
Abstract
May-Thurner syndrome, iliac vein compression syndrome, or iliocaval compression syndrome is caused by the compression of the left common iliac vein by the right common iliac artery. We report a case of MTS and the subsequent course of the findings and clinical outcome.
Introduction
May-Thurner syndrome (MTS), iliac vein compression syndrome or iliocaval compression syndrome, is caused by the compression of the left common iliac vein by the right common iliac artery.1,2 We report a case of MTS and the subsequent course of the findings and clinical outcome.
Case Report
A 24-year-old white, slightly obese female patient had a sudden onset of cramping in the left groin radiating down to the shin area. After 1 h with these symptoms, she presented to a local emergency room. She had no complaints of chest pain but was having shortness of breath. She had a temperature of 105°F. An initial duplex venous scan showed extensive deep venous thrombosis (DVT) in the left common femoral, femoral, and popliteal veins. A ventilation perfusion scan was also obtained, which was positive for pulmonary emboli (PE). She was hospitalized, admitted to the intensive care unit, and administered intravenous heparin therapy. She was discharged 6 days later on warfarin. The cause of the extensive DVT and PE were presumed to be from her recent start of oral contraceptives for irregular menses just 3 months previously.
Her medical history included asthma. Her medications included Vicodin and albuterol PRN. She denied using tobacco, alcohol, or drug abuse. Her emergency department examination did include mild left lower quadrant tenderness.
Within 24 h after discharge, she developed more extensive pain and swelling extending to her left lower leg and foot. She went to another local hospital emergency room, where she was once again admitted. She was once again started on heparin therapy. A second venous duplex scan was performed, which documented her extensive left lower-extremity (LLE) DVT. During her second hospital course she had further evaluation, which included a chest computed topography, which confirmed multiple bilateral PE, right greater than left, but no main pulmonary artery emboli. The patient also underwent an abdominal and pelvic computed tomography with contrast. This showed extensive clot formation involving the left common iliac vein (Figures 1–3).
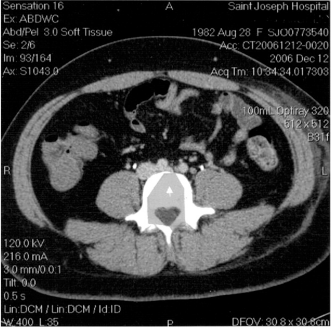
Left common iliac vein (small arrow) compressed by right common iliac artery.
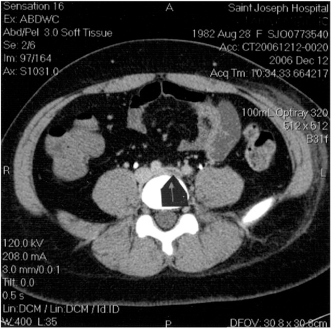
Filling defect within left common iliac vein (arrow) just distal to compression.
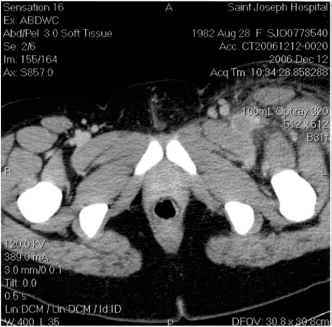
Large clot more distally in left common femoral vein.
Consultations were obtained with a hematologist, pulmonary specialist, and a vascular surgeon. Given the extent of the thrombus in the LLE, consideration was given for thrombolysis and/or placement of an inferior vena cava (IVC) filter. Upon review of the computed tomography findings, the vascular surgeon concluded that the findings were more indicative of May-Thurner syndrome.
Because of the patient's history of multiple bilateral PE, absence of phlegmasia alba, or cerulea dolens, the vascular surgeon did not consider the patient a candidate for thrombolysis. An IVC filter was not inserted because she appeared to be stable on her anticoagulation without further emboli. Temporary IVC filters were not clinically available at the time of her presentation. She was discharged 6 days later and advised to continue anticoagulant therapy and start compression stockings.
At her 3-month follow-up the venous duplex scan demonstrated resolving DVT. The extremity was still edematous, with patient stating she had moderate pain and discomfort. At her 6-month follow-up venous examination, the duplex scan demonstrated minimal residual thrombus in the left common femoral vein and femoral vein as well. This study noted a significant improvement from her previous exam.
At her last physician's office visit, the patient was free of pain with faint edema in the LLE. She has no manifestations of chronic venous hypertension with no inflammation and no hemosiderin-laden deposits. She maintained a daily dose of warfarin 5 mg daily.
Discussion
Reviewing previous published articles, medical journals, and vascular textbooks, we have found there appears to be rare documentation of this interesting phenomenon. In 1957, May and Thurner examined 430 cadavers that appeared to have iliac compression syndrome and documented the impedance in venous flow that resulted from intimal changes. They hypothesized that these changes were acquired from compression of the left common iliac vein by the right common iliac artery, with the transmitted arterial pulsation causing the two walls of the vein to rub against each other leading to irritation of the endothelium. Over time, this irritation led to proliferation of the endothelium and formation of a partition of the lumen.
This condition has been estimated to occur in 2–5% of patients who are evaluated for lower-extremity venous disorders. Symptoms include leg swelling, varicosities, DVT, and chronic venous stasis ulcers and could develop into pulmonary embolus or phlegmasia cerulea dolens. 3
It is important to recognize the persistent edema of the left leg, especially in women between the ages of 20–40 years of age who may or may not be diagnosed with DVT. MTS is a progressive disease with long-term complications.
Recurrence of Disease
As many as 60% of patients with MTS are predicted to have postthrombotic syndrome (edema, pain, stasis dermatitis, ulcers, or cellulitis) at some time during their lives. 4 Catheter-directed thrombolysis with tissue plasminogen activator or urokinase appears to reduce the risk of postthrombotic syndrome by one half over 12 months compared with conventional anticoagulation with warfarin (66% versus 33%, respectively). Stenting also has better outcomes than anticoagulation, with 87% vessel patency and symptom recurrence of only 20% at 41 months of follow-up. 5
Conclusion
As vascular technologists, the primary reason or cause for a venous duplex examination request is to rule out the diagnosis of DVT. If continuous, nonphasic venous Doppler flow velocities are encountered in the common femoral vein without evidence of DVT, further investigation of the external iliac vein and common iliac vein would assist in a clinical diagnosis. As vascular ultrasound technologists, we should be cognizant of this rare disorder to better serve our patient population.