
Abstract
Intraoperative transcranial Doppler (TCD) monitoring allows us to see intracranial blood flow changes related to endovascular and surgical manipulation in real time. This study evaluates the results of TCD monitoring during transcarotid artery revascularization (TCAR) with flow reversal, carotid endarterectomy (CEA) without shunt, with a shunt (shCEA), and transfemoral carotid artery stenting (tfCAS) with distal filter protection. Patients who underwent carotid artery revascularization with TCD monitoring were included. Patient demographics and medical history were recorded based on medical documentation. Intraoperative TCD, hemodynamics, fluoroscopy images, and surgical manipulation were recorded simultaneously with a 4-channel video recording system, and based on the recordings, the number of high-intensity signals (HITS) and middle cerebral artery (MCA) flow changes were registered. HITS during contrast injections were not included in the analysis due to the high number of artifacts. HITS were compared between the four groups, and HITS during lesion crossing/predilation/stent deployment/postdilation were compared between the tfCAS and TCAR groups. Thirty six patients were involved (mean age 69.5 ± 10.59 years; 24 male) (9 CEA; 11 shCEA; 4 tfCAS; 12 TCAR). Hypertension, diabetes mellitus, coronary artery disease, and smoking were frequent in all groups. Median number of HITS for CEA, shCEA, tfCAS, and TCAR were 5 (range: 0-90), 10 (range: 3-72), 197.5 (range: 153-340), and 29 (range: 2-74), respectively. The number of HITS during TCAR was not significantly different compared to CEA or shCEA but significantly lower than in patients receiving tfCAS (P < .01). Procedural phases of lesion crossing, predilation, stent deployment, and postdilation were associated with significantly higher HITS during tfCAS than TCAR (P = .002, P = .006, P = .04, P = .006, respectively). The number of embolic events during TCAR is comparable with CEA with and without a shunt and associated with a significantly lower HITS rate than tfCAS with distal filter protection. According to our results, TCAR appears to be a safer alternative to tfCAS.
Introduction
Transcranial Doppler (TCD) is a noninvasive, cost-effective, and reliable technique; it provides accurate and real-time information on cerebral hemodynamics and embolic events in the cerebral vessels without the use of radioactive substances.1,2 Carotid artery disease (CAD) can potentially lead to ischemic stroke, a catastrophic complication of the disease. Up to 30% of ischemic strokes are associated with CAD due to plaque rupture and cholesterol embolism.3-5 Current operative treatment options for CAD include open carotid endarterectomy (CEA) or carotid artery stenting (CAS). Extensive clinical trials showed that CEA is associated with lower stroke risk; CAS remains an alternative option of carotid artery revascularization in selected patient groups. 6 Embolic protection systems have been developed and are used to prevent intraprocedural cerebral embolization. While distal filter protection catches debris during transfemoral carotid artery stenting (tfCAS), transcarotid artery revascularization (TCAR) prevents distal embolization by avoiding endovascular manipulation in the aortic arch and flow reversal during the procedure.
Recent studies have revealed that TCAR is associated with lower cerebral embolization rates than tfCAS.7,8 The amount of silent ischemic postoperative lesions found on diffusion-weighted magnetic resonance imaging (MRI) after TCAR is equivalent to that after CEA but significantly less than tfCAS.9,10 Therefore, TCAR seems to be a more appropriate alternative to CEA among the high-risk surgical patient population.
Although postoperative clinical outcomes and imaging results are well established, our knowledge of real-time, intraoperative cerebral flow changes, and embolization patterns during different procedural phases are limited. This study aims to evaluate the results of TCD monitoring during TCAR with flow reversal, CEA without shunt, with shunt (shCEA), and tfCAS with distal filter protection.
Methods
Patient Inclusion and Study Design
This is a retrospectively designed study. The patients included in the study are those who underwent CEA, shCEA, tfCAS, and TCAR, all with TCD monitoring. Patients who did not have a sufficient temporal window for obtaining the appropriate TCD signal were excluded. The CEA, shCEA, and TCAR groups were included with consecutive patients between September 2017 and December 2019. Previously published data were used for patients in the tfCAS group. 11 The selection of interventions for all groups was assessed and was consistent with the most current guidelines.
