
Abstract
Objective
—Ulnar nerve compression, the Guyon's canal syndrome, is more unusual than carpal tunnel disorders. An exceptional case of a patient with vascular and neurogenic signs and symptoms is described.
Patient Presentation
—A 26-year-old female physiotherapist presented with neurogenic and arteriovenous signs and symptoms involving the right hand. The patient described fourth finger and wrist pain with flexion, and pain and itching extending to arm and forearm. Sensations worsened when exposed to air conditioning. Enlarged vessels were noted in the medial aspect of the fourth digit; trauma occurred 8 years earlier during attempts to open a nail polish container.
Methods
—Color flow, duplex-Doppler ultrasonography (US) of the subclavian to digital vessels was performed using 3- to 13-MHz transducers. Interpretation focused on flow waveforms obtained with the hand open and closed, having the left extremity as reference. Thermography was performed with camera Flir 15, room temperature at 21°C (70°F) and relative humidity at 48%.
Results
—Right subclavian to digital arteries had high diastolic flow with opened hand. Hand closure interrupted diastolic flow except in the ulnar circulation to the fourth digit. Common digital arteries feeding digits 3–4 and 4–5 had significantly more diastolic flow than the artery feeding digits 2–3. Diastolic flow through a dilated ulnar artery despite hand closure was associated to a millimetric arteriovenous fistula in the fourth finger. Hyperthermia saturating at 35°C (95°F) showed channel-like images over the ulnar nerve and artery and fourth digit, compared with 20°C (68°F) for digit 2.
Conclusions
—US and thermography demonstrated high flow and hyperthermia associated with a fourth digit fistula and abnormal vessels, and ulnar artery dilatation likely associated with ulnar nerve injury. A coadjuvant diagnosis of Guyon's canal syndrome at the wrist was raised.
Introduction
A patient with arteriovenous and neurologic signs and symptoms, primarily in the right hand, was directed to the noninvasive vascular laboratory. Most common suspicion was a carpal tunnel nerve compression syndrome and/or ulnar nerve compression at the elbow. Vascular lesions (Figure 1) and neurologic presentation also suggested an ulnar compression syndrome at the wrist, historically referred to as the Guyon channel. 1
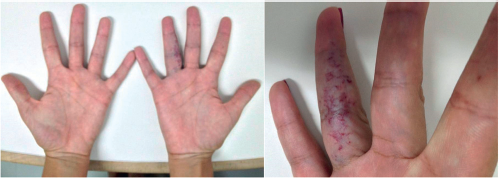
Patient with vascular and neurogenic signs and symptoms relatable to a compression syndrome.
Signs and symptoms of neural compression in the upper extremities can be specific or not, or related to coexisting pathologies as ulnar or carpal tunnel compression syndrome, thoracic outlet compression syndrome, C8-T1 radiculopathies, or peripheral neuropathies. Carpal tunnel compression syndrome is common among peripheral nerves, with a prevalence estimated in 4% 2 ; its surgical treatment is 10 times more frequent 3 than surgical treatment of the ulnar nerve at the elbow. 4
Ulnar nerve compression syndrome at the wrist is rarer than carpal tunnel or ulnar compression at the elbow.5,6 Idiopathic and traumatic causes would be most common 7 ; cysts and ganglia would be primary alternatives,8,9 following anomalous muscles or tendons,10,11 periarthritis, 12 and tumors as lipomas13–15 and giant cell tumor. 16 Occupational or traumatic hyperactivity can cause neurovascular syndromes in the Guyon channel.17–24
Doppler ultrasonography (US) has been recommended as the method to differentiate hypothenar hammer syndrome versus a more general syndrome caused by arm, forearm, and hand vibration. 25 A vascular cause for an ulnar syndrome is rare. 26 Trauma can cause ulnar vein or artery thrombosis and digital embolization17,27–29; trauma can also cause aneurysms that, when detected, could be partially thrombosed and a potential risk for distal embolism.27,30,31 Ultrasonographic imaging is an effective method to detect true or false aneurysms.32,33 Other vascular causes include arteriovenous malformation, 34 hemangioma, 35 leiomyoma, 36 and tortuous ulnar artery. 37
US, electroneuromyography, computerized tomography, and magnetic resonance contribute to diagnosis. US presents advantages regarding vascular diagnostic,25,38 particularly in cases of ulnar artery occlusion.39,40
Thermography has been used to evaluate carpal tunnel syndrome, 41 Raynaud's phenomenon 42 and arm-forearm-hand vibration syndrome. 43
We describe an exceptional case of a patient with arteriovenous fistula and malformation, ulnar nerve compression syndrome, and suspicion of even more complex pathologies. The exams performed in the noninvasive vascular laboratory included both upper extremities. Vascular alterations were detected with duplex-Doppler US and color-flow imaging. Thermo-related abnormalities originated from neurologic, inflammatory, and/or even vascular pathologies were investigated using thermography.
