
Abstract
Introduction
Arteriovenous malformations (AVMs) are abnormal, direct connections between the arteries and veins. AVMs are most commonly associated with the brain and spinal cord; however, they can occur in any part of the body. Duplex ultrasound can play a pivotal role in both the diagnosis and treatment of AVMs.
Methods
A high-resolution duplex ultrasound machine along with a high-frequency 15–7 MHz probe was used in transcatheter techniques to treat an AVM. Ultrasound was used to guide arterial and venous access, target specific vessels for treatment, and ultimately reduce radiation exposure.
Case Report
A 6-year-old female patient was diagnosed with a left foot AVM and hemihypertrophy (Parkes Weber). Despite previous treatments with coil embolization, the patient developed discoloration and swelling of the left second toe and a nonhealing ulceration on the plantar aspect of the left foot. Duplex ultrasound was used to confirm the diagnosis and to aid in the treatment of the AVM. Under ultrasound guidance, catheter access was achieved via the dorsalis pedis artery and advanced distally into a large digital artery directly associated with the AVM. Anhydrous ethanol alcohol was injected through the catheter to treat the arterial inflow of the AVM. Ultrasound was then used to identify cavernous veins on the plantar aspect of the foot and to guide direct ethanol injections into the affected veins. Two weeks after the procedure, ultrasound confirmed 90% reduction in the AVM. The patient's toe discoloration resolved, and the ulceration healed.
Conclusion
Undiagnosed or poorly managed AVMs of the extremities can result in multiple surgical resections and skin deterioration. Ultrasound imaging of arteriovenous malformations with B-mode, color, and Doppler is essential for the evaluation (staging), treatment, and follow-up of vascular malformations. Ultrasound-guided transcatheter and direct techniques can be used in the treatment and prolonged management of AVMs. The application of ultrasound during these treatments will reduce radiation exposure in these patients.
Introduction
Arteriovenous malformations (AVMs) are abnormal, direct connections between the arteries and veins. AVMs can be characterized as a tangle of blood vessels often referred to as the nidus. In the presence of an AVM, the oxygen-rich blood bypasses the capillary beds and is transferred directly into the venous system. AVMs most commonly occur in the central nervous system; however, they can be found in any part of the body. AVMs are high-flow volume systems; therefore, they can be the source of significant pain. Certain conditions are characterized by the presence of high-flow AVMs, such as Parkes Weber hemihypertrophy. This case study identifies a patient who has Parkes Weber hemihypertrophy of the left leg with a left foot AVM. The AVM was treated with ultrasound-guided injections of ethanol and sclerotherapy. 5
Methods
A high-resolution duplex ultrasound machine along with a medium frequency 7–4 MHz probe was used to identify and aid in the diagnosis of a left foot arteriovenous malformation. A high-frequency 15–7 MHz probe was used to guide arterial and venous access and target specific vessels for transcatheter techniques to treat an arteriovenous malformation. The use of ultrasound in cases such as this can ultimately reduce radiation exposure.
Case Report
A 6-year-old female patient presented with the chief complaint of left leg warmth and discrepancy in size, with left larger than the right (Figure 1). Angiography was used to confirm the presence of a left foot AVM (Figure 2). The patient was diagnosed with Parkes Weber hemihypertrophy and a left foot AVM. The patient underwent several coil embolization treatments over the course of 13 months. These initial treatments diminished the size of the AVM and alleviated some of the patients' symptoms. The patient went without further treatment for the next 2 years (26 months). Without treatment, progressive discoloration and enlargement of the left second toe occurred (Figure 3); the length of the legs did not appear to have increased much during the 2-year period. The patient, now 9 years old, returned after minor trauma to the left foot. A nonhealing ulceration on the plantar aspect of the left foot was apparent (Figure 4), as well as discoloration and swelling of the left second toe. On physical examination, the left second digit appeared blue with necrotic skin on the plantar aspect and the web between the first and second digits. Ultrasound confirmed an increase in the size of the AVM. A treatment plan was developed for this patient, including ultrasound-guided transcatheter and direct injection techniques.

Size discrepancy, left greater than right, is shown in our female patient with Parkes Weber hemihypertrophy.

An angiogram depicting the left foot arteriovenous malformation; the arrow is pointing to the nidus.

Left second-digit staining and edema.

Open ulceration, necrotic tissue, and skin blistering on the plantar aspect of the left second digit and foot.
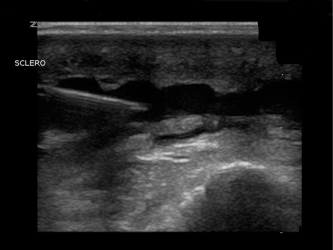
Because of the significant pain associated with ethanol alcohol injection, the patient was placed under general anesthesia (Figure 5) for postprocedure pain management. A high-frequency 15–7 MHz probe was used to identify the dorsalis pedis artery (DPA) (Figure 6). Under ultrasound guidance, a 21-gauge needle was used to achieve access via the DPA. A wire (Figure 7) followed by a sheath was placed within the vessel. Under ultrasound guidance, a catheter was advanced within the DPA; we lost sight of the catheter at the level of the plantar arch because of shadowing from overlying boney structures. At this point fluoroscopy was used to guide the catheter further distally into the inflow artery closer to the nidus. Ethanol was injected through the catheter (Figure 6).