Hospital electronic medical records were reviewed for demographic data, past medical history, presentation to our center, perioperative imaging, and postoperative outcomes for all patients. Intraoperative data were collected from a 4-channel live case recording (Figure 1), which included live fluoroscopy images, 3-dimensional (3D) reconstructed computed tomography angiography images, vital parameters, and TCD. Separate intraprocedural phases were analyzed for each of the procedures. For tfCAS and TCAR, the phases were lesion crossing, predilation, postdilation, and removal of devices. For shCEA and CEA, vessel isolation, clamping, shunt-placement (only shCEA), endarterectomy, clamp removal, revision, and closing were defined as phases.

Four-channel live case recording.
Primary endpoints were total procedural high-intensity signals (HITS) numbers and the number of HITS in different phases of the procedures. Secondary endpoints were in-hospital mortality, neurological events, re-intervention, and significant adverse events, including bleeding, myocardial infarction and cardiac arrest that required cardiopulmonary resuscitation. The institutional review board approved this study.
Carotid Revascularization Techniques
Transcarotid artery revascularization
The technique of TCAR has been previously described.12,13 Briefly, the proximal common carotid artery (CCA) is exposed through a small transverse incision at the base of the neck. After gaining vascular access at the CCA, a carotid angiogram is performed. The ENROUTE sheath (Silk Road Medical, Sunnyvale, CA) is placed in the CCA over the wire. An 8 Fr sheath is inserted percutaneously in the common femoral vein, which provides passive reversal of the blood flow from the carotid artery through a circuit and filters the blood. Once the CCA is clamped proximal to the sheath, flow reversal is introduced. After crossing the lesion with a wire, predilation is performed with a 3 to 4 mm balloon catheter. The lesion is stented with a self-expanding system and finally postdilated with a 4 to 6 mm balloon catheter. The decision to predilate or postdilate is left to the operator’s discretion.
Transfemoral carotid artery stenting
The CCA was catheterized from femoral arterial access. Selective angiography was performed to visualize the target lesion. After achieving optimal visualization of the lesion, FilterWire EZ System (Boston Scientific, Santa Clara, Calif) was deployed in the distal internal carotid artery (ICA). As per the conventional CAS technique, predilation was performed with a 3 to 5 mm diameter balloon catheter after advancing the wire. A self-expanding stent (NexStent Carotid Stent; Boston Scientific, Santa Clara, Calif) was used, and postdilatation was performed in all cases.
Carotid endarterectomy
Open endarterectomy with a bovine pericardial patch closure was performed. The use of a shunt was decided intraoperatively based on the ipsilateral middle cerebral artery (MCA) mean flow velocity in TCD. If a 50% or more drop in mean flow velocity relative to the baseline was noticed after clamping the carotid artery, a shunt was introduced.
Anesthesia and Anticoagulation
All interventions were performed under general anesthesia with standard anesthetic monitoring, including noninvasive blood pressure monitoring, continuous electrocardiogram, end-tidal CO2, and pulse oximetry. Bivalirudin was used for all carotid artery patients intraoperatively. A bolus dose of 0.75 mg/kg bivalirudin accompanied by a continuous infusion of 1.75 mg/kg/hr for the intervention duration was used as a standard protocol. Activated clotting times were followed, and all remained in the therapeutic range without additional boluses being required. Patients who had no contraindication were given Plavix 75 mg three days before the procedure for the TCAR and tfCAS groups. All patients received Plavix 75 mg for one month postoperatively.
TCD Monitoring
Preoperatively, all patients underwent a complete TCD examination (power-mode Doppler, Spencer Technologies PMD-100) to assess intracranial flow status and the presence of concomitant intracranial stenosis. A 2 MHz transducer with a 13-mm circular probe surface was used to insonate the ipsilateral MCA. A commercially accessible probe-holding head frame device (Marc 600 series; Spencer Technology, Seattle, Wash) was utilized to sustain the temporal bone window imaging. PMD-100 software settings were 2 MHz transducer, 13 mm circular probe surface, 125-175 Hz filter, 80% to 100% output power, 4 dB Doppler volume, 8 kHz pulse repetition frequency, 0 to 3 dB noise, 128 points fast Fourier transformation, 66% overlap, 9 mm sample volume axial length, and 30 dB M-mode range.