Case Report
Patient history, physical examination information, methods used in the noninvasive vascular laboratory—US and thermography—results of such examinations, and discussion are reported herein.
Clinical Information
A 26-year-old woman, physiotherapist, nulliparous, no abortion, user of hormonal contraceptive for the last 7 years, related pain and discomfort in the right wrist and fourth digit during flexion movements. The patient also mentioned constant petechiae, pain, numbness, and itching in the right upper extremity. Such conditions got worse when exposed to air-conditioning, e.g., in the car. Vascular lesions (Figure 1) were perceived ≈8 years ago following apparent trauma while trying to open a tightly closed nail-enamel container.
Physical examination revealed vascular lesions in the fourth finger: blue and red vessels, with localized vasodilatations. Bruits were not detected by auscultation or palpation. Axillary, brachial, radial, and ulnar arteries were palpable bilaterally, showing no apparent alterations. Manual pressure exertion was maintained bilaterally but the patient complained of pain in the right forearm. Sensation was adequately present in both upper extremities. Percussion of the right carpal tunnel and distal ulnar epiphysis radiated to the forearm and third, fourth, and fifth digits.
Laboratory exams did not show significant alterations regarding collagenous diseases. Electroneuromyography and imaging examinations were not performed prior to the vascular laboratory visit. As an addendum, the patient showed psychological reluctance to face her disorders both clinically and medically.
Vascular US
Methods
Axillary, brachial, radial, ulnar, palmar, and digital arteries were evaluated bilaterally using duplex-Doppler US and color-flow imaging. The equipment used was a GE Vivid S5 (General Electric, Milwaukee, WI); transducer frequencies were 3–13 MHz.
Arterial flow detection was performed with the patient supine and hands open or closed. Flow data from the abnormal right upper extremity were compared with flow data from the contralateral left extremity used as reference. The main interpretation focused on flow waveform analysis.
Results
Figure 2 compares flow waveforms from the right and left radial arteries. Such waveforms also represented similar responses obtained at the subclavian, axillary, and brachial arteries of the corresponding extremities. Figure 3 shows flow waveforms obtained from the right and left ulnar arteries. Figure 4 shows flow waveforms obtained from digital arteries and arteriovenous fistulas of the fourth digit in the right hand.

Color-flow and duplex-Doppler-flow waveforms from the right and left radial arteries of a patient with neurovascular symptoms primarily in the right hand. Elevated diastolic flow through the right radial artery, representing subclavian artery to radial flow, was interrupted with hand closure. Arteria Radial, radial artery waveforms; Mão Aberta, open hand; Mão Fechada, closed hand; Direita, right; Esquerda, left. Note: Images were altered to show similar 1 cm depths in the right and left hand comparisons.
