
Abstract
Introduction.
—According to Beppu et al., spontaneous echocardiographic contrast (SEC or smoke) is a pattern of “spontaneous swirling echoes originally visualized by transthoracic echocardiography in the enlarged left atrium of patients with mitral stenosis” (J Am Cardiol 1985;6:744–749). It has since been primarily associated with atrial fibrillation and flutter. The clinical significance of SEC is its association with left atrial thrombus, increased thromboembolic complications, and death. The pathogenesis of SEC seems to involve Rouleau formation between red cells and fibrinogen at low shear rates, which is an in vitro equivalent of blood stasis. Black noted that “Red cell aggregation, manifested as SEC, appears to be a precursor to thrombosis. Left atrial thrombi are rich in fibrin and red cells, resembling venous more than arterial thrombi” (Echocardiography 2000;17(4):373–382).
Methods.
—If left atrial thrombi are associated with SEC and resemble venous thrombi, it was hypothesized that actual venous thrombi in previously undescribed locations, most notably deep vein thrombosis, may equally be associated with SEC. We asked our coauthors (H.T. and M-C.Y.) to search for such a phenomenon among patients referred to the vascular laboratory for suspected venous thrombosis.
Case Presentation.
—In the following case series, we report an original phenomenon of swirling echogenicity in the venous system that we believe is SEC. The phenomenon was fairly rare (maximum 1.5% of referred patients, whereas deep venous thrombosis itself was 15-20%). The clinical significance of this phenomenon is discussed.
Introduction
Spontaneous echocardiographic contrast (SEC or smoke) is a pattern of spontaneous swirling echoes originally visualized by transthoracic echocardiography in the enlarged left atrium of patients with mitral stenosis” (Figures 1–3). 1 It has since been primarily associated with atrial fibrillation and flutter (Table 1). The clinical significance of SEC is its association with left atrial thrombus, increased thromboembolic complications, and death. 2
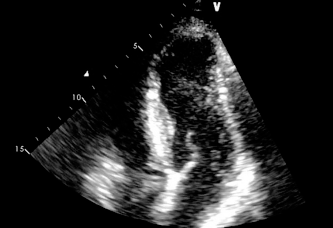
SEC in the left atrium of a patient with mitralstenosis (1/3).
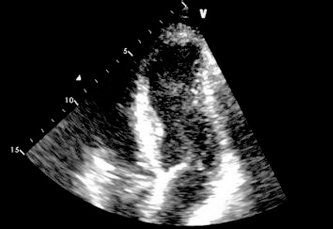
Mitral stenosis (2/3).
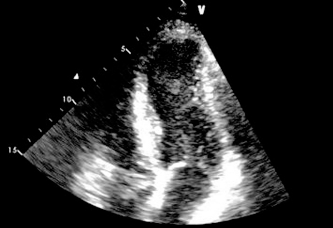
Mitral stenosis (3/3).
Literature Pertaining to Spontaneous Echocardiographic Contrast (1996–2012) *
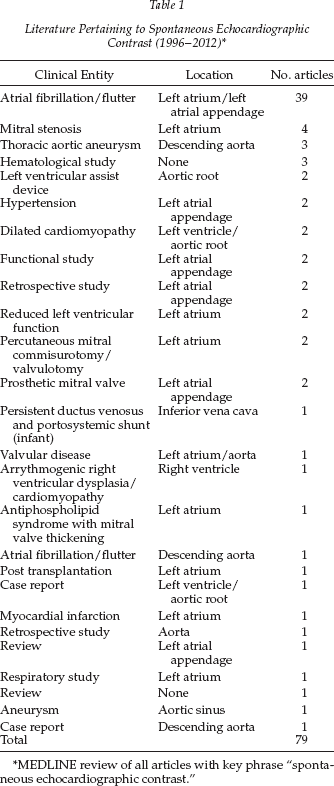
MEDLINE review of all articles with key phrase “spontaneous echocardiographic contrast.”
The pathogenesis of SEC seems to involve Rouleau formation between red cells and fibrinogen at low shear rates, which is an in vitro equivalent of blood stasis.3,4 Black 5 noted that “Red cell aggregation, manifested as SEC, appears to be a precursor to thrombosis. Left atrial thrombi are rich in fibrin and red cells, resembling venous more than arterial thrombi.” 6
If left atrial thrombi are associated with SEC and resemble venous thrombi, it was hypothesized that actual venous thrombi in previously undescribed locations, most notably deep vein thrombosis (DVT), may equally be associated with SEC. We asked our coauthors (H.T. and M-C.Y.) to search for such a phenomenon among patients referred to the vascular laboratory for suspected venous thrombosis.
In the following case series, we report an original phenomenon of swirling echogenicity in the venous system that we believe is SEC. The phenomenon was fairly rare (maximum 1.5% of referred patients, whereas DVT itself was 15–20%). The clinical significance of this phenomenon is discussed.