During the entire procedure, the ipsilateral MCA was monitored for cerebral flow status and HITS detection. Several TCD parameters were recorded and evaluated during the initial, final, and procedural steps (as described above). The mean flow velocity of the MCA, pulsatility index of the MCA, and HITS count for all phases were also analyzed. The number of HITS was counted by two observers independently to ensure accuracy and reliability during each of the procedural phases. Phases with emboli counts were evaluated and recounted by viewing the recording. Consensus committee guidelines were used for the calculation of the number of HITS. 14 Bolus contrast injections for angiographic runs were not included in the analysis because of the high amount of artifacts seen and verified on the recording.
Statistical Analysis
Normally distributed continuous variables are presented as mean ± standard deviation (SD), and not-normally distributed continuous variables are presented as median (minimum-maximum). Categorical variables are presented as numbers (%). Pearson’s chi-squared tests were performed to compare categorical variables (demographic characteristics, cardiovascular risk factors, anatomical and procedural characteristics). Normally distributed continuous variables (total number of HITS between groups, MCA flow drop with clamping) were compared with 1-way ANOVA. Post-hoc tests were performed for the dual evaluation of the groups with a Bonferroni correction. Wilcoxon rank-sum test was used to assess differences between groups during the procedure. A P value of less than .05 was considered statistically significant. Statistical analyses were performed using SPSS software (StataCorp LP, College Station, TX, USA).
