
Abstract
Keywords
Introduction
Preterm birth (<37 weeks’ gestation) occurs in about 10% of live births. 1 With advances in neonatal care, most individuals born preterm now survive to adulthood. 2 However, adults born preterm have increased risks of hypertension and cardiovascular diseases.3 -6 The underlying mechanisms remain unclear. There are conflicting reports relating low birth weight and preterm birth with endothelial dysfunction, vascular compliance, and carotid artery intima-media thickness (IMT). Children with cardiovascular risk factors have increased morbidity related to atherosclerosis in adulthood. 7 Carotid IMT is a known subclinical imaging marker for early atherosclerosis.8,9 In children with risk factors for atherosclerosis, carotid IMT was elevated.8,9 However, despite recommendations set by the Mannheim carotid IMT and plaque consensus, 8 and the Association for European Paediatric Cardiology (AEPC) Working Group on Cardiovascular Prevention, 9 IMT measurement techniques are variable, thus adding a challenge to data interpretation and comparisons across studies.
Techniques for measuring IMT include B-mode ultrasound imaging (manual, semi-automated, or automated) and radiofrequency echo tracking, but these do not necessarily correlate with each other. The reason behind the lack of correlation could stem from the fact that the underlying mechanism is not necessarily atherosclerosis and measurement technique is less adequate due to body habitus.3 -6 The latter is in keeping with the lack of correlation of the techniques in children. 10 More importantly, the variability in the technique in young adults could be the main reason for the lack of correlation. The manual technique reflects individual measurements and is inherently less robust than the semi-automated technique which gives an average measurement along a segment of the vessel. Calipers tracing the IMT could over or underestimate the measurement depending on the operator, especially knowing that IMT is around half a millimeter. Contradictory reports in the literature on preterm birth also pertain to the fact that the preterm population is not homogeneous with respect to associated comorbidities. In particular, as a result of oxygen supplementation, bronchopulmonary dysplasia is thought to reduce the elastin content of blood vessels. Furthermore, young adults born preterm may have a smaller body surface area, 11 necessitating adjustments in IMT measurement technique. A recent meta-analysis showed no difference in carotid IMT between adults born preterm and full-term controls, even though cardiovascular risk was increased. 11 The Health of Adults born Preterm Investigation (HAPI) did not demonstrate a difference either, even when controlling for confounding variables such as blood pressure.12 -15 On the other hand, it is known that in older adults, the semi-automated IMT technique has a stronger association with cardiovascular outcomes than the manual technique. 16
The intraclass correlation coefficient (ICC) between manual and semi-automated IMT measurement techniques in adults at low risk for cardiovascular disease was shown to be 0.74. 17 However, knowing that the pathophysiology of vascular disease could be different in young adults born preterm, the reliability of the techniques has not been studied in this population and could indicate early vascular changes and contribute to the risk stratification, hence the importance of evaluating the best technique to identify these changes. The primary objective of the present study was therefore to compare the intra-observer agreement for B-mode ultrasound manual and semi-automated IMT measurement techniques in the risk assessment for early vascular changes in young adults born preterm. Secondary objectives were to determine whether correlation was affected by the anthropometric characteristics in order to identify the better technique to predict IMT changes in young adults born preterm below 30 weeks’ gestation. Clinical implications will include the use of the best suited technique, or avoidance of comparing different techniques and misinterpreting risk assessment initially and during follow-up in this particular population of young adults born preterm.
Methods
Study Population
We used data from the Health of Adults born Preterm Investigation. The HAPI (ClinicalTrials.gov Identifier: NCT03261609) is a cross-sectional, prospective, observational cohort study comparing the cardiometabolic health of young adults aged 18 to 29 years who were born very preterm (<30 weeks’ gestation by definition) to that of matched peer controls born full-term (≥37 weeks’ gestation by definition).12 -15 Results of the clinical aspects, anthropometrics, laboratory, and imaging findings of the same cohort presented in this article were published previously but without any evaluation of the technical considerations for the IMT measurement techniques that make up the core of the actual study.12 -15 The study was approved by Institutional Research Ethics Board and participants signed informed consent. Exclusion criteria were severe neurocognitive impairment and pregnancy limiting participation. Participants were recruited from September 2014 to December 2016. Anthropometric measurements, blood pressure, and fasting blood samples were obtained on study visit day.
Measures
Resting brachial blood pressure was measured using an automated oscillometer (DINAMAP, model DPC300M-CF, GE Medical Systems Information Technologies, Inc., Milwaukee, WI, USA). Measurements were recorded 3 times with 5-minute breaks between them; we used the average of the last 2 measurements.
All IMT measurements were performed on the right common carotid artery according to Mannheim recommendations. 8 The head of the patient was tilted 45° to the left. A longitudinal 2D-ultrasound image of the common carotid artery was taken with a 12-MHz linear transducer (18L7) of a Toshiba Aplio XG ultrasound machine (British Columbia, Canada), depth 4 cm, gain around 60, dynamic range 60 dB, 1 focal zone and 42 frames per second. Image resolution was 0.1 mm/pixel. The mean IMT was obtained on the far wall of the common carotid artery, 10 mm proximal to the end of the common carotid artery during diastole, that is, at optimal resolution when the vessel diameter was at its smallest dimension (Mannheim recommendations). M’Ath SR software version 3.2.1 (Argenteuil, France) allows detection of the smallest and the largest arterial diameter using the distensibility function by analyzing a video sequence of 5 cardiac cycles long. IMT and vessel diameter were calculated at the minimal distension reflecting end-diastolic measures. The rational for measuring IMT during diastole stems from the recommendations of Mannheim and literature showing that using the systolic normative data to compare IMT obtained during diastole when IMT is increased can lead up to 42% overestimation of the risk for cardiovascular disease. 18 In one study in children, IMT measurements obtained during R-wave using electrocardiogram were significantly higher than those obtained subjectively during diastole. 19
Semi-automated measurement was performed using M’Ath SR software connected to the Toshiba ultrasound machine. Both machines are still in function in many institutions with even an active online version of the M’Ath SR interface. A 1-cm line was drawn by the operator next to the lumen-intima interface. The software then measured the mean thickness over that segment (Figure 1A). We aimed at a quality index of at least 0.5, meaning that the software took into account at least 50% of the measurements in the calculation of the mean IMT over the segment in question and a standard deviation of 0.05 mm. Five to 10 manual measurements were performed on the same ultrasound segment after calibration by drawing with calipers on a truly horizontal image parallel to the probe surface the shortest vertical distance between 2 echogenic (bright) lines (equivalent to placing 2 calipers on each interface), representing the lumen-intima interface and the media-adventitia interface (intima-media complex) (Figure 1B). To account for differences in lumen diameter between preterm and full-term individuals, we calculated the relative IMT, that is, the ratio of IMT to end-diastolic carotid diameter. One sonographer took the ultrasound images and a radiologist did the measurements. Data generated or analyzed during the study are available from the corresponding author by request.