Case Reports
Case 1
Mrs. B, a 62-year-old Peruvian woman with a previous history of asthma (>40 years), type II diabetes, and hypothyroidism.
HPI.
The patient fell in Peru and fractured her left humerus 3 weeks before admission. After the fall, she complained of increasing pain, redness, and tenderness in her left calf. She was seen in the emergency department on August 29, 2012, and investigated for suspected DVT. Computed tomography scan was interpreted as follows: “At the level of the junction of the external and internal iliac veins, the left common iliac vein appears extremely hypoplastic or collapsed. This may be either developmental or related to the May-Thurner syndrome.”
Vascular Lab Report.
September 2, 2012: the patient presented with 3+ swelling in the thigh and calf, left greater than right. On the left side we noted an abnormal venous flow of almost 0 at common femoral vein level suggestive of proximal extrinsic compression or partial thrombosis of iliac vein. Femoral vein under tension 3+. Acute DVT of the distal popliteal and multiple soleal veins also was witnessed; otherwise, results were normal up to common femoral vein. The patient was treated with enoxaparin and coumadin, and her calf pain quickly improved.
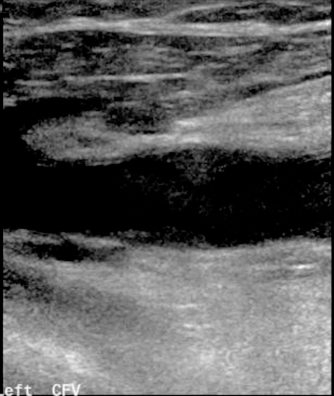
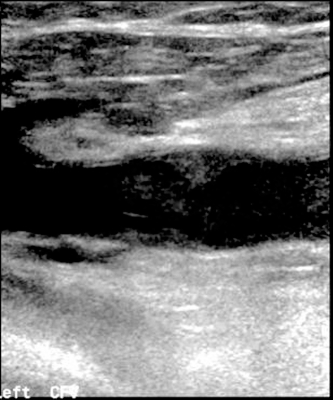
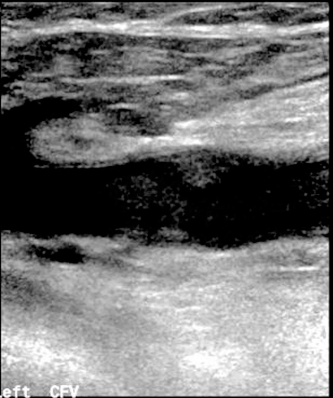
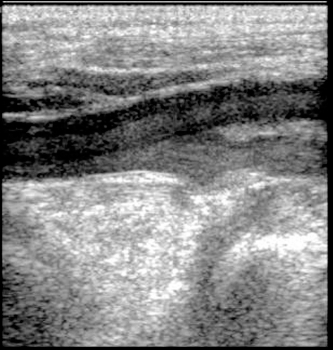
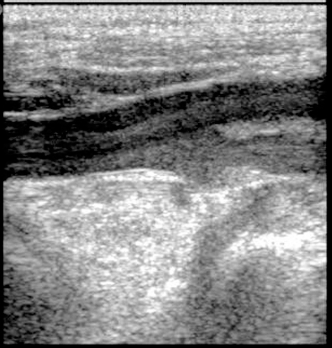
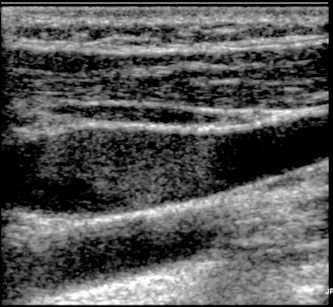
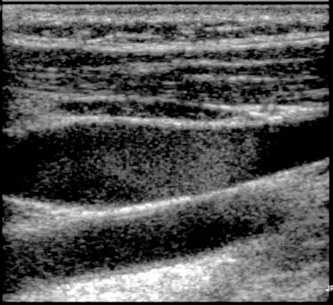
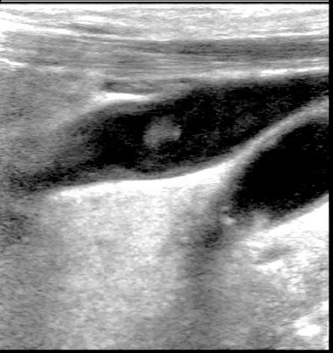
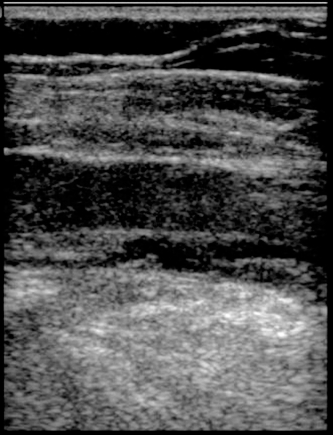
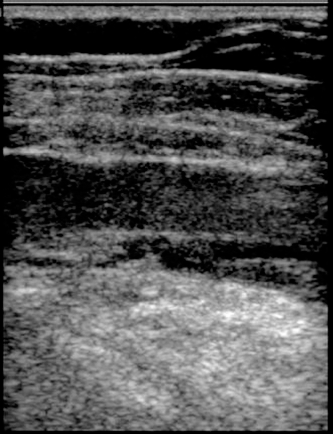
SEC Report.
