasound displaying classic aneurysmal Doppler flow separation.
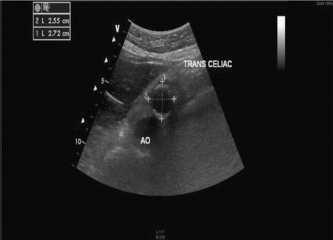
2D ultrasound transverse image of celiac artery aneurysm with calipers.

2D ultrasound sagittal image of celiac artery aneurysm.
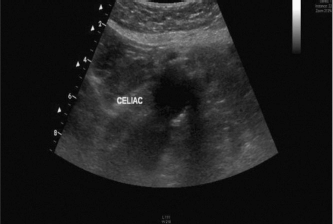
2D ultrasound sagittal image of celiac artery aneurysm.
CTA
The study was administered on a GE 16–slice CT scanner (GE Lightspeed) with an intravenous demonstration of 100 mL/L of Isovue-370 with spiral CT technique of the abdomen along with the superior mesenteric and celiac arteries with and without contrast (Figures 1–3).
The CTA was positive for CA aneurysm measuring 3.0 cm × 3.0 cm with a widely patent SMA and IMA, correlating with duplex ultrasound findings of CA aneurysm. The aneurysm extended to within 3 mm of the left gastric artery origin. The remainder of the distal celiac was unremarkable, giving off splenic and hepatic branches. Dense calcification also was noted in the walls of the aneurysm.
Discussion
Celiac trunk aneurysms are a rare and unusual pathology, accounting for roughly 4% of all splanchnic aneurysms. Fewer than 180 cases have been reported since 1745.1–3,6 The most common pathologic findings of the celiac artery are medial degeneration and atherosclerosis. 1 Only 22% of all visceral aneurysms are detected before rupture and death, with a total mortality rate of 72–87%.1,6 This high incidence of rupture has been reduced to 7% in recent years secondary to the advances in diagnostic imaging, mainly duplex ultrasound.2–4,6
CA aneurysms can be asymptomatic or, more frequently, produce only vague abdominal discomfort. Some patients may not present until the occurrence of aneurysmal rupture. 6 The aneurysm may spontaneously rupture into the peritoneal cavity, retroperitoneum, or thorax. 6 Intraperitoneal rupture is another concern, where the aneurysm may initially be contained within the lesser sac, with subsequent free rupture into the peritoneal cavity, which produces the classic “double-rupture” phenomenon.
Early recognition of splanchnic aneurysms is crucial because the operative mortality rate associated with a ruptured celiac aneurysm is 40% when compared with only 5% for nonruptured aneurysms. 6 Therefore, celiac aneurysms with a diameter >2 cm are considered amenable to surgical or endovascular repair; the origin and anatomy of the aneurysm will determine the type of intervention.1,2
Conclusion
Duplex ultrasound has shown to be a valuable tool in the detection of celiac aneurysms. Although there was a 3-mm discrepancy between CTA and duplex diameter measurement correlation, duplex ultrasound was sensitive enough to detect the aneurysm, which in turn lead to CTA for a confirmation study.
This case study demonstrates duplex ultrasounds sensitivity in detecting splanchnic circulation vessel abnormalities. Early detection of these abnormalities through ardent sonographic principle and clinical manifestation adds to the overall reduction of CA rupture and their associated mortality rates. Unfortunately, at the time of writing, the patient in this case was not a candidate for endovascular or operative repair because of her cardiac status.