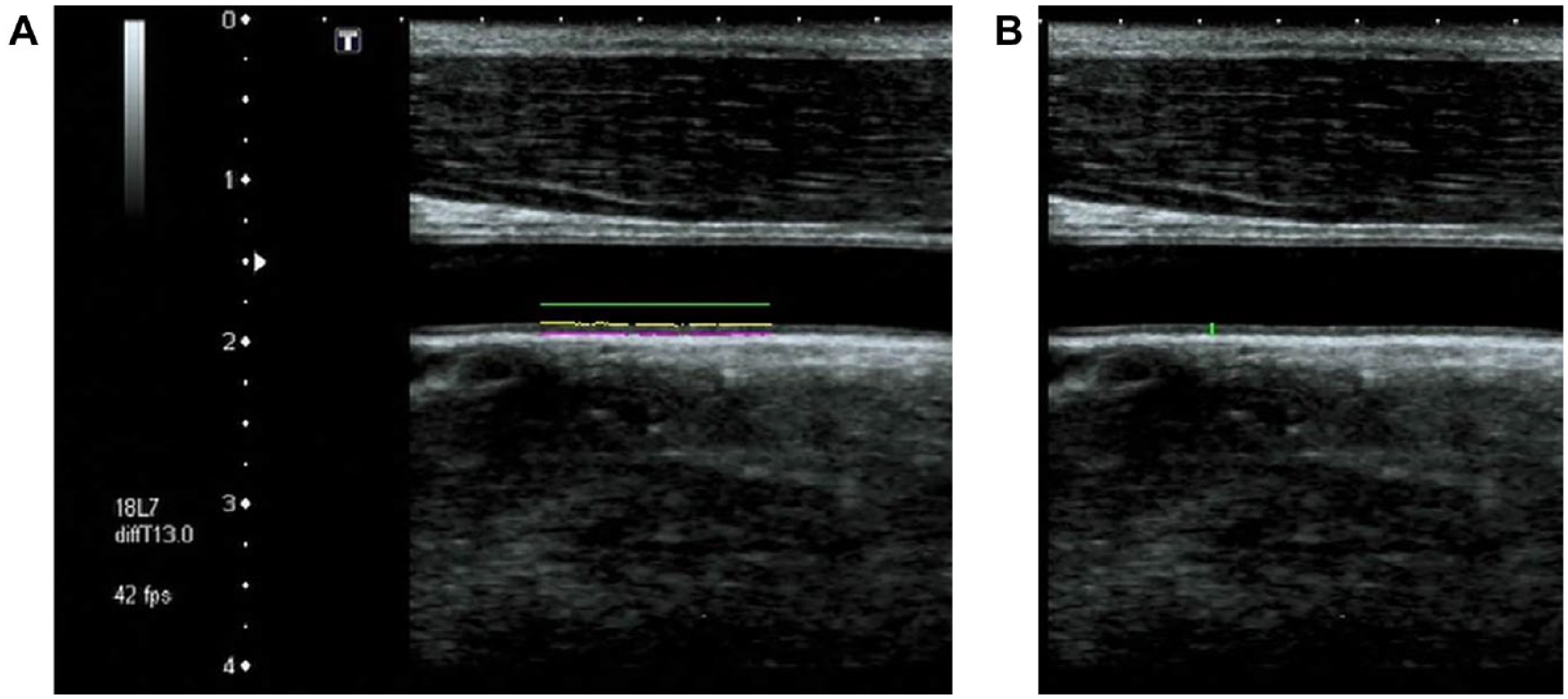
Measuring intima-media thickness (IMT).
Statistical Analysis
We used Student t tests for descriptive statistics of anthropometric data (mean and standard deviation) and comparison of continuous variables. We calculated 2-way mixed, average score ICC (c, k) to examine the agreement between manual and semi-automated techniques using the psych package in R. We used Pearson’s correlation coefficients for the relationship between technique type and body mass index (BMI), age, and comorbidities in preterm- vs full-term-born participants. We examined absolute differences between the 2 techniques, with Bland-Altman plots showing differences of the mean of the paired measurements. A P value <.05 was considered statistically significant. All analyses were performed using R Statistical Software version 3.6.0 (International Open Source collaborative).
Results
The HAPI cohort included 86 preterm and 85 full-term participants (Figure 2). Mean ages were 23.2 (±2.4) years and 23.3 (±2.3) years, respectively. More than half were women (58% and 56%, respectively). Mean diastolic blood pressure was higher in the preterm group (72 ± 9 vs 68 ± 8 mm Hg) (Table 1).