With the patient placed under general anesthesia, a high-frequency 15–7 MHz probe is used to identify the dorsalis pedis artery.
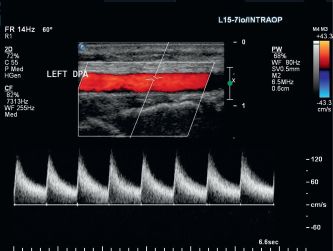
Duplex ultrasound depicts the dorsalis pedis artery in a sagittal plane with low-resistive, high-end diastolic Doppler flow pattern.

B-mode is used to depict a wire within the dorsalis pedis artery.
Ultrasound was then used to identify the cavernous veins on the plantar aspect of the foot associated with the AVM. A 21-gauge needle was used to gain access to these veins (Figure 8). A live B-mode image demonstrated the direct injection of ethanol alcohol (Figure 9).
A 21-gauge needle is placed within the cavernous veins on the plantar aspect of the foot.
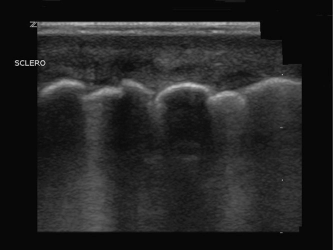
B-mode depicts the ethanol bubbles within the cavernous veins on the plantar aspect of the foot.
The patient returned 2 weeks post procedure for follow- up. The ulcer had healed (Figures 10 and 11), and the AVM was evaluated with ultrasound. The size of the AVM shrank substantially, i.e. approximately 90% per the physician's note. The patient will continue to follow-up with repeat duplex examinations. Further embolization treatments may be performed as needed.

This image, taken eight days post procedure depicts healthy, supple skin tissue on the plantar aspect of the left second digit.

This image depicts healthy, supple skin tissue between the first and second digits.
Discussion
Parkes Weber syndrome is often referred to, or combined with, Klippel-Trenaunay syndrome. Both syndromes have similar presentations, including limb enlargement, discoloration, varicosities, and capillary malformations; however, it is important to distinguish the difference for therapeutic planning and outcomes. Parkes Weber syndrome consists of high-flow AVMs with subsequent soft tissue and bone hypertrophy of the affected limb. The affected limb continues to grow past the age of 10 years of age until epiphyseal closure. Parkes Weber patients may develop high-output cardiac failure because of the arteriovenous shunting. Klippel-Trenaunay syndrome is a low-flow condition with malformations of the capillary, venous and lymphatic systems. Minimal intervention is clinically indicated in patients in Klippel-Trenaunay. Minor surgical procedures may be performed, such as treatment of varicose veins and venous malformations. 1
Ethanol embolotherapy has proven clinically to improve treatment results with an acceptable rate of morbidity. According to Do et al, 2 “[E]thanol has the unique ability to induce protein denaturation in endothelial cells with subsequent vessel wall denudation and thrombus formation, which results in the complete obliteration of the vessel lumen rather than simple obstruction.” Transarterial catheterization can provide direct access to the nidus and may aid in the prevention of major complications. Most common ethanol complications include localized tissue damage, such as skin blistering or necrosis; however, in extreme cases it may cause nerve damage.2–4,6
Sclerotheraphy is a common practice used in treating varicose veins and vascular malformations. Sclerotherapy is a technique that involves injecting medicine directly into the affected veins. A few common medicines typically used for sclerotherapy include ethanol alcohol, sotradecol, and polidocanol. Although ethanol was chosen in this particular case, there are alternative medications available.
Sotradecol is the common name for sodium tetra-decyl sulfate, which is a sclerosing agent commonly used to treat small varicose veins and may be used in treating some cases of malformation. Sotradecol and polidocanol act in a similar manner as an irritant to the vessel intima, which induces thrombus formation. Consequential fibrous formation around the vessel leads to partial or complete disintegration.2,3
Although transcatheter embolization techniques can provide symptomatic relief, many lesions may recur. These lesions may require multiple treatments; therefore, ultrasound is a safer alternative to fluoroscopy. Fluoroscopy exposes the patient to harmful ionizing radiation. Ultrasound directed treatments are noninvasive, cost-effective, easily reproducible procedures that can sometimes be performed on an outpatient basis.
Conclusion
Undiagnosed or poorly managed AVMs of the extremities can result in multiple surgical resections, skin deterioration, and in extreme cases can lead to decreased cardiac function. Duplex ultrasound can be used to effectively diagnose the presence of an AVM as well as aid in transcatheter and direct techniques for treatment. Ethanol injections and sclerotherapy may not be a one-time cure; however, it is an effective treatment in the long-term management of pain symptoms and tissue break down. Patients with malformation may require ongoing treatment throughout the course of their lifetime; therefore, ultrasound directed treatments could significantly reduce their exposure to radiation.