
Abstract

Introduction
Until recently, varicose vein surgery was primarily limited to an invasive surgical procedure called “ligation and stripping” of the great saphenous vein (GSV), and its tributaries. However, over the past 15 years, the field of phlebology has witnessed tremendous growth due to new technologies that are minimally invasive and can be performed in an outpatient setting. We see such a wide variety of patients from having no visible veins at all to the very tortuous and raised veins covering much of the lower extremity. Both groups usually experience similar symptoms: heavy, throbbing, and fatiguing legs. In general, patients should undergo a preoperative lower extremity Duplex exam to confirm venous insufficiency.
Protocol
A thorough review of the patient's history and current symptoms is obtained. It is very important to know if the patient has had a history of a prior DVT, is taking any anticoagulants, or hormone therapy. Inquiring about previous vein treatments is also valuable information. Once the history is completed, a standing visual exam is performed looking for signs of venous insufficiency including varicose or spider veins, skin discoloration and stasis ulcers. Our lab uses the Logic GE Notebook with a 10 MHz linear probe. The routine exam begins with the deep system to include compression, color and spectral analysis images evaluating for DVT and venous reflux. The superficial system is next examined beginning in the supine position with compression images. The GSV, anterior accessory saphenous vein (AASV), and the small saphenous vein (SSV) are routinely included. Several size measurements are taken of each vein. It is very important to review the entire length of the vein, as refluxing perforators or tributary veins may be present. Any veins that show reflux must be further evaluated with vein diameter and length of reflux noted in seconds. Reflux times that have been previously published vary according to the source. The values used in our lab are as follows:
Mild reflux: 0.5–4 s
Moderate reflux: 5–9 s
Severe reflux: greater than 10 s
For many reasons, it is helpful to use the longest sweep speed possible when testing for venous reflux (Figure 1). First, this allows one image to show augmentation, valsalva, and normal respiration.
Second, the severity of the reflux is obtained much easier even though the reflux may exceed the limit of the machine (Figure 2).
Lastly, it ensures that delayed reflux is not missed, as it often takes a few seconds for the reflux to occur.
Standing images of the superficial system should also be performed because occasionally reflux is only seen with the assistance of gravity. There are three ways to check for reflux: augmentation, proximal release and valsalva. Sometimes the reflux is more obvious with one approach over another. Also, the reflux may be so slow that it may not register with color and/or spectral analysis. In this scenario, a two-dimensional gray scale clip is beneficial so as to not miss sluggish venous reflux. Lastly and most importantly, always ask the patient if all the areas of concern were evaluated.
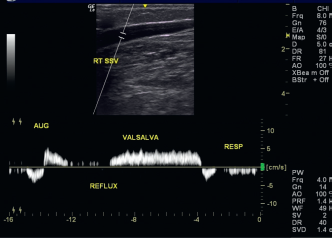
Augmentation, valsalva, and normal respiration.
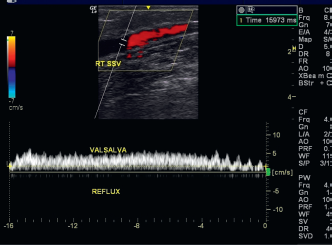
Severe reflux.
Even clusters of spider veins are evaluated for the presence of underlying refluxing reticular veins to complete a thorough exam. A worksheet with drawings is then completed notating all the necessary measurements of each vein site and duration of reflux. These measurements are important to submit for insurance preauthorization. The worksheet also provides a helpful road map on procedure day (Figure 3).
Conclusion
The bilateral lower extremity Venous Duplex exam is both timely and tedious but most often can identify the etiology of venous insufficiency causing the patient's symptoms. Even the most experienced vascular technologist will require approximately an hour evaluating the patient and documenting the results.
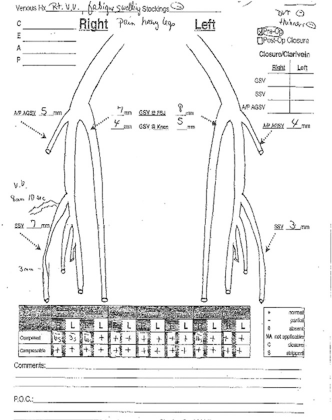
Worksheet.