
Abstract
Endovascular intervention has emerged as a first-line therapy for peripheral arterial occlusive disease. Duplex ultrasound has been used for surveillance after vascular interventions and is an integral component for evaluating patients after endovascular procedures. Technical protocols vary; however, most include color flow imaging and pulsed Doppler with an emphasis on single plane long-axis imaging. Exclusion of short-axis imaging, however, may miss pathologies involving the medial or lateral vessel wall. This report will describe the importance of imaging in multiple planes for evaluation of the peripheral arteries in patients after endovascular interventions.
Introduction
Endovascular intervention has gained widespread acceptance as the first line of therapy for both iliac and femoropopliteal atherosclerotic occlusive disease. 1 Duplex ultrasound (DU) scanning has been applied extensively to the follow-up of vascular interventions and is an integral component in the evaluation of patients after these endovascular procedures. 2 Technical protocols vary; however, most include color flow imaging and pulsed Doppler waveform analysis proximal to, at and distal to the site of intervention with an emphasis on long-axis imaging. 3 However, if short-axis imaging is excluded, pathologies involving the medial or lateral arterial vessel wall may not be detected. We describe a case in which the transverse sweep of a lower-extremity arterial stent revealed a pseudoaneurysm that was not appreciated in the sagittal plane.
Patient History
The patient was a 61-year-old man with a history of diabetes, hypertension, and myocardial infarction who presented to the vascular laboratory for a preoperative assessment before coronary artery bypass graft surgery (CABG). The patient complained of calf claudication but offered no other complaints relevant to the lower extremities. The patient did not present with any signs or symptoms to suggest the presence of pseudoaneurysm. He offered a history of unspecified peripheral arterial disease that was treated at an outside facility with bilateral lower extremity stents. An arterial DU of the bilateral lower extremities was ordered as part of the preoperative work-up for CABG and to further elucidate the situation.
Imaging Findings
The study was performed on a Philips HD-11 ultrasound machine with the use of a high-frequency (3–9 MHz) linear array transducer. Given the vague history offered by the patient, the short-axis approach was used to determine the length and locations of the arterial stents. Long-axis imaging was used to evaluate for the presence of any hemodynamically significant stenosis proximal to, within, and/or distal to the stent body. Long-axis DU on the right revealed a patent superficial femoral artery (SFA) with stents in the mid to distal thigh and no hemodynamically significant flow disturbance or other pathology noted. However, a transverse sweep revealed a mid stent body pseudoaneurysm (PA) at the level of the mid-thigh that measured AP 1.5 cm × TRV 1.6 cm. The PA arose from the medial wall of the SFA and was not similarly demonstrated with the transducer in a sagittal orientation. This failure was attributed to the medial wall origin of the PA. Images demonstrating coaptability of the femoral vein at the site of the pseudoaneurysm were obtained to avoid confusing the gray-scale images for a deep vein thrombosis of the femoral vein at that level. Arterial DU of the left lower extremity in the sagittal and transverse planes demonstrated a stented SFA with multiple areas of stenosis but yielded no evidence of PA.
Discussion
Percutaneous transluminal angioplasty was first described by Dotter and Judkins 1964 4 and has since emerged as the first-line treatment of choice for most occlusive lesions in the iliofemoral segment. 1 However, long-term durability can be marred by early or late complications, and routine surveillance and early detection of these complications is imperative.
Although, other imaging modalities such as contrast, computed tomography, and magnetic resonance angiography provide a broader plane of view to assess the integrity of the artery and stent in the postintervention patient, because of the relatively superficial and easy to access location of the SFA, and because of its noninvasive nature, duplex ultrasound is the ideal surveillance tool in this setting. However, ultrasound images obtained in the sagittal or transverse planes only, represent a “thin slice” of the anatomy being imaged and DU imaging with the transducer in a single plane or orientation exclusively may not detect vital information during routine follow-up assessment post intervention. Although traditional long-axis DU imaging of arterial stents is ideal for the detection of hemodynamically significant stenotic lesions, more rare complications such as PA can easily go undetected when only single plane imaging is used.
In this case, long-axis DU scanning alone failed to produce images that were necessary in order to diagnose the presence of the PA. This was thought to be attributable to the medial wall origin of the lesion (Figures 1–3). Additional scanning, from multiple projections, with the transducer aligned to the short axis of the vessel easily visualized the presence of the PA.
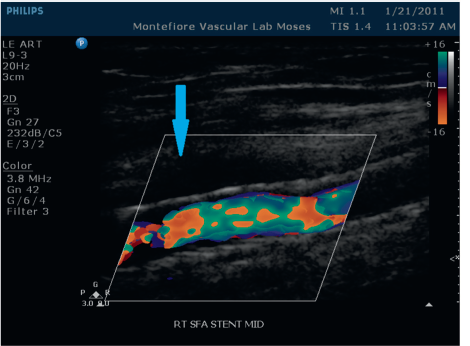
This image was obtained with the transducer sagittal to the long axis of the SFA at the level of the stent. No gross evidence of pseudoaneurysm is seen in this projection. In retrospect, the anechoic area connoted by the blue arrow was subtle evidence of the presence of the pseudoaneurysm.
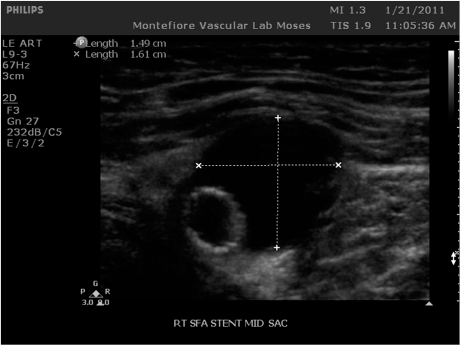
This image was acquired with the transducer aligned to the short axis of the vessel at the same level of Figure 1. A large anechoic area medial to the vessel wall is clearly seen.
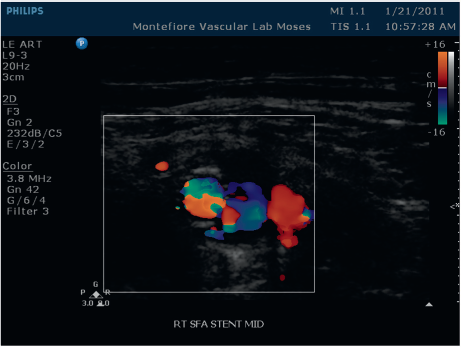
Color flow image confirming the presence of a pseudoaneurysm. Note that the pseudoaneurysm is not in a typically located position (i.e., anterior and superficial to the vessel).
Conclusion
When used together, sagittal and transverse imaging in multiple planes allows for three-dimensional visualization and assessment of any postintervention complications after peripheral artery stent placement. This three-dimensional approach to DU can have a profound impact on the long-term patency and integrity of the stent and the overall well being of the patient by detecting medial or lateral wall pathology that may not otherwise be appreciated. To maximize the efficacy of the DU technique, we recommend that all poststent placement protocols include combinations of the long- and the short-axis from multiple views at the level of the stent.