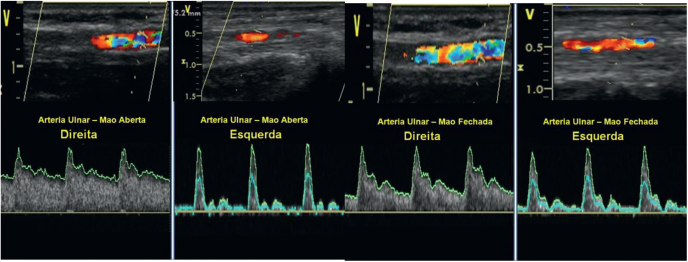
Color-flow and duplex-Doppler-flow waveforms from the right and left ulnar arteries of a patient with neurovascular symptoms primarily in the right hand. Elevated diastolic flow through the right ulnar artery was not interrupted with hand closure. Arteria Ulnar, ulnar artery waveforms; Mão Aberta, open hand; Mão Fechada, closed hand; Direita, right; Esquerda, left. Note: Images were altered to show similar 1 cm depths in the right and left hand comparisons. Observation: Ulnar artery diameter is significantly larger on the right than on the left upper extremity.
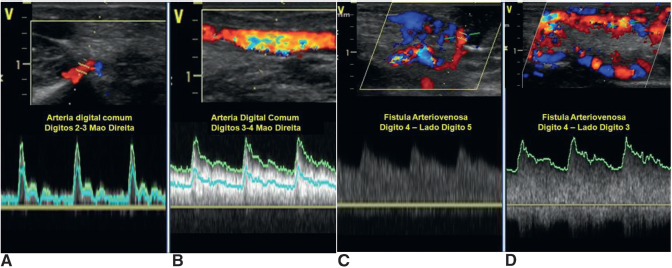
Color-flow and duplex-Doppler waveforms from right hand digital arteries of a patient with neurovascular symptoms primarily in the right hand. Common digital artery (Arteria digital comum) toward (A) second and third digits, (B) third and fourth digits. Mão Direita, right hand. Arteriovenous fistula (Fistula Arteriovenosa) in the fourth digit (C) transverse image in color and (D) longitudinal image in color. Lado 5, fifth digit side; Lado 3; third digit side.
Interpretation
Flow waveforms from the right upper extremity demonstrated vasodilation with open hand. Hand closure increased peripheral resistance to radial, brachial, axillary, and subclavian flow. Uninterrupted ulnar diastolic flow with hand closure, however, suggested arteriovenous malformation even in the region proximal to the digits. Nonocclusion of fistula or fistulas noted in the fourth digit could also be contributory to maintenance of high diastolic flow in the ulnar artery despite hand closure. Figure 4 demonstrated digital fistulas.
In contrast, flow waveforms from the left upper extremity showed no significant vasodilatation under the same environmental conditions.
Thermography
Methods
Arm, forearm, and hand thermography was performed with the patient sitting and hands extended over a table. The room temperature was set at 21°C (70°F) and the relative humidity was 48%. An infrared camera Flir I5 (Flir Systems, Inc., Wilsonville, OR) was used. Images were obtained from about 1 m distance. Temperature scale and pattern were set automatically. Artificial colorization was selected to optimize the operating physician visual preferences. Thermographic data from the right upper extremity were compared with data from the left as reference.
Results
Figure 5 shows the temperature mappings comparing right and left forearms and hands. Figure 6 shows details of the relative hyperthermia (hyperreactivity is a term improperly used) detected at the right forearm and hand.
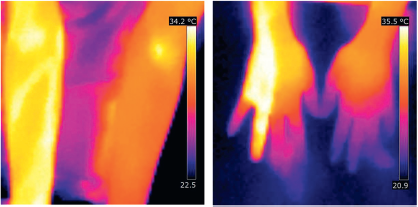
Bilateral forearm and hand thermography of a patient with neurovascular symptoms primarily in the right hand. Forearm scale from 22.5°C to 34.2°C (72.5°F to 93.6°F) indicated saturation at the maximum temperature in forearm regions corresponding to ulnar artery and nerve. Hand scale from 20.9°C to 35.5°C (69.6 to 95.9°F) indicated saturation at the maximum temperature associated to the arteriovenous fistula(s) and to the ulnar nerve. In contrast, digital temperatures not affected by fistulas were about 20°C (68°F).
