
Abstract
Introduction.
—Deep vein thrombosis should be considered as one of the differential causes of unilateral lower-extremity swelling. When the lower-extremity venous duplex ultrasound is negative for a deep vein thrombosis and a proximal occlusion is suspected, investigation should be completed with interrogation of the pelvic veins.
Case Report.
—We describe a 66-year-old man with a history of rectal carcinoma treated with chemotherapy, radiation, and proctosigmoidectomy who presented to the vascular laboratory with left lower-extremity swelling and erythema. A lower-extremity venous duplex was performed with a Phillips iU22 9–3 MHZ linear transducer, which revealed monophasic flow in the distal left external iliac vein with normal compression images. Further evaluation with a 5–1 MHZ curved array probe revealed a velocity shift within the external iliac vein consistent with iliac vein stenosis. A venogram confirmed a critical stenosis in the mid left external iliac vein with associated thrombus. The patient underwent mechanical thrombectomy and placement of 10 by 40 mm Smart stent. Post-interventional venogram demonstrated excellent antegrade flow and no evidence of residual thrombus.
Discussion.
—If left untreated, venous stenosis may predispose the patient to persistent lower extremity swelling, venous thrombosis, and venous stasis ulcers. Because of the underlying anatomic defect, symptoms may not improve with conservative management, including anticoagulation. Several diagnostic modalities can be considered for diagnosis of the venous stenosis, including venous duplex ultrasound, magnetic resonance venography, computed tomography with venous phase, venography, and intravascular ultrasound.
Conclusion.
—Cost considerations makes venous duplex a valuable, noninvasive, first-line method to investigate suspected venous stenosis.
Introduction
Duplex ultrasound (DU) has been a very successful method for initial assessment of deep vein thrombosis. The presence of swelling and pain of the lower extremity and monophasic flow in the external iliac vein on an otherwise-negative venous duplex is suggestive of a more proximal thrombosis or occlusion. We report the use of venous DU to diagnose iliac vein stenosis on a patient with radiation-induced venous stenosis.
Case Presentation
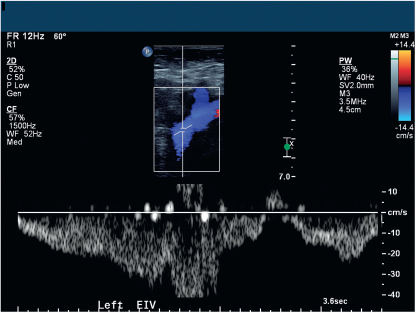
We present a 66-year-old man with a history of essential hypertension and metastatic rectal carcinoma who was treated with chemotherapy, radiation, anterior protosigmoidectomy, and recent resection of a 3-cm metastasis to the liver. The patient was evaluated for left lower extremity swelling and erythema. Given the patient's history of malignancy, deep venous thrombosis was suspected, and further investigation was conducted. A venous duplex study was negative for deep vein thrombosis of the left lower extremity but revealed monophasic flow within the left distal external iliac iU22 5–1 MHZ curved array transducer vein, suggestive of more proximal disease (Figure 1). Monophasic flow was also noted at mid common iliac vein, just distal to the stenosis (Figure 2). Venous DU (Phillips, Bothell, WA) of pelvic veins demonstrated a velocity shift from peak systolic velocity 32 cm/sec to peak systolic velocity 150 cm/sec in the left mid-external iliac vein, consistent with a 50–99% stenosis (Figures 3 and 4). Findings on cava-gram confirmed severe stenosis and thrombus within the left external iliac vein (Figures 5 and 6). A mechanical thrombectomy was performed, and a 10- by 40-mm Smart stent was placed. A postintervention venogram showed a widely patent iliac vein with no evidence of thrombus (Figures 7 and 8). A follow up venous duplex ultrasound demonstrated restoration of the normal respirophasic flow in the proximal veins of the left lower extremity (Figure 9).
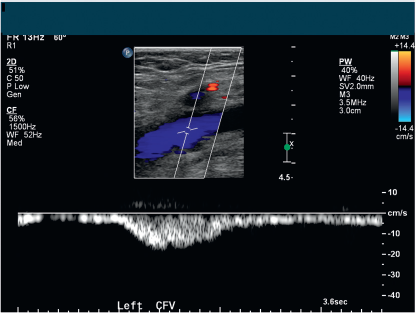
Monophasic flow within the left common femoral vein with DU.
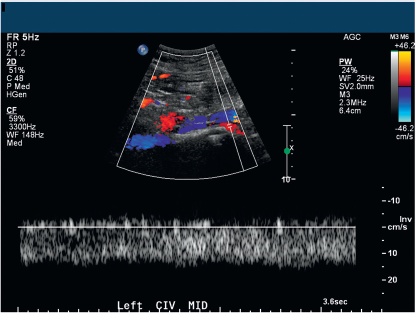
Monophasic flow just distal to iliac vein stenosis.
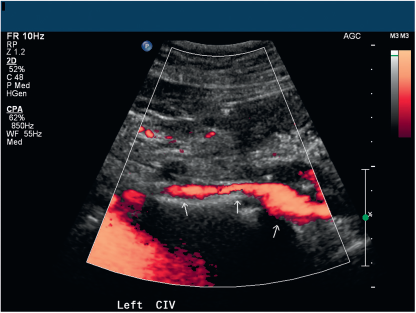
Color power angiography, noting narrowing in the vessel diameter within the stenosis.
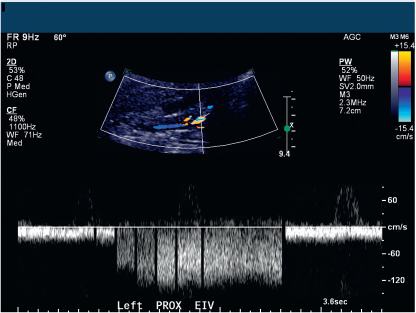
DU of the external iliac vein demonstrating a velocity shift from peak systolic velocity 32cm/sec to 150 cm/s.