Results
Patient Characteristics
Thirty-six patients (mean age 69.5±10.59 years) who had ipsilateral MCA transtemporal acoustic windows and were monitored with TCD during carotid artery revascularization were included in the study (CEA 9, shCEA 11, tfCAS 4, TCAR 12). Twenty-four (77.8%) patients were male. No significant difference was seen between the four groups in the demographic characteristics (Table 1). The presence of cardiovascular comorbidities was remarkably high in all groups.
Patient Characteristics and Cardiovascular Risk Factors.
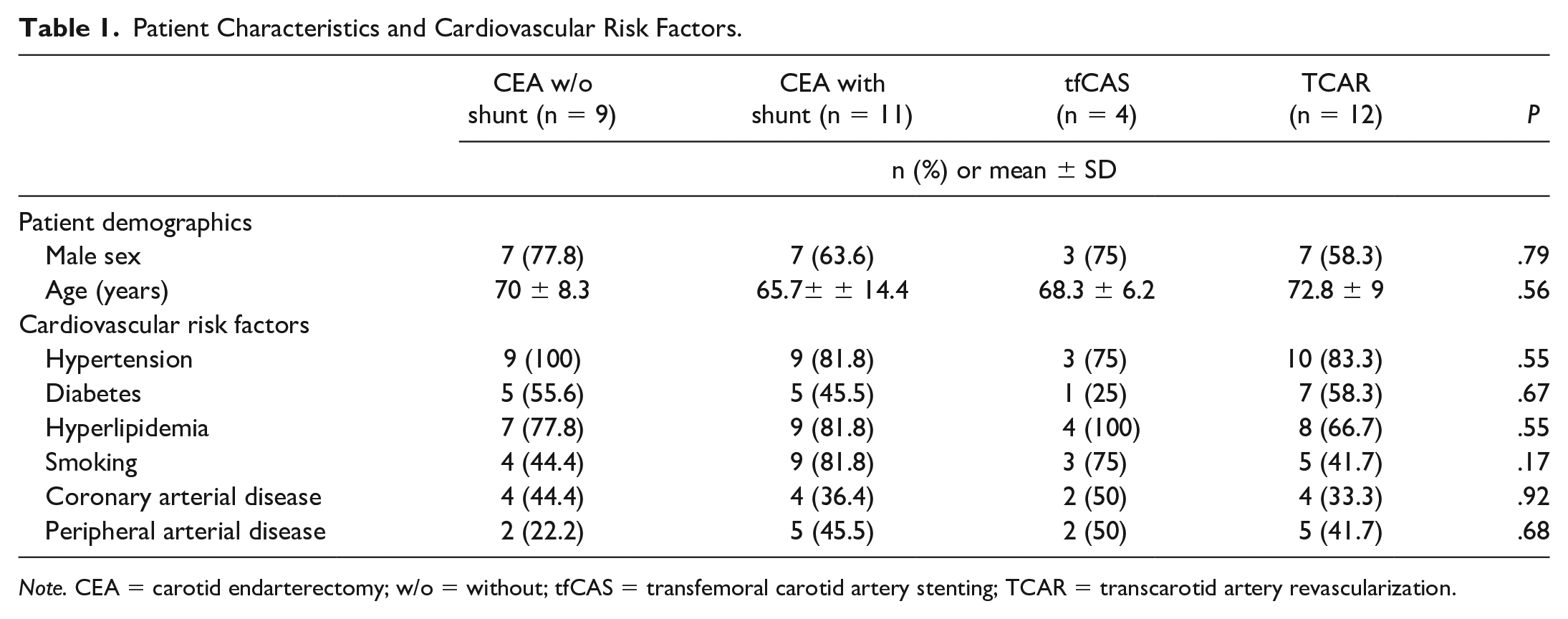
Note. CEA = carotid endarterectomy; w/o = without; tfCAS = transfemoral carotid artery stenting; TCAR = transcarotid artery revascularization.
Almost one-third (31%) of the patients had a carotid artery stenosis of greater than 90%, and 47% of the patients presented with neurological symptoms. Three patients were operated on more than 14 days following the onset of symptoms. A significantly higher proportion of patients (n = 7, 53.8%) had a previous ipsilateral carotid intervention in the TCAR group. The presentation features of carotid disease for the patient groups are listed in Table 2.
Presentation of Carotid Artery Disease.
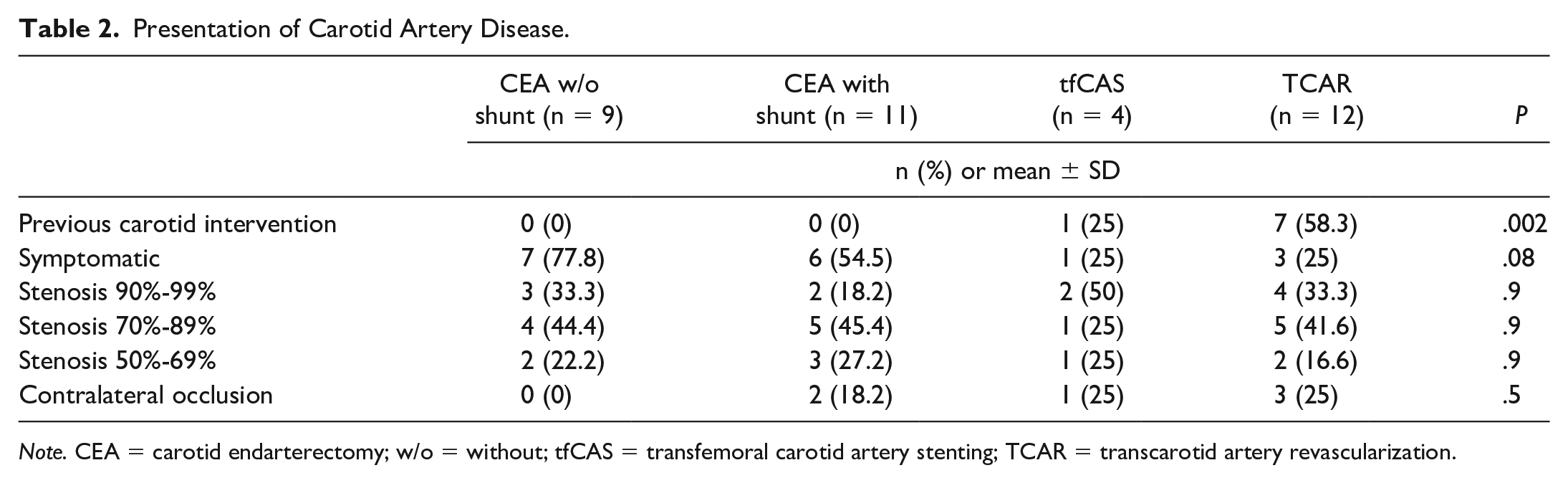
Note. CEA = carotid endarterectomy; w/o = without; tfCAS = transfemoral carotid artery stenting; TCAR = transcarotid artery revascularization.
