
Abstract

Case Report
A 50-year-old woman with a history of end-stage renal disease secondary to longstanding type I diabetes mellitus had received a simultaneous pancreas-kidney transplant 15 years previously. Her postoperative course was uncomplicated, and she was seen regularly for routine follow-up. At a recent visit, findings of the physical examination revealed an abdominal bruit over the right lower quadrant and the findings of a laboratory evaluation demonstrated increased lipase and glucose levels. An ultrasound of the pelvis was performed, which showed the transplanted pancreas in the right iliac fossa and an associated large structure measuring 2 cm with turbulent flow (Figure 1). Presumed diagnoses of a pseudoaneurysm versus an arteriovenous fistula (AVF) were considered. Computed tomography angiography was performed to further assess these assumptions. The result suggested an arteriovenous fistula between a branch of the superior mesenteric artery and the outflow vessel of the portal vein (Figure 2).
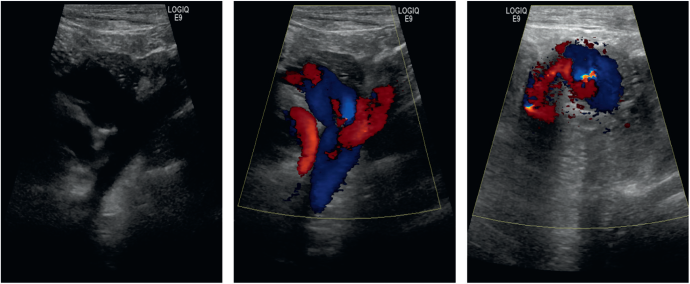
Ultrasound of the right iliac vessels and vessels supplying the transplant pancreas (left and center) as well as turbulent blood flow within the fistula (right).
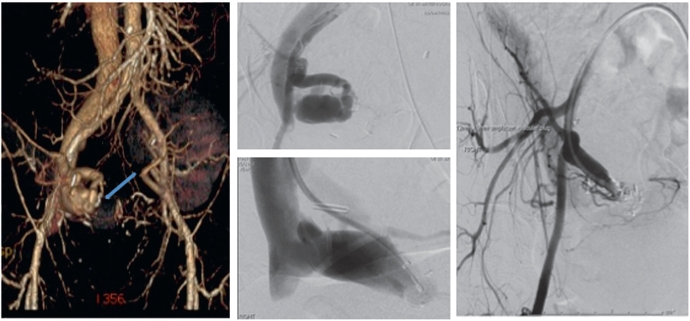
Computed tomography angiography showing AVF (left). Angiogram demonstrating the AVF (center, top). Plug placed at inflow of the AVF (center, bottom). Physiological blood flow after definitive plug deployment and detachment (right).
Results
The patient was admitted to the vascular surgery service for hydration and renal protective protocol (creatinine of 1.8 mg/dL, baseline 1.2 mg/dL) before angiography. Under local anesthesia, arterial and venous accesses were obtained via the left femoral artery and the right femoral vein. Angiography of the venous and arterial system delineated the inflow vessel and confirmed an AVF. Endovascular embolization with a 12 × 9-mm Amplatzer Vascular Plug II (AGA Medical Corp. Plymouth, MA) was performed. The postprocedure angiography showed no flow in the AVF and enhancement of both the parenchyma and arterial system of the pancreas (Figure 2). Ultrasound postdischarge demonstrated physiological perfusion of the pancreas and absence of flow within the AVF (Figure 3).
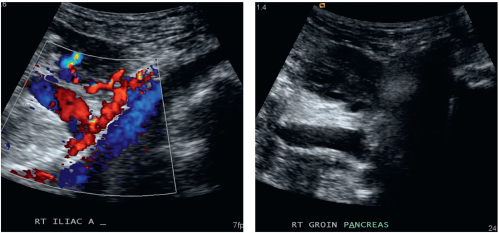
Color (left) and B-Mode (right) after embolization with no AVF detected.
Discussion
When vascular disorders attributable to transplanted pancreas are suspected, ultrasound remains the most common diagnostic method used. It is highly sensitive for detecting peripancreatic fluid collections, pseudoaneurysms, and AVFs. 1 Pseudoaneurysm and AVF of the transplant arteries can occur but are reported as a rare complication. 2 If not treated, this can lead to pelvic hemorrhage, hematuria, graft dysfunction, or failure.2,3 Several reports have described open techniques for treatment of pancreatic AVFs; however, this can be complicated potentially leading to the loss of the transplant.
Several types of devices, which include coils and balloons, can be used for embolization. The Amplatzer plug is a multilayered nitinol wire mesh shaped into three separate lobes. Unlike other embolization devices, it can be recaptured and repositioned to allow accurate deployment. 4 Although angiography remains the gold standard for diagnosis and direction for endovascular or surgical intervention, embolization offers an alternative therapy with minimal morbidity. Percutaneous embolization has limitations, which may not permit it to be an entirely innocuous option 1 ; however, if practical it can prevent the need for operative intervention.