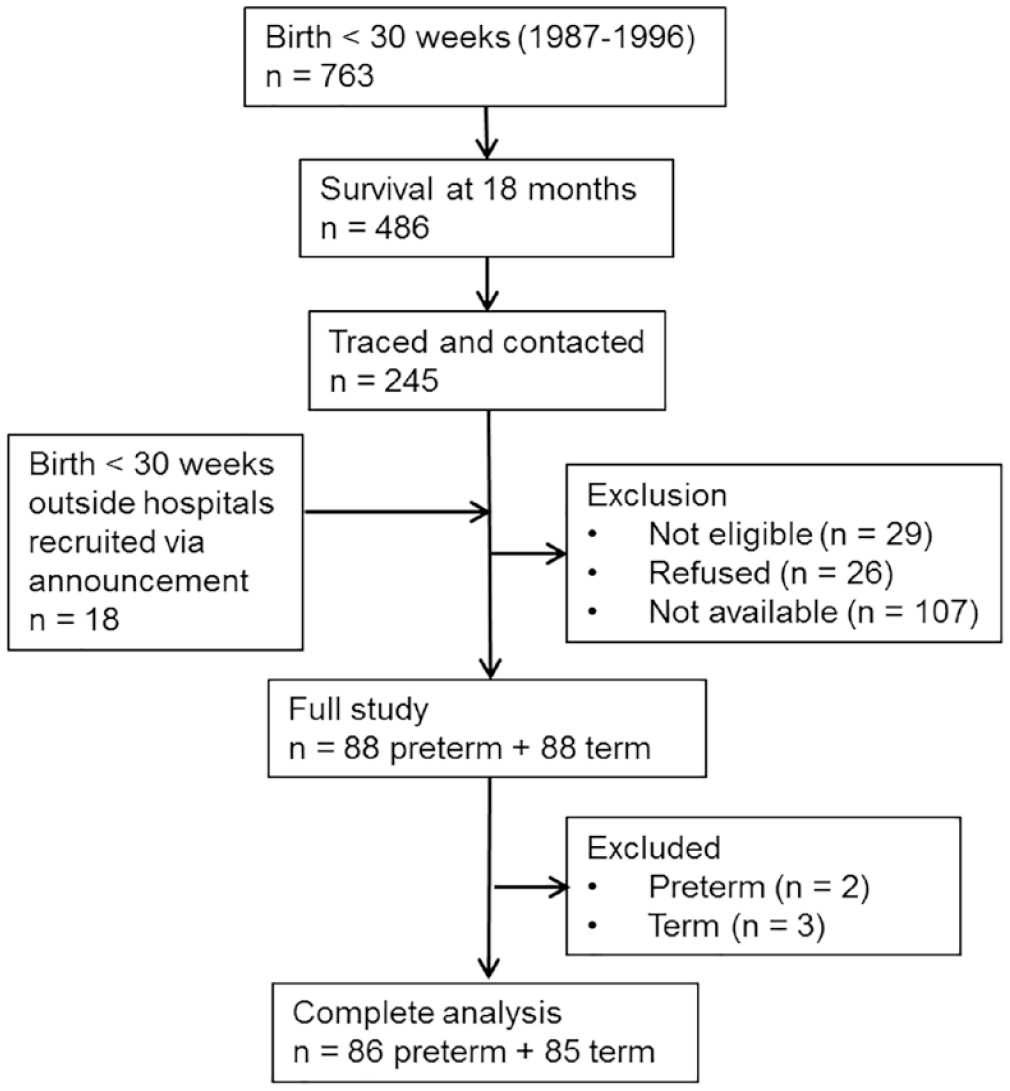
Flow diagram of the Health of Adults Born Preterm Investigation (HAPI) cohort.
Participant Characteristics.
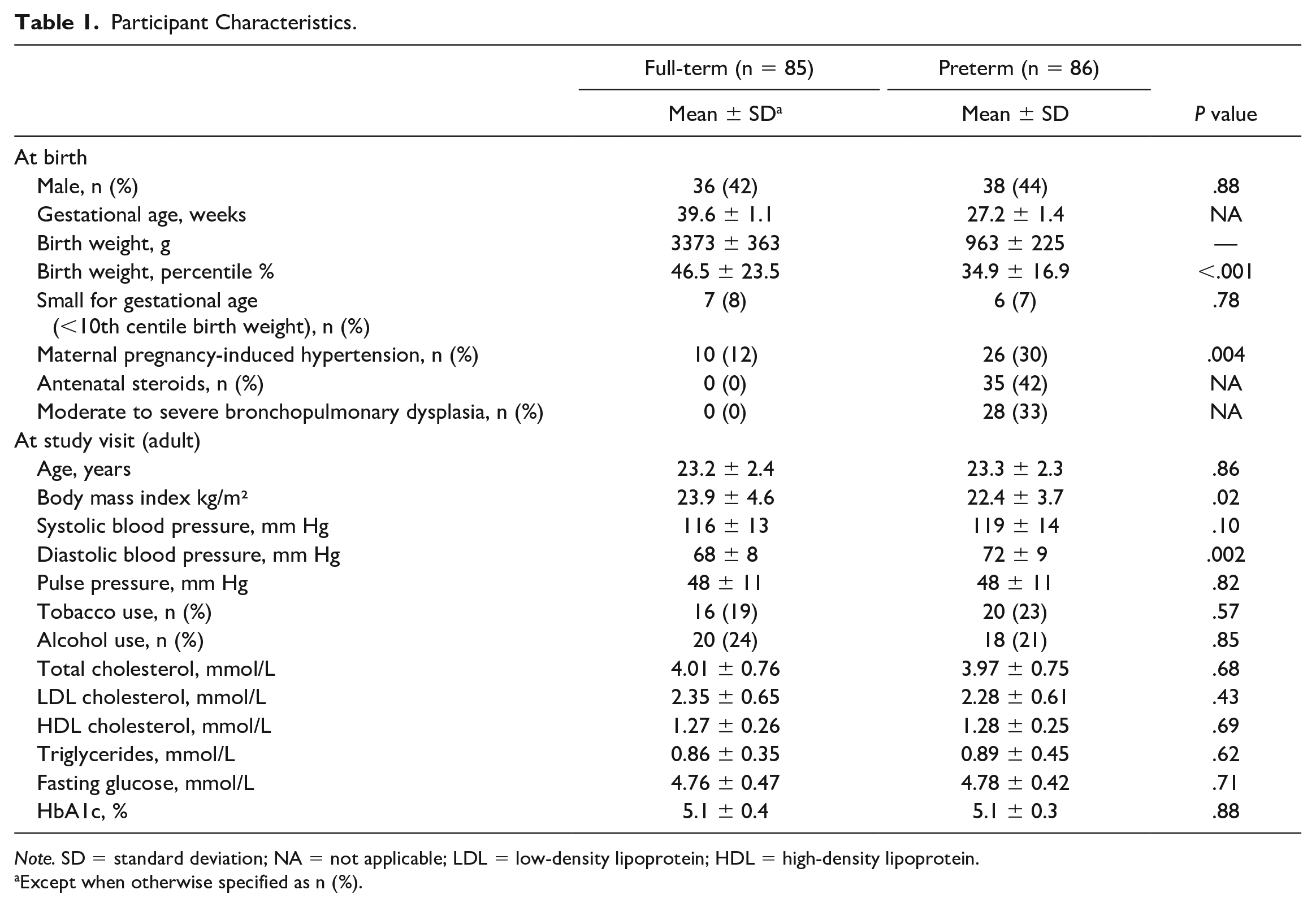
Note. SD = standard deviation; NA = not applicable; LDL = low-density lipoprotein; HDL = high-density lipoprotein.
Except when otherwise specified as n (%).