MCA Flow Changes and Number of HITS
The CEA group had a significantly lower MCA mean flow velocity drop than the TCAR and the shCEA groups (20.6 ± 11.6 vs. 59.7 ± 33 vs. 64.5 ± 22.9, P = .001). The median number of HITS was significantly higher in the tfCAS group, 197.5 (range: 153-340), P = .004, when compared to the CEA, shCEA, and TCAR groups (5 [range: 0-90] vs. 10 [range: 3-72] vs. 29 [range: 2-74], respectively). Post-hoc analysis of total HITS numbers showed no significant difference between the CEA, shCEA, and TCAR groups. Still, the difference was significant when comparing tfCAS to any of the other groups (p < .001 for all paired comparisons).
Endovascular procedural phases (lesion crossing, predilation, stent deployment, and postdilation) were assessed in the TCAR and CAS groups. A significantly higher number of HITS was seen in the tfCAS group during all phases compared to the TCAR group (P = .002, P = .006, P = .04, P = .006, respectively) (Table 3). During TCAR, the highest embolization rate occurred during the stent deployment phase (0.5 [range: 0-60]), whereas the highest embolization rate occurred during the predilation phase in the tfCAS group (106.5 [range: 90-120]). No significant difference was seen based on the number of HITS per phase between the CEA and shCEA groups (Table 4).
Number of HITS in Endovascular Procedural Phases.
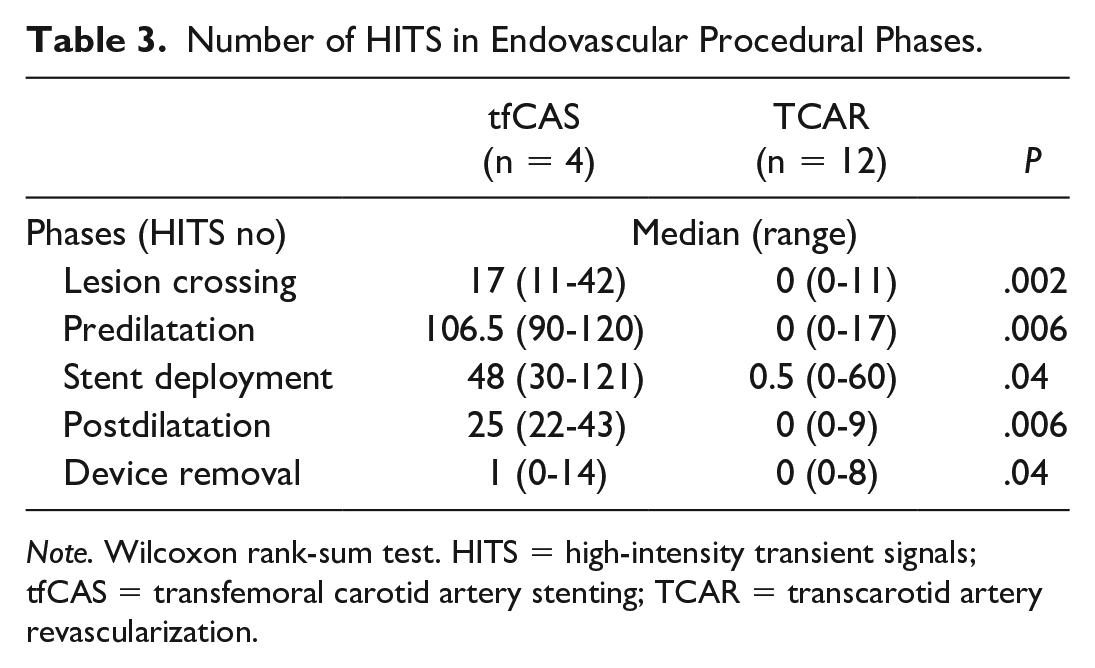
Note. Wilcoxon rank-sum test. HITS = high-intensity transient signals; tfCAS = transfemoral carotid artery stenting; TCAR = transcarotid artery revascularization.
