
Abstract
Patients with dialysis access steal phenomenon can present with pain, paresthesia, ulceration, and tissue loss of the digits. Some degree of steal is common, up to 80% of patients with a radiocephalic arteriovenous fistula have mild, asymptomatic arterial steal documented by a decreased digital blood pressure. Critical ischemia of the upper extremity is a rare condition compared with ischemia of the lower extremities. High-flow arteriovenous fistulas have a greater risk of steal than normal flow arteriovenous fistulas; however, combined with arteriosclerotic disease they may also lead to ischemia. There are several strategies to prevent arterial steal following hemodialysis access that should be used; preoperative testing to identify proximal arterial lesions, upper extremity vein mapping and sizing, Allen's test (radial artery patency), end-to-side arteriovenous anastomosis to decrease steal and distal venous hypertension, selective venous arterialization at the elbow with ligation of deep perforation branch to improve maturation and restrict flow, and stepped or tapered grafts to limit flow. A noninvasive upper extremity arterial Doppler diagnosis is of importance to determine treatment options for patients. The goal of the vascular access surgeon is to promptly recognize and treat the disorder to maximize both limb and access salvage.
Introduction
Dialysis access steal syndrome is a common complication for patients on dialysis. Digital pressures are useful in evaluation of dialysis access steal. 1 Dialysis access steal syndrome can lead to digital ischemia. 2 Severe dialysis access steal can develop immediately following the procedure. 3 There is also a possibility of inflow stenosis post procedure and patients are sometimes referred to interventional nephrology for angioplasty as needed. 4 There are four states of dialysis access steal syndrome. 5 An ischemic hand is a serious complication. 6 In the United States 180 people per million are treated for end-stage renal disease. 7 Dialysis access digital ischemia affects 4% of patients. 8 Treatment options such as distal revascularization-interval ligation (DRIL) have been performed on patients who have severe distal ischemia. 9
Methods
Multiple patients underwent upper extremity arterial Doppler examinations to rule out significant dialysis access-associated steal syndrome (DASS) (Table 1). Dialysis access steal syndrome distal to an arteriovenous fistula remains a clinical problem. 10 Ischemia of the upper extremities is a rare condition compared to the lower extremities. 11 The patients were evaluated with and without compression of the AV fistula. The purpose of the noninvasive exam was to determine the severity of the DASS. The arterial studies included digital-brachial indices on all digits with and without AV fistula compression.
Upper Extremity Arterial Doppler—Dialysis Access Steal Syndrome: Severity Criteria
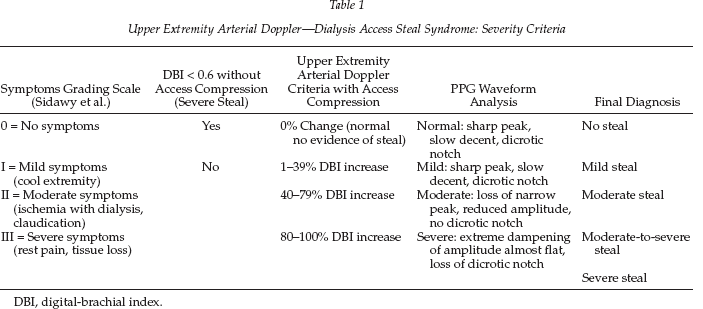
DBI, digital-brachial index.
Results
A total of 21 patients were diagnosed with DASS. The patients were all noted to be symptomatic. The patient symptoms ranged from mild symptoms to severe symptoms (i.e., tissue loss). On noninvasive access evaluation, the following was determined in the 21 patients: 19% of patients were diagnosed with a mild steal; 24% of patients were diagnosed with a moderate steal; 24% of patients were diagnosed with a moderate-to-severe steal; 29% of patients were diagnosed with a severe steal. The patient results were based on symptoms, arterial waveform analysis, and digit-brachial indices on all digits with and without fistula compression. The following diagnostic criteria were determined: a patient with Grade I (mild; Sidawy et al.) steal symptoms combined with a digital-brachial index (DBI) that increased with fistula compression 1–39%, accompanied by mild waveform changes (i.e., sharp peak, slow decent, diacrotic notch) is considered to have a mild steal; a patient with Grade II (moderate; Sidawy et al.) steal symptoms combined with a DBI that increased with fistula compression 40–79%, accompanied by moderate waveform changes (i.e., loss of narrow peak, amplitude reduced, no dicrotic notch) is considered to have a moderate steal. If the patient has Grade II (moderate; Sideway et al.) symptoms, a DBI that is less than 0.6 without compression of the fistula, and has a DBI that increased 40–79% with compression of the fistula, the patient is considered to have a moderate-to-severe steal; a patient with Grade III (severe; Sidawy et al.) steal symptoms, a DBI that increased with fistula compression 80–100%, accompanied by severe waveform changes (i.e., extreme dampening of waveform amplitude, almost flat, no dicrotic notch) is considered to have a severe steal. To make an accurate diagnosis for DASS, all of the above must be taken into consideration. Accurate DASS diagnosis is crucial to have a successful outcome for the patient.
Conclusions
Upper extremity arterial Doppler examinations were performed on patients who showed symptoms of DASS. Multiple patients were reviewed and based on patient symptoms, DBI, and digital waveform analysis, we were able to determine the actual severity of dialysis access steals.