We conducted subgroup analyses comparing manual vs semi-automated measurements (Table 2). Regardless of technique used, the IMT distribution was normal. No significant differences were observed in carotid diameter or IMT for either technique (Table 2). In each of the 2 techniques, the preterm group had a nonsignificant but slightly smaller carotid diameter resulting in a slightly higher relative IMT (IMT/carotid diameter ratio) than that of the full-term group (Table 2).
Subgroup Analyses By Preterm vs Full-Term Birth and By Women vs Men, for Both Manual and Semi-Automated IMT Measurement Techniques.
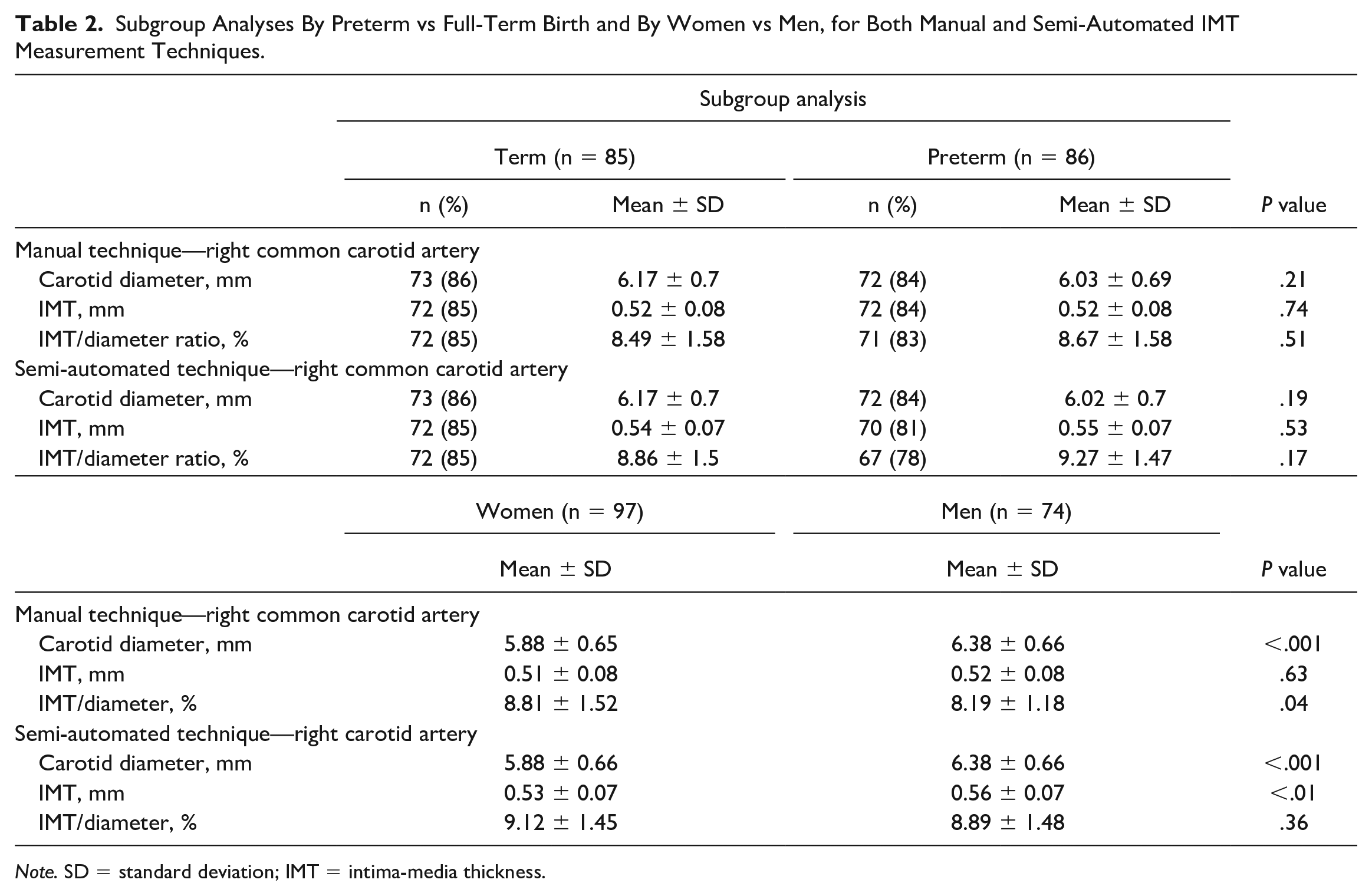
Note. SD = standard deviation; IMT = intima-media thickness.
When stratified by sex, IMT and carotid diameter were significantly higher in men than women, for the semi-automated technique (Table 2). While not statistically significant, the semi-automated technique yielded higher values throughout. This was confirmed on a Bland-Altman plot (Figure 3).
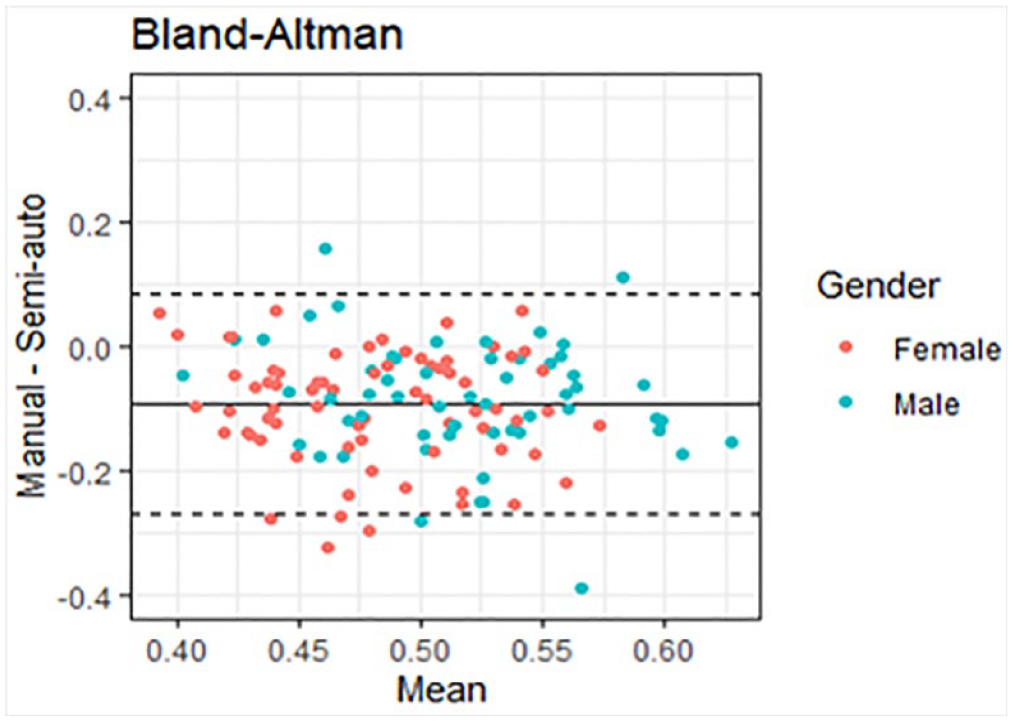
Bland-Altman plot showing consistent disparity between the manual and semi-automated techniques of carotid intima-media thickness (IMT) measurement.