Number of HITS by Phases in Carotid Endarterectomy Groups.
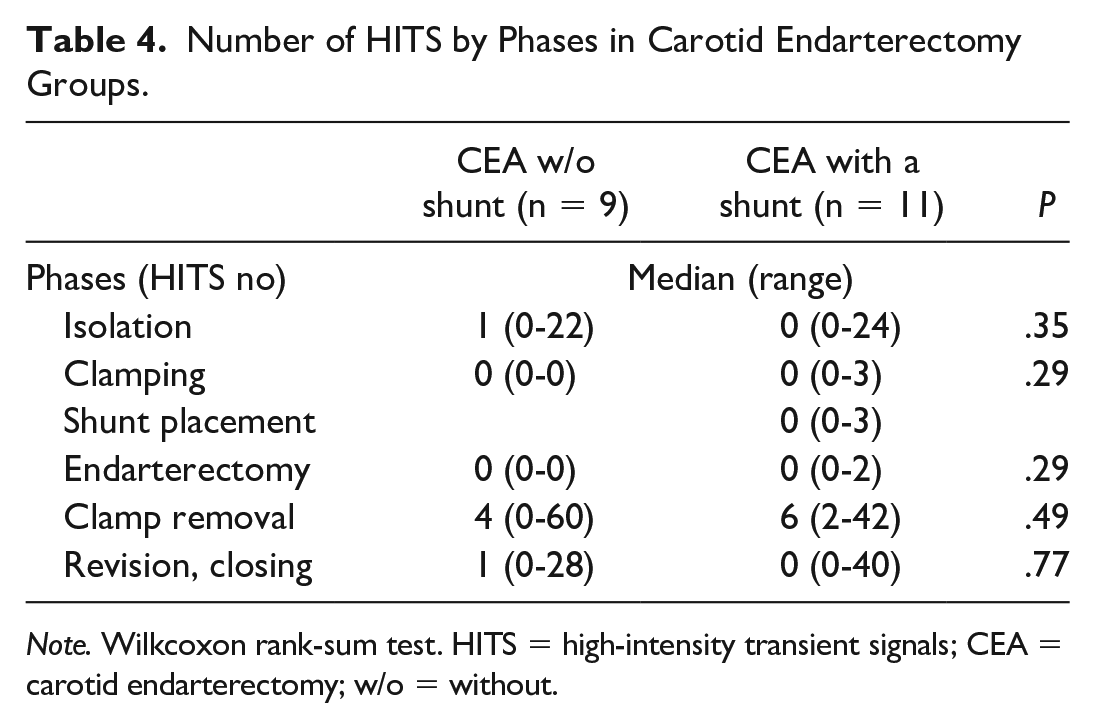
Note. Wilkcoxon rank-sum test. HITS = high-intensity transient signals; CEA = carotid endarterectomy; w/o = without.
In-Hospital Outcomes
No significant adverse events or in-hospital mortality were observed. Three patients in the CEA group developed neurological complications that were diagnosed by a neurologist during the postoperative course. Two of them had a transient ischemic attack (TIA), and the number of HITS was registered as 43 and 90, respectively. However, there was no correlation between the number of HITS and neurologic events. The third patient developed left upper extremity weakness within three days with unremarkable findings as seen in computed tomography imaging of the head. MCA mean flow velocity drop during clamping was below 15% in all three cases.
