
Abstract
Vascular complications associated with orthopedic procedures, though rare, pose the potential for permanent disability or limb loss. Thermal, mechanical, and vibratory forces incurred during total knee arthroplasty may traumatize the popliteal artery leading to thrombosis, laceration, dissection, arteriovenous fistula, or pseudoaneurysm formation. Color duplex ultrasound (8 MHz), followed by digital subtraction angiography promptly diagnosed a large left popliteal artery pseudoaneurysm. Definitive surgical intervention via a posterior approach permitted direct arterial repair, venous decompression, and tibial neurolysis. There were no neurovascular sequelae. Adherence to both preoperative vascular assessment and meticulous surgical technique are crucial to mitigate against this potentially catastrophic injury.
Case
A morbidly obese [body mass index (BMI) 39.8] 53-year-old gentleman underwent an uneventful left total knee arthroplasty under pneumatic tourniquet for severe osteoarthritis. Within 2 weeks, he began to experience progressive dysesthetic pains and peripheral lymphedema despite a regimen of systemic anticoagulation with Coumadin. Color duplex ultrasound examination revealed a 5.2 × 3.5 cm left popliteal pseudoaneurysm in transverse view, and to and fro flow in the sagittal view (Figure 1). Clinical examination noted only left monophasic peroneal and posterior tibial arterial signals, whereas the contralateral extremity exhibited +1 palpable dorsalis pedis and posterior tibial arterial pulses. Digital subtraction angiography revealed an isolated, bilobed, left popliteal pseudoaneurysm with myriad feeding collaterals and stagnant infrapopliteal flow due to a “steal” effect within the aneurysm (Figures 2 and 3). Preoperatively, a retrievable Denali IVC filter (Bard, Inc., Murray Hill, NJ) was temporarily implanted and subsequently removed 3 months postoperatively given the patient's high risk of perioperative thrombotic complications. A pneumatic tourniquet was placed on the left thigh prior to the prone positioning necessary for surgical repair via a posterior “lazy S” incision. Intermittent tourniquet inflations allowed for hemostasis and avoidance of vascular clamp injury during primary ligation of collaterals and repair of the popliteal artery, coupled with decompression of the popliteal vein and neurolysis of the tibial nerve. Postoperatively, the patient immediately regained palpable posterior tibial and dorsalis pedis pulses. On the third hospital day, the patient was discharged. Post operative color duplex ultrasound certified normal arterial and venous flow dynamics. The dysesthetic leg pains and peripheral lymphedema resolved within 2 months, after which the patient returned to full work capacity.
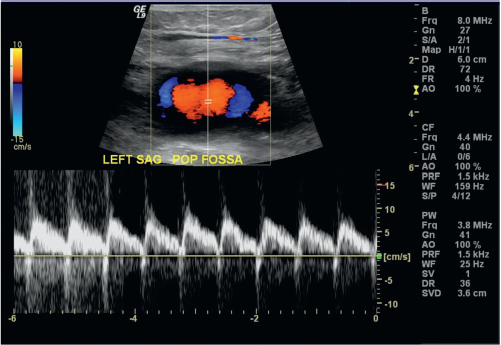
Duplex scan of to and fro flow in the pseudoaneurysm.

Knee prosthesis with multiple collaterals seen around pseudoaneurysm.
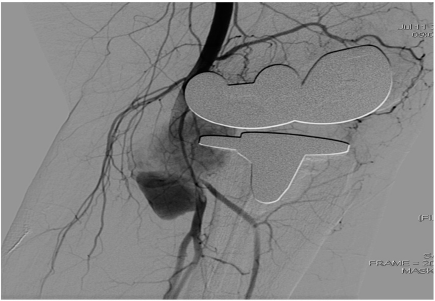
Filling of pseudoaneurysm compressing the popliteal vein and nerve complex.
Discussion
The incidence of popliteal arterial injuries following orthopedic knee operations is exceedingly low (0.005–0.08%).1,2 Nevertheless, the consequences of delayed diagnosis heighten risk of permanent disability and amputation. Treatment of popliteal injuries varies from endovascular intervention to open primary repair or bypass.3–5 Presentation may be as sudden as brisk hemorrhage following decompression of the pneumatic tourniquet or manifest later as deep vein thrombosis, peripheral edema, neuropathic pain, claudication, or limb ischemia. Both the orthopedic and vascular surgical literature address the risk of arterial injury and suggest that certain patient risk factors heighten potential injury: peripheral vascular disease vis-a-vis nonpalpable pulses, African–Americans, and reoperative knee operations.1,6 Atherosclerotic medical comorbidities such as diabetes, obesity, and cicatricial tissue associated with obliterated surgical tissue planes explain these tendencies, respectively. The literature also notes the potential that a tourniquet may induce injury to calcified vessels or previously bypassed extremities.1,2,7,8
Anatomic relation of the popliteal artery to the tibial plateau is shown by both cadaveric and in vivo studies that demonstrate the posterior displacement of the popliteal artery from the tibial shaft during 90-degree flexion. 9 However, the potential exists for the distal popliteal artery and its geniculate and sural branches to tether the proximal segment during knee flexion. A resultant hematoma or, in this case, a pseudoaneurysm may then develop. 10 The constellation of claudication, neuropathic pain, and peripheral lymphedema reflects elevated compartmental pressures within the popliteal fossa: the bilobed dimension of the aneurysm allowed for blood pooling, while simultaneously compressing both the popliteal vein and tibial nerve. Arterial duplex was critical in securing the diagnosis of popliteal artery injury with resultant pseudoaneurysm formation. Angiography confirmed a traumatic pseudoaneurysm, not true aneurysm; a causal link to total knee arthroplasty was further enhanced by noting neither a contralateral popliteal aneurysm, nor aortic aneurysm. The geniculate feeding vessels to the left popliteal pseudoaneurysm did not preclude endovascular repair. However, the signs and symptoms of peripheral 2 + lymphedema and tibial neuropathy mandated an open approach to not only repair the popliteal artery, but also decompress both popliteal vein and tibial nerve.
The aging population and those patients with a BMI >30 will continue to pose a serious challenge to resolve their symptomatic osteoarthritis, while limiting perioperative complications. Critical to successful limb preservation is high index of suspicion and, hence early diagnosis with an initial arterial duplex study, followed by angiography and intervention. The high frequency of peripheral vascular disease in these populations mandates preoperative vascular assessment either by performing ankle-brachial indices or vascular surgical referral to mitigate the consequences of arterial injury.