We evaluated intra-observer variability in IMT measurement for the manual and semi-automated techniques. The intra-observer correlation was good for the manual technique (ICC = 0.73; 95% CI = [0.65-0.79]) but better for the semi-automated technique (ICC = 0.79; 95% CI = [0.86-0.91]). However, there were more missing values using the semi-automated technique due to failure of edge detection of the lumen-intima and intima-adventitia interfaces by the software (Table 2).
When analyzing the entire cohort, we found moderate correlation between the 2 techniques (Pearson correlation coefficient 0.40 (P < .01); ICC = 0.58) (Table 3). This did not change when stratifying by prematurity status, r = 0.35, P < .01, ICC = 0.53 for the preterm group, and r = 0.44, P < .01, ICC = 0.62 for the full-term group (Table 3). For BMI ≥25 (definition for overweight and obesity in adults) vs BMI <25, the 2 techniques were moderately correlated (ICC = 0.65 and 0.51, respectively for each weight group) and similarly for the presence of adult comorbidities such as hypertension, glucose intolerance, adiposity, and obstructive lung disease or absence thereof (ICC = 0.59 and 0.54, respectively for each group of with or without comorbidities).
Correlation Between Manual and Semi-Automated IMT Measurement Techniques for All Participants, Stratified By Prematurity Status, Adult Body Mass Index, and Adult Comorbidities.
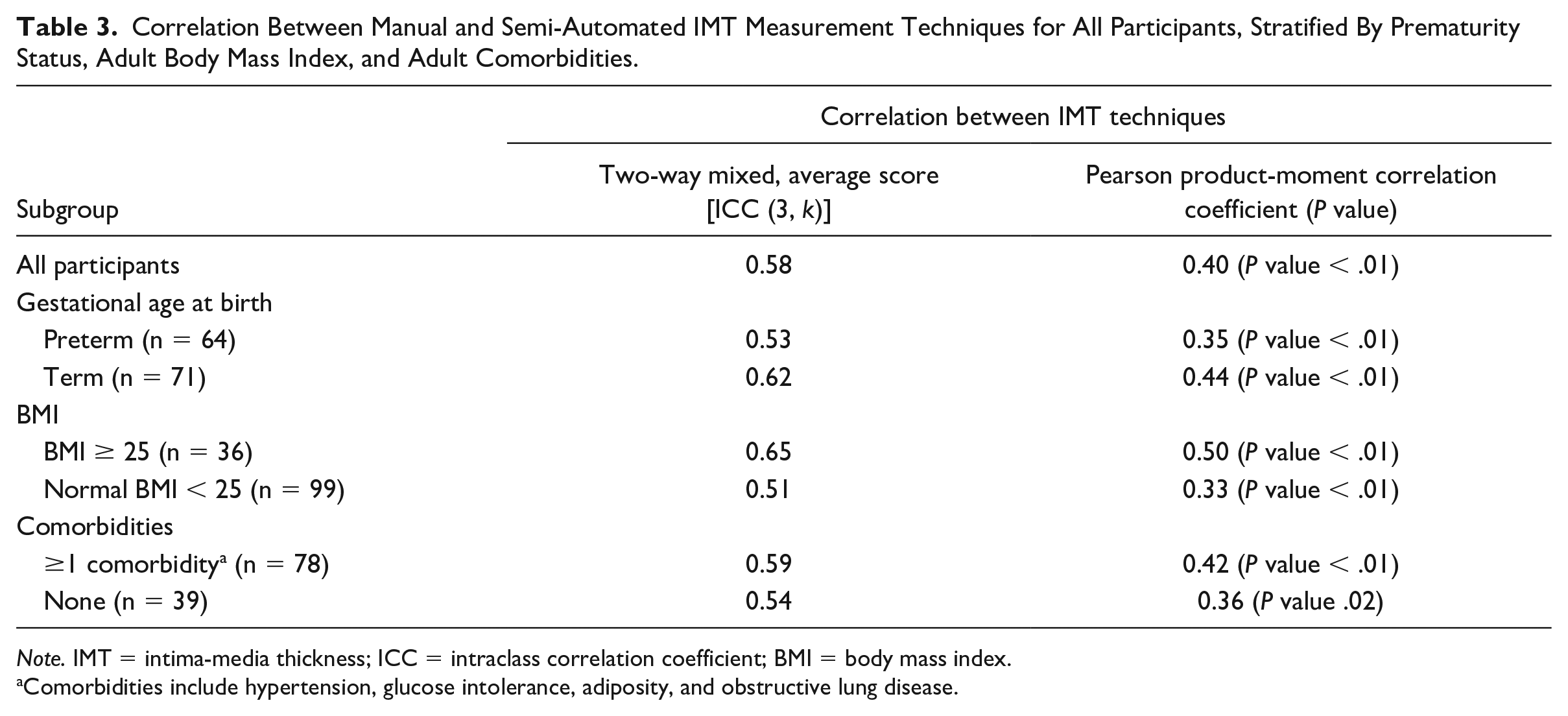
Note. IMT = intima-media thickness; ICC = intraclass correlation coefficient; BMI = body mass index.
Comorbidities include hypertension, glucose intolerance, adiposity, and obstructive lung disease.
Although moderately correlated, both techniques were good at discriminating participants according to BMI (manual P = .01 and semi-automated P < .01) (Table 4). IMT measures using either technique did not correlate with age (Pearson’s correlation coefficient = 0.02 (P = .76) and 0.14 (P = .10) for the manual and semi-automated technique, respectively) (Table 4). These results were confirmed by scatterplots (Figures 4 and 5).
Subgroup Analyses of the Correlation Between Each of the 2 IMT Measurement Techniques With Respect to Adult Age and Body Mass Index.