Venogram performed in April 2011 that confirmed venous stenosis.

Venogram performed in September of 2011 that revealed venous stenosis and thrombus.

Flow noted within the left iliac vein post mechanical thrombectomy.

Smart stent inserted into the left iliac vein.
Follow-up venous duplex showing phasic flow within the left iliac vein.
The patient was started on anticoagulation with weight based enoxaparin. On a visit after thrombectomy and venous stent placement, the patient's lower-extremity swelling had resolved. The etiology of thrombosis was likely multifactorial and related to altered hemodynamics caused by possible radiation-induced venous stenosis and hypercoagulable state of malignancy.
Discussion
If left untreated, venous stenosis may predispose the patient to persistent lower-extremity swelling, venous thrombosis, and venous stasis ulcers. 1 There are a number of conditions that can lead to venous stenosis. Among those is May-Thurner syndrome, which is the compression of the left iliac vein between the crossing over right iliac artery and underlying vertebrae.1–3 May-Thurner anatomy is the most typical anatomic variant found with imaging during the treatment of proximal deep-vein thrombosis (DVT). 3 Intravascular ultrasound has shown that >90% of symptomatic chronic venous disease patients have this type of obstruction. 2 Patients with May-Thurner anatomy are exposed to an increased risk of left leg varicosities, venous insufficiency, and recurrent DVT. They frequently experience symptoms of postthrombotic syndrome, which consist of swelling, pain, ulceration, and venous claudication of the lower extremity during follow-up. 3 Venous stenosis may be caused by extrinsic compression from the adjacent organs, such as gravid uterus, tumors, or enlarged lymph nodes. 2 There are iatrogenic causes of venous stenosis, including long-term femoral cannulation and radiation therapy. The etiology in those cases is related to endothelial damage leading to the formation of stenosis and, in some cases, thrombosis. 4
Radiation therapy has been widely used as a concurrent treatment for many cancers. 4 Radiation-induced vascular disease may present with progressive stenosis due to the damage of the endothelium and surrounding tissues. 5 When a nonradiated vessel slowly occludes, collateral vessels distend to supply compensatory circulation.4,6 It is not known whether radiotherapy hinders collateral vessel creation, which in turn may exacerbate venous stasis and lead to thrombus formation. 4 The onset of arterial radiation-induced symptoms has been known to appear from 1 to 29 years; however, the majority of clinically symptomatic arterial stenosis is not observed earlier than 8 years postirradiation. 7
There is no conclusive evidence as to whether radiation-induced venous stenosis will follow a similar time course as that of radiation-induced arterial stenosis because of the marked difference between venous and arterial anatomy. 4 The symptoms of radiation-induced iliac vein stenosis may manifest from an asymptomatic presentation to venous congestion to extensive limb-threatening iliofemoral DVT and possible fatal pulmonary embolus. 4 The treatment of radiation-induced venous stenosis may be challenging. Because of an underlying anatomic defect and altered hemodynamics, conventional therapy with anticoagulation may not be adequate, and symptoms may reoccur. 4 Some patients may require interventional treatment. Accurate diagnosis is important to formulate an individualized treatment plan.
There are number of methods available for the detection of vein stenosis, including more traditional and relatively new diagnostic modalities. Like the other methods of investigation for venous stenosis, DU has advantages and disadvantages. Some of the anatomical locations are technically difficult to interrogate with DU and are subject to the availability of a technologist trained to perform the study. 8 It can be problematic to visualize the iliac veins in the pelvis with DU because of overlying pelvic organs and bowel gas. 1 Mussa et al. 1 noted that DU may exhibit deceiving normal spontaneous flow in the common femoral veins as the result of large collateral vessels around the site of proximal obstruction. In their studies, Hurst et al. reported false-negative scans in 5 of 18 patients with iliac vein obstruction. 10 The accuracy of the test increases with increasing degree of stenosis. 8 Labropoulos et al. 8 reported a 90% accuracy rate in diagnosing a >50% stenosis when there was a poststenotic to prestenotic peak vein velocity ratio of 2.5. They also found that poststenotic turbulence and planimetric calculations of the diameter reduction increased the diagnostic confidence but not the accuracy. 8 The study noted that some of the stenoses were present for a part of the venous cycle, as there were alterations of high and lower velocities affected by the respiration and the change in the right atrial pressure. As a result of this the affected vein was periodically compressed and decompressed. 8 The study also found that DU is a great method for following up venous interventions because restenosis, thrombosis, and reflux can be detected. 8
Conclusion
Poor flow augmentation, low-amplitude signals, which appear symmetrical in case of inferior vena cava, superior vena cava, or bilateral vein stenosis, contralateral asymmetry of the Doppler waveform in unilateral stenosis, and a mosaic color at the exit of the stenosis are good indicators of vein stenosis. 8 In the presence of any of these signs, further investigation should be undertaken to search for venous stenosis. There are multiple modalities which can be used for detection of venous stenosis. With careful investigation and technical experience, DU offers the significant advantage of being a noninvasive, inexpensive, and easily repeatable test compared with the other techniques, making it an excellent first-line method to investigate suspected venous stenosis.3,8,9