There was a slow-stagnant flow phenomenon in the midstream of the left common femoral vein (Figures 4–6), which demonstrated spontaneous echogenicity.
Case 1 - Flow in the left common femoral vein demonstrating SEC (1/3).
Case 1 - Left common femoral vein SEC (2/3).
Case 1 - Left common femoral vein SEC (3/3).
Case 2
Mrs. C., a 62-year-old woman with a history of advanced cervical cancer complicated by hydronephrosis.
HPI.
The patient was initially diagnosed with stage IIIa, grade 3 adenosquamous cervical carcinoma in May 2011 and treated with chemoradiation for 2 months. The cancer recurred and was complicated by right-sided hydronephrosis requiring surgery in February 2012. Four months later, she began to complain of pain in the right hip posteriorly as well as the posterior thigh with shooting pains down the leg. She was sent to the vascular laboratory for suspected DVT.
Vascular Lab Report.
August 31, 2012: This is a patient with recurrent cervical carcinoma adherent to the pelvic sidewall. She is feeling numbness and pain increasing in the right leg. Laboratory findings indicated right leg soleal vein thrombosis (calf muscle). A follow-up study was undertaken on September 14, 2012, in which it was noted that right posterior tibial and right peroneal and right calf muscle venous thrombosis represented an extension of DVT in the right leg.
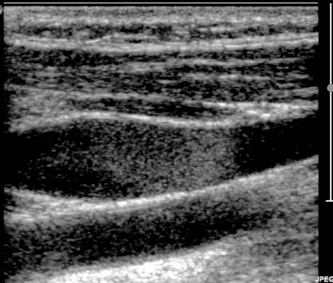
SEC Report.
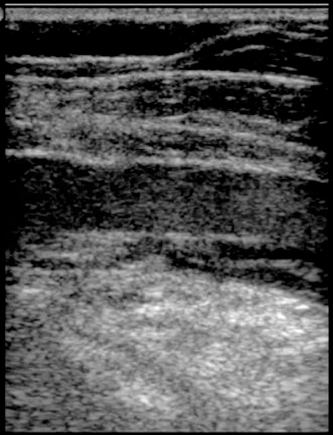
At the bifurcation of the right common femoral vein, we see faster flow in the midstream with increased echogenicity. There is a respiratory cycle with decreased flow on inspiration. Antegrade flow to the heart is preserved, i.e., there is little evidence of circular or retrograde flow at this level. Some blood elements appear to be totally stagnant, although there is no thrombus. There is evidence of mild retrograde flow at the level of the right popliteal vein (Figures 7–9).
Case 2 - Right common femoral vein SEC (1/3).
Case 2 - Right common femoral vein SEC (2/3).

Case 2 - Right common femoral vein SEC (3/3).
Case 3
Mrs. R., a 58-year-old woman with a previous history of rectal carcinoma, hypertension, and coronary artery disease.
HPI.
The patient was diagnosed with localized rectal adenocarcinoma in June 2009. She was treated with surgery and ileostomy, neoadjuvant chemoradiation, and adjuvant chemotherapy. A positron emission tomography scan taken in August 2012 was suspicious for inferior internal iliac nodes. The patient was receiving chemotherapy through a left-sided PICC (i.e., peripherally inserted central catheter) line when the treating oncologist noted 3+ swelling of the left side of the neck. He requested an urgent carotid duplex to rule out thrombosis on September 18, 2012.
Vascular Lab Report.
September 19, 2012: Acute DVT of brachial, axillary, and subclavian veins was noted, along with external jugular vein thrombosis and patent internal jugular, ulnar, and radial veins.
SEC Report.
The left internal jugular showed a huge mass of echogenic red cells moving back and forth with minimal respiratory change. The vein was distended but compressible (see Figures 10–12).
Case 3 - Left internal jugular SEC (1/3). Case 4
Case 3 - Left internal jugular SEC (2/3).
Case 3 - Left internal jugular SEC (3/3).
Mr. T., a 77-year-old man with an extensive problem list, including dyslipidemia, hypertension, atrial fibrillation, chronic obstructive pulmonary disease, benign prostatic hypertrophy, remote DVT (1998), remote coronary artery bypass graft (1998), diverticulosis, chronic renal failure and nephrotic syndrome, diabetes type II, gastroesophageal reflux disease, and arterial occlusive disease (both legs).