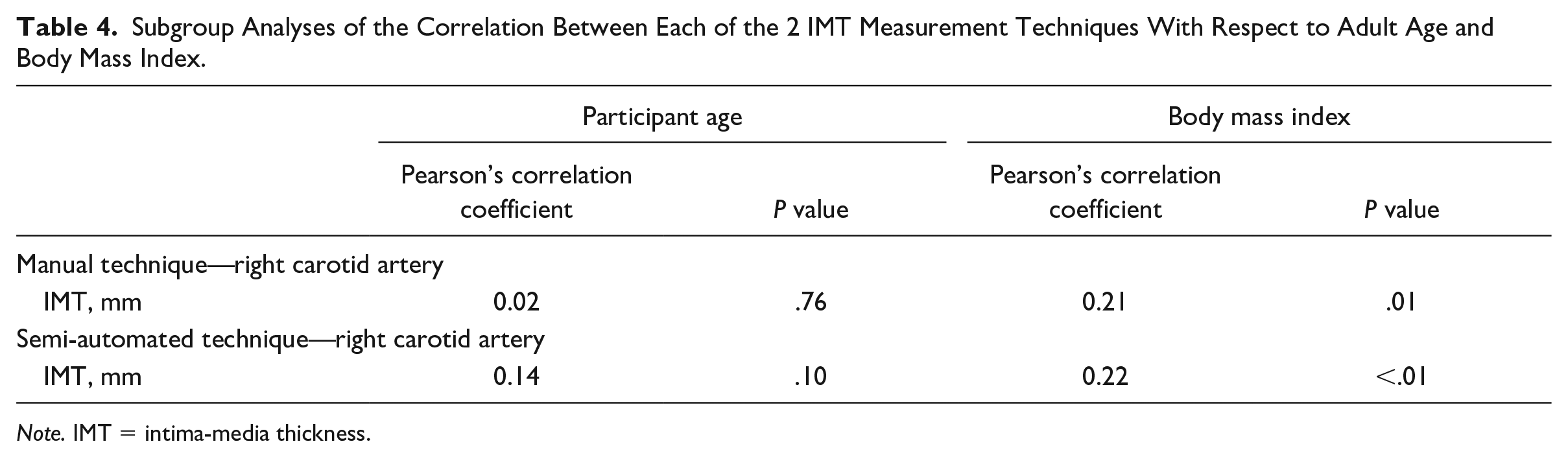
Note. IMT = intima-media thickness.
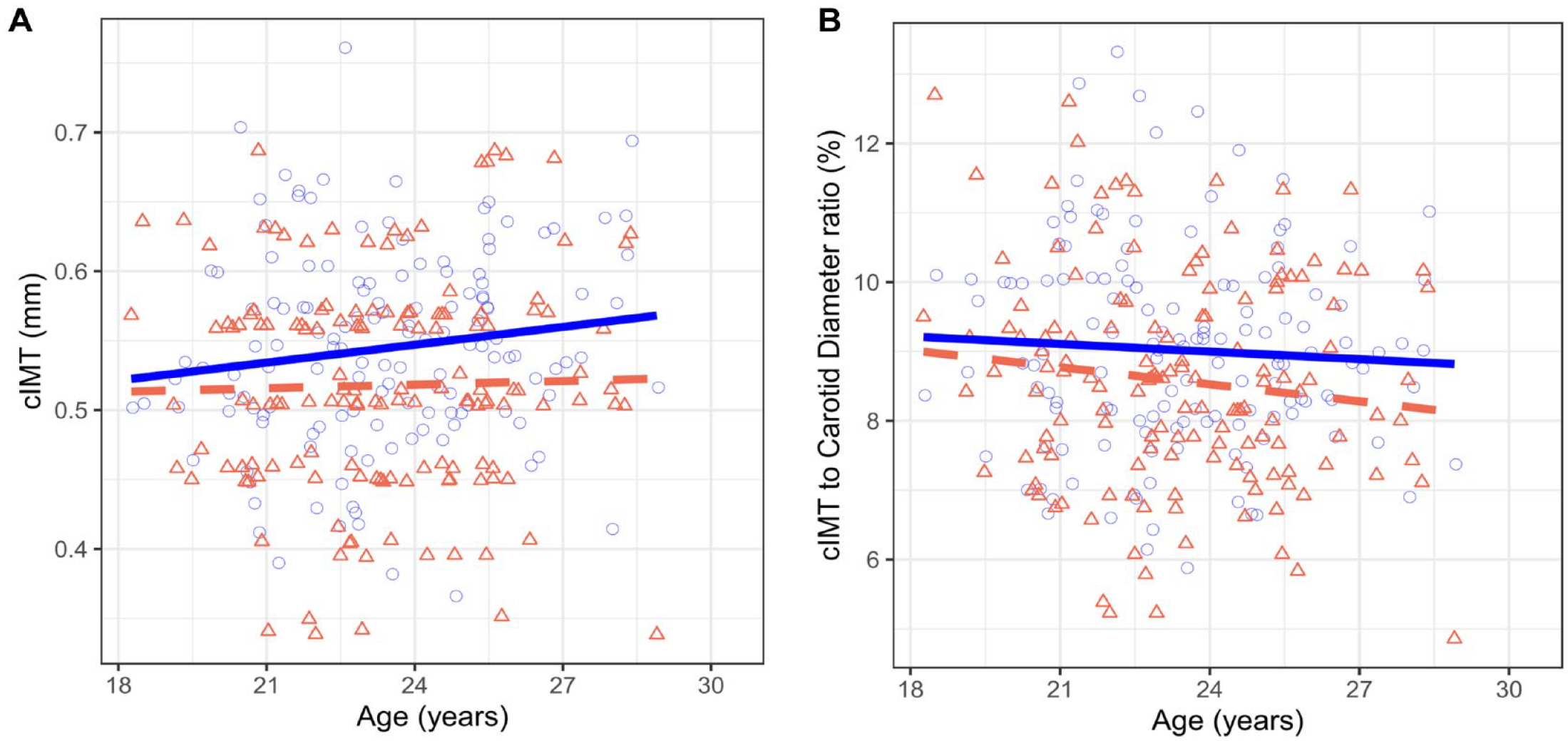
Scatterplots comparing manual and semi-automated techniques of carotid intima-media thickness (IMT) measurements, as a function of age: (A) mean cIMT; (B) cIMT/carotid artery diameter ratio.