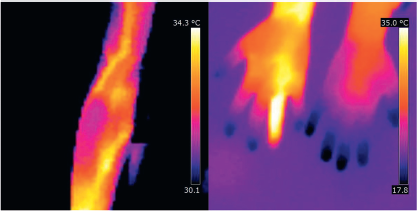
Right arm-forearm and bilateral hand thermography of a patient with neurovascular symptoms primarily in the right hand. Right arm scale from 30.1°C to 34.3°C (86.2°F to 93.7°F) indicated saturation at the maximum temperature in arm and forearm regions related to brachial and ulnar arteries and corresponding nerves. Hand scale from 17.8°C to 35.0°C (64.0°F to 95.0°F) indicated saturation at the maximum temperature associated to the arteriovenous fistula(s) and to the ulnar nerve. In contrast, digital temperatures not affected by fistulas were about 18°C (64.4°F) or even colder, particularly in the digits of the left, normal hand.
Interpretation
Relative hyperthermia (the term hyper reactivity, with a dubious meaning, is used by some) was demonstrated in axial regions associated to the brachial and ulnar arteries, corresponding nerves, and to the fourth digit of the right upper extremity. Hyperthermia was also related to a medial nerve or even artery. The radial artery region did not present temperature changes as drastic as the ones presented by the ulnar artery. Right wrist thermography, however, showed radial hyperthermia relative to the corresponding site of the left wrist. An apparent relative hypothermia was noted in the digits not affected by the arteriovenous fistulas or even malformation.
Discussion
This case report describes a rare thermovascular condition of an upper extremity. Vascular US demonstrated primarily arteriovenous fistula or fistulas in the fourth digit of the right hand affecting flow even to the level of the subclavian vein. Duplex-Doppler demonstrated significant differences between the right ulnar artery and the other arteries at both wrists. Right hand closure interrupted radial flow but ulnar flow continued to have a high end-diastolic component. Such diastolic flow was attributed to arteriovenous fistulas and potential malformation in the fourth digit and surrounding region. The main fistula could be associated with trauma described by the patient.
US imaging also demonstrated significant large diameter of the right ulnar artery (Figure 3) and some enlargement of the right radial artery (Figure 2). Such ulnar artery enlargement may cause a neural compression.
Thermography showed results compatible with diastolic flow through the right ulnar artery and its feeding arteries. Temperature differences among right and left wrist were also shown. Besides high fistula flow, one must consider the possibility of neural compression and inflammation as direct or indirect contributories to the hyperthermia.
The literature already mentioned trauma and arteriovenous malformation to ulnar nerve compression syndrome.5,6,17–24,26,34,35 Occupational trauma has to be considered in a physiotherapist. Positional pain and discomfort, itching, and numbness, described by the patient, are compatible with neural compression.
A possible cause of ulnar nerve compression in the Guyon channel would be the increase in diameter of the ulnar artery at the wrist. Such ulnar artery dilatation would be in response to the high flow of the fistulas and/or possible malformation. This increase in diameter would not be aneurysmatic but could have similar influence as cause of neural compression.27,30–33
Thermography also suggested relative hypothermia at the tip of several digits. Lower temperatures were noted in the digits of the left and right hands not associated to the fistulas of the fourth finger. Such finding is compatible with the patient history describing her feelings when exposed to air-conditioning. Raynaud's disease or phenomenon could be another entity, not necessarily as differential but as a complementary diagnosis. 42
Additional examinations, especially electrodiagnosis of neural behavior, are dependent on the patient's points of view and emotional conditions.
Conclusion
Physiotherapist with history of neurovascular signs and symptoms, mainly related to the right hand and also when exposed to the cold of an air-conditioning, was examined in the noninvasive vascular laboratory. Doppler and imaging US demonstrated pathologic diastolic flow in the right ulnar artery associated to arteriovenous connections in the fourth digit; dilated ulnar diameter could be causing nerve compression at the Guyon channel. Thermography demonstrated relative hyperthermia related to ulnar artery flow from the brachial artery to the digit with fistulas and to adjacent nerves. Thermography also demonstrated digital hypothermia in digits of both hands.
Fistulas, vascular malformations, and Raynaud's and Guyon's canal syndrome have been exposed by the US and thermographic data. US and thermography should be combined to provide significant information to clarify a mixed and complex condition.