HPI.
The patient was seen in the emergency department on August 30, 2012, where he presented with severe anemia (Hb = 62) and positive occult blood. He underwent a colonoscopy on September 4, 2012. A 2- to 3-cm cecal polyp was discovered, which was confirmed by the pathology report to be invasive intestinal type adenocarcinoma. No metastatic disease was reported. The patient under went right hemicolectomy (September 6, 2012) with ileocolic anastomosis, which was complicated 10 days later by possible small bowel obstruction with excess free air. A follow-up laparotomy to redo the ileocolic anastomosis was performed. The patient subsequently began to complain of left arm swelling and tenderness and was referred to the vascular lab for suspected DVT.
Vascular Lab Report.
September 27, 2012: Abnormal flow at the subclavian vein level was found, along with decreased amplitude compared with the right side suggestive of proximal extrinsic compression or partial thrombosis, No DVT was encountered up to the axillary vein. The internal jugular was patent, and the subclavian vein appeared patent but could not be fully visualized
SEC Report.
There was good flow in the left internal jugular vein, which demonstrates bidirectional, circular echoes. There may be evidence of constriction, possibly attributable to a probe artifact. Different echogenicity of red cell elements suggests different sized aggregates. Flow appears slower in the midstream of the left brachial vein (see Figures 13–15).

Case 4 - Left internal jugular SEC (1/3).
Case 4 - Left internal jugular SEC (2/3).

Case 4 - Left internal jugular SEC (3/3).
Case 5
Mrs. T, a 49-year-old woman with a history of recent DVT/pulmonary embolism.
HPI.
The patient was previously in good health until she presented to an Ontario hospital with DVT/pulmonary embolism in August 2012. She was admitted to a nearby hospital in September with vague abdominal pain. An abdominal computed tomography scan showed a 10-cm ovarian mass with cystic and solid features. Further, there was mild left internal, external, and common iliac lymphadenopathy with numerous liver hypodensities. CA-125 was markedly increased (383, normal = 0–35). Follow-up ultrasound was highly suspicious for malignant ovarian neoplasm. She was referred for assessment by gynecological oncology of the Jewish General Hospital, who recommended urgent total abdominal hysterectomy with bilateral salpingo-oopherectomy. A follow-up duplex scan was ordered.
Vascular Lab Report.
October 9, 2012: No DVT was encountered on the right side up to common femoral vein. Chronic changes consistent with previous thrombosis were found on the left side. A thrombus in the distal popliteal vein of 50% diameter was found, as well as in the peroneal and soleal veins. Thickening of the veins was noted. Otherwise, the findings were normal up to common femoral vein.
SEC Report.
There was echogenicity of blood elements in the midstream of the right common femoral, which demonstrates fast flow. It was possible to notice a slower flow phenomenon with echogenicity closer to the vessel wall (similar to other cases). Echoes were found equally in the left common femoral and the right popliteal vein. Note that these echoes were unchanged while the patient was positioned (Trendelenburg, reverse Trendelenburg; see Figures 16–18).
Case 5 - Right common femoral SEC (1/3).
Case 5 - Right common femoral SEC (2/3).
Case 5 - Right common femoral SEC (3/3).
Discussion
Although we are dealing with a very small case series, it is possible to visualize certain associations between the patients. For example, most of the cases had documented DVT as well as SEC, although these two phenomena did not occur in the same vein. There was a strong association with cancer (4/5 cases), which is hypothesized to be a hypercoagulable state. 7 Another strong association is stasis and sometimes-venous compression, which points to a second arm of Virchow's triad. It is at present unknown how SEC might be linked to endothelial damage.
As opposed to the classical SEC of the left atrium, venous SEC is a much more unusual entity. During a period of 2 months, five cases were discovered among approximately 300 patients referred for suspected DVT, which would suggest a rate of 1–2% among highly suspicious cases. In the left atrium, SEC frequently coexists with mural thrombus and is actually more common. 8 We have found that venous SEC does not coexist with DVT, is usually one-sided, and is about 10% as common as DVT in referred cases.
Because this is a preliminary study, it is difficult to speculate on the significance of venous SEC. A conservative approach involving repeat duplex scanning would appear to be prudent at this point. The patients could be recalled and assessed for potential DVT in the future. Because most of the patients were anticoagulated because of previous or ongoing DVT, we did not find SEC in isolation in an otherwise-healthy patient. In such an instance, follow-up and possibly antiplatelet agents might be considered.
Footnotes
Acknowledgments.
Many thanks to Jean Marcotte of the medical photography department for his diligent efforts in capturing still images from the patient videos and Marie-Josée Blais of the echocardiography lab for sharing her video of SEC in the left atrium.