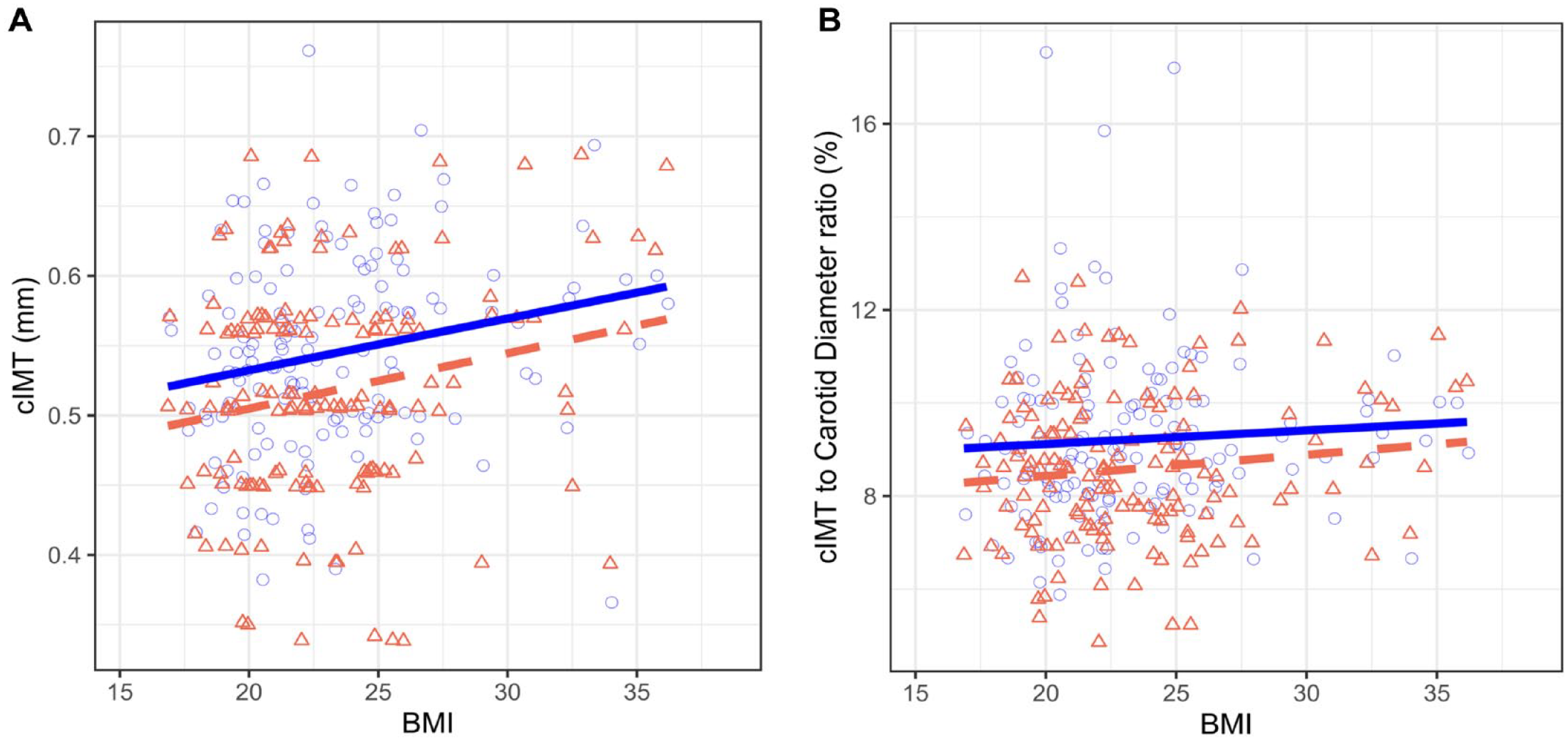
Scatterplots comparing manual and semi-automated techniques of carotid intima-media thickness (IMT) measurement, as a function of body mass index (BMI): (A) mean cIMT; (B) cIMT/carotid artery diameter ratio.
Discussion
We found that the manual and semi-automated IMT measurement techniques on B-mode ultrasound moderately correlated with each other. Intra-observer agreement was better for the semi-automated technique. The semi-automated technique showed a slight but statistically significant higher IMT in men than women (Figure 6). The IMT of the carotid artery is a known marker for cardiovascular disease.20 -23 However, although the risk of cardiovascular disease is increased in the growing number of adults born preterm, and especially those born extremely-to-very preterm (gestational age <30 weeks), the literature is conflicting on the use of carotid IMT as a diagnostic marker.13 -15,24,25 We conducted a detailed study of 2 IMT measurement techniques to see whether they correlated with each other and which of the 2 could better distinguish individuals at risk in this population known to have a different pathophysiology underlying the vascular changes compared with classic atherosclerosis. It is the first study exploring technical variability with respect to IMT measurement in young adults born preterm.
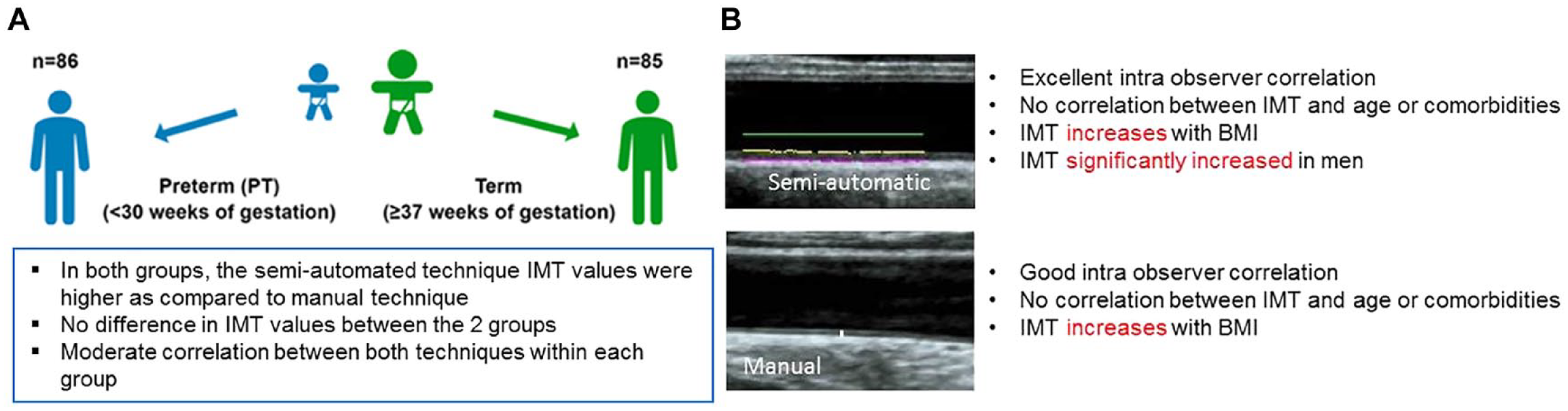
Summary of main results when comparing the 2 techniques of intima-media thickness (IMT) measurement: (A) adults born preterm vs full-term; (B) all participants, regardless of birth group.