Discussion
CAD treatment remains an evolving area of vascular surgery. CEA has been proven to effectively prevent stroke in managing both symptomatic and asymptomatic carotid atherosclerotic disease.15-18 tfCAS was developed to treat selected patients with physiologic and anatomic risk factors that preclude CEA; nevertheless, tfCAS is associated with higher periprocedural stroke risk than CEA.16,19 TCAR represents a minimally invasive hybrid option that maintains favorable postoperative neurological outcomes. The main drawback of TCAR is the fate of the ipsilateral hemisphere during reversed flow, particularly in patients with contralateral CAD.
According to our knowledge, this is the only study that compares the embolic events and mean flow velocity of the MCA as assessed by TCD in the four following procedures: CEA, shCEA, tfCAS, and TCAR. TCD monitoring is a real-time, cost-effective tool for detecting intraoperative cerebral flow changes that enables operators to react immediately. This study presents our intraoperative TCD monitoring experience during TCAR, CEA with a shunt, CEA without a shunt, and transfemoral CAS procedures with paired comparisons. The overall intraoperative TCD monitoring analysis showed a significantly higher HITS rate during tfCAS than any of the other investigated treatment modalities, which supports the higher periprocedural stroke rate with CAS, as reported by previous studies. HITS occurring in the protected phases of CAS can result from particles smaller than the filter’s pore size or disintegration of larger particles during the procedure. A low number of HITS was also observed during TCAR with reversed flow. Retrograde flow from the external carotid artery, competing with the reversed flow, may explain these results. During TCAR, the highest embolization rate occurred during the stent deployment phase, whereas the highest embolization occurred during the predilation phase in the tfCAS group.
A drop in flow in MCA velocity during clamping suggests that the cerebral hemisphere cannot recruit adequate collaterals and indicates the need for shunting. MCA flow velocity decrease with clamping as a predictor of hemispheral hypoperfusion has been described before. 20 Although three patients developed neurological symptoms in the nonshunt CEA group, we assume that these events were related to embolization rather than cerebral hypoperfusion. Moreover, due to the small patient cohort involved in this study, our results are not representative of clinical outcomes.
A substantial number of studies have focused on using intraoperative neuromonitoring techniques to elucidate potential biomarkers indicative of stroke and other neurological complications. Although intraoperative EEG (electroencephalography) monitoring was used in the lead-in phase to evaluate safety, 21 perioperative TCD monitoring allows us to visualize changes in the cerebral flow and embolic events, enabling immediate reaction during the procedure. Moreover, TCD can detect, quantify, and localize gaseous and solid microemboli in the intracranial cerebral arteries. 2
Multiple randomized, controlled trials have repeatedly shown relatively higher stroke rates but lower rates of periprocedural MI among patients undergoing tfCAS as compared with CEA.15,22-24 Although it is a common finding that CAS is associated with more intraoperative embolization than CEA, direct comparisons may be partially distorted because contrast injection occurs only in CAS and generates emboli-like signals that are often picked up by automatic detection programs. As micelles of the contrast agent can generate TCD signals, embolic loads may be overestimated for CAS. 25 To avoid this problem, we excluded the signals directly related to contrast injection. Rosenkranz et al 26 showed that most cerebral microemboli that occur during CAS are gaseous, while less than 15% of microemboli are solid. They noted no relationship between the number of solid emboli and new ischemic lesions as detected by diffusion-weighted imaging (MR-DWI), which can also be evidence that not only can solid emboli have an ischemic effect on the brain, but that any emboli could be hazardous.
Nonetheless, despite the less-invasive nature of CAS, it still yielded higher embolization and periprocedural stroke rates than CEA, likely due to manipulating endovascular catheters and wires through the unprotected aortic arch or the stenotic carotid artery potentially embolizing unstable plaques. 27 To mitigate this risk, embolic protection devices have become a mainstay of tfCAS. Despite the reduced number of microemboli reaching the brain, Garami et al 11 showed that the use of embolic protection devices does not eliminate distal microembolization during CAS and suggested TCD monitoring for all interventions. Additionally, distal protection devices have limitations, including varying pore size, malposition, tilting, and the need for recapture that can still allow plaque debris to embolize. 28
The ENROUTE transcarotid neuroprotection and stent system (Silk Road Medical Inc, Sunnyvale, CA, USA) was developed for TCAR to protect against strokes during CAS. The system requires direct surgical cut-down to access the CCA and blood flow reversal during stent delivery. Continuous reversal of flow provides neuroprotection by clamping the proximal CCA and allowing retrograde blood flow from the ICA to flow through an extracorporeal filter before returning to the femoral vein. Contrary to distal filter protection, flow reversal provides embolic protection before any instrumentation or lesion crossing, which is a window of markedly increased embolization risk. Notably, the aortic arch is not traversed, and the lesion is not crossed until blood flow is reversed, thereby allowing any embolic material to be removed from the carotid circulation and filtered in the external circuit before returning to the circulation.
TCAR has shown promising initial results in the ROADSTER multicenter trial with a 30-day stroke rate of 1.4%. The 30-day all-stroke rate was the lowest reported to date in any prospective trial of CAS. This has translated clinically into lower stroke and death rates from TCAR, matching CEA. 12 In comparison, patients undergoing tfCAS in the Carotid Revascularization Endarterectomy vs. Stenting Trial (CREST) had a 4.1% periprocedural stroke rate. 6 Patients undergoing CEA had a 2.3% stroke rate and 5.3% cranial nerve injury rate. 22 On the contrary, TCAR has been shown to overcome certain limitations of transfemoral carotid stenting with distal protective filters and the new DW-MRI lesion rates, and stroke presentation are comparable with CEA.9,10,29 Our study is consistent with these findings, since the embolic load during TCAR was similar to that during CEA.
The retrospective study design and the relatively low numbers of patients in the various treatment groups are limitations of our study. The inability to differentiate between solid and gaseous emboli with TCD could also have influenced the outcomes. Although studies investigating DWI-MRI positive intracranial lesions after carotid artery revascularization have also found that a higher proportion of patients develop intracranial lesions after CAS than other revascularization techniques, this study did not include DWI-MRI imaging. Postoperative DWI-MRI imaging should be included and addressed in future studies to validate these results.
Conclusion
This is the first study comparing embolic events and mean flow velocity in the MCA by TCD in the four following procedures: CEA, shCEA, tfCAS, and TCAR. TCD monitoring is a useful tool for detecting intraoperative cerebral flow changes that enables the operator to react immediately. Our findings are consistent with the data published by previous clinical trials. CEA and TCAR are comparable in terms of intraprocedural microembolic signals and are associated with a significantly lower number of intraprocedural microembolic signals than tfCAS.
Supplemental Material
sj-doc-1-jvu-10.1177_15443167211032371 – Supplemental material for Preliminary Experience With Transcranial Doppler Monitoring in Patients Undergoing Carotid Artery Revascularization: Initial Observations on Cerebral Embolization Patterns
Supplemental material, sj-doc-1-jvu-10.1177_15443167211032371 for Preliminary Experience With Transcranial Doppler Monitoring in Patients Undergoing Carotid Artery Revascularization: Initial Observations on Cerebral Embolization Patterns by Busra Tok Cekmecelioglu, Peter Legeza, Kavya Sinha, Pooja Tekula, Alan Lumsden and Zsolt Garami in Journal for Vascular Ultrasound
Footnotes
Author’s Note
This study has been read during Society of Vascular Ultrasound 2020 Conference.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A.B.L. Boston Scientific: Consulting Fees (e.g., advisory boards), Speaker’s Bureau; Cook Medical: Research Grant; Intact: Consulting Fees (e.g., advisory boards); W.L.G.: Consulting Fees (e.g., advisory boards), Grants, Research, Investigator, Other Financial or Material Support, Speaker’s Bureau. Z.G.—Neural Analytics: Consulting Fees (e.g., advisory boards), Speaker’s Bureau; Silkroad Medical: Consulting Fees (e.g., advisory boards), Speaker’s Bureau. Other co-authors have nothing to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.