In previous studies, low birth weight was not significantly associated with increased IMT,23,24 except in cases of exacerbated postnatal growth. 25 Kerkhof et al 26 found no relationship between gestational age and IMT. Mohlkert et al 27 reported that although arteries of 6-year-old children were 5% to 10% narrower in those born preterm than full-term, the difference became nonsignificant after adjusting for current body surface area. Similarly, a small study of 21 preterm vs 29 full-term infants revealed no difference in IMT. 28 Other than Lee at al., who did find a significant increase in IMT in children at mean age 12 years who were born preterm, 29 our results on both techniques are consistent with the existing literature. In adults aged 24 to 39 years, IMT was found to increase with age.30,31 In their study of the Framingham Offspring cohort, Polak et al 32 found that the maximal IMT improved risk stratification.
Although IMT is associated with age 33 and risk factors, we want to emphasize that the age range in our participants is small (age ranges between 18 and 29 years), probably pertaining to the lack of statistical association and poor correlation between age and IMT in contradistinction to the other published literature in adults with larger age ranges and no history of prematurity. The lack of a significant difference in IMT between the 2 groups could be related to 3 factors: the techniques are heterogeneous affecting accuracy; IMT is inherently thinner indicating the need for a different, technique similar to children; and lastly, the underlying pathophysiology for the vascular disease in young adults born preterm includes factors other than early atherosclerosis.
That IMT should be interpreted relative to arterial diameter is consistent with the finding of altered arterial distensibility in preterm participants. 15 However, in this study, the difference in IMT relative to carotid diameter between preterm and full-term birth was not consistently statistically significant when using both techniques. IMT has been suggested as a screening tool for both children and adults who are overweight/obese.34 -36 When combined with preterm birth, one would expect a correlation between risk factors and increased IMT in our study population.
Although manual and semi-automated techniques correlate well in adults,17,37,38 our results are in keeping with Mac Ananey et al 17 who found variability between the 2 techniques. In their study of 126 healthy adults, with a Pearson correlation of 0.8 but an ICC of 0.74 between the 2 techniques, manual IMT overestimated the measurements with respect to the semi-automated technique, while the latter was more reproducible. 17 Our results were along the same lines with respect to reproducibility but with weaker correlation. However, in our study, semi-automated values were higher. This could be because our population was different from theirs (mean age 40, low-risk participants). 17 Notably, we corroborated, as they did, the lack of a gold standard in the present study and existing literature. 17 Although semi-automated techniques performed better, 16 longitudinal studies similar to the Framingham Offspring cohort study 32 are needed in this particular population of young adults to examine the relationship between specific IMT technique and the incidence of cardiovascular disease outcomes.
Due to operator dependency, manual measurement may have accuracy limitations, but in adult studies, there is usually good agreement between the automated and the manual techniques, with greater ease of processing for the former. 39 Molinari et al 40 found good correlation using Atheros software. In a review, Naik et al 41 concluded that none of the existing semi-automated and automated techniques were perfect and that further validation studies were needed to better segment the vessel wall. They also noted that the semi-automated technique could be better than fully automated, since the operator could identify areas of erroneous edge detection by the software. They concluded that the intra-observer variability in the semi-automated technique was comparable to that of the manual technique.41,42 Furthermore, the radiofrequency technique for measuring IMT is mostly semi-automated or automated. Studies have found good correlation between radiofrequency-based measurements and manual B-mode measurements in adults. 43 However, previous work found poor correlation in children. 10 It could be that, like in children, the IMT is small in young adults born prematurely, and any differences are beyond detection capability. This has important clinical implications, as this population of young adults is different from the full-term-born adults with typical risk for atherosclerosis. Therefore, the same technique specific IMT measurements should be used consistently to assess risk for vascular disease in this population of young adults born prematurely. We recommend, therefore, to include IMT measurement in the assessment of cardiovascular risk in this population of young adults but to interpret the results carefully taking into account the technical factors and normative data obtained in similar technical circumstances.
There were some limitations to our study. First, although we aimed at 1 cm proximal to the end of the common carotid artery, we cannot know whether the measured segment was at an identical location in all patients. Second, although we aimed at a diastolic measure, there may have been variability, as we did not use electrocardiography. Third, there were slightly more missing data for the semi-automated technique, a rate higher than what is present in the literature. 39 Edge detection accuracy was not always assessed on the day of the research visit, hence the higher rate of absent data for the semi-automated technique after quality control checks. The measurements could not be recalculated because the quality of the interfaces on the initial image was poor, the semi-automated algorithm being dependent on an optimal image to start with. Importantly, participants were all young adults, ranging in age from 18 to 29 years. Because the age range was so narrow, the cardiovascular risk at young ages is relatively low, and the techniques are heterogeneous, differences in IMT by age may be difficult to detect with existing methods, as confirmed by the scatterplots.
Conclusion
While both IMT measurement techniques correlate, the semi-automated technique was more reproducible overall, and semi-automated was more indicative in distinguishing sex differences in IMT. For these reasons, and because the semi-automated technique generated higher values, it would not be a good approach to mix techniques in assessing vascular changes in young adults born preterm. Although the current study does not confirm a gold standard, adherence to a single technique, preferentially the semi-automated technique, is recommended.
Footnotes
Acknowledgements
The authors are grateful to Danielle Buch, Medical Writer, Research, for critical revision and substantive editing of the entire manuscript. They thank all research nurses, technical team from the Division of Cardiology and the Medical Imaging Department, and the Applied Clinical Research Unit of the Sainte-Justine Research Centre, and especially, all study participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Institutes of Health Research (CIHR) grant MOP-133572 (to TML and AMN); the Canadian Foundation for Innovation (to AMN); the CHU Sainte-Justine Foundation (to AMN) and the Professoral Support Committee of the Department of Radiology, Radiation Oncology and Nuclear Medicine of the University of Montreal (to REJ).