
Abstract
Introduction:
Subclavian artery stenosis of >50% has been linked to an increased risk of cardiovascular morbidity, complications after carotid interventions, and difficulty in managing hypertension. This has led to increased emphasis on screening for these lesions. In addition, these lesions may be associated with upper extremity symptoms including claudication and pain at rest.
Methods:
A retrospective review of patients who were referred over a 2-year period for arm pain in the setting of suspected or proven subclavian artery stenosis or occlusion was performed. This was compared to an unmatched cohort of patients who underwent carotid artery duplex with subclavian artery duplex for other reasons. Data included measuring the interbrachial systolic pressure difference (>15 and >20 mm Hg), arm-arm index, and hand acceleration time (HAT).
Results:
Among the172 patients studied, 48 had subclavian artery stenosis or occlusion and 26 of these had corresponding symptoms. Female gender (P = .012), history of coronary intervention (P = .007), hypertension (P = .039), and arm-arm index of <0.9 (P = .0001) were significantly associated with subclavian artery stenosis or occlusion. A HAT of >100 milliseconds was significantly associated with symptomatic subclavian artery stenosis or occlusion.
Conclusions:
An arm-arm index of <0.9 is a useful tool for screening for subclavian artery stenosis. In patients with subclavian artery stenosis, HAT may be useful in confirming that the arm symptoms are due to this particular lesion.
Keywords
Introduction
Identifying a significant difference in the brachial systolic pressures (interbrachial pressure or IBP) can have significant clinical implications. An IBP value of >10, >15, or >20 mm Hg has been correlated with subclavian artery stenosis, difficulties in managing long-term hypertension, occult carotid and coronary disease, complications following carotid endarterectomy, and overall increased risk of cardiovascular morbidity and mortality. In our region, not all vascular laboratories perform an evaluation of the subclavian arteries at the time of a carotid duplex examination. Significant subclavian artery stenosis has been defined as >50% diameter reduction. Measurement of brachial systolic pressure can be affected by antihypertensive management and the patient’s overall blood pressure at the time of the study, and some centers use the arm-arm index (AAI) as a parameter to take these variables somewhat into account. Our group has been studying the potential utility of hand acceleration time (HAT) in determining the clinical perfusion state of the extremity.1,2 We wished to study the utility of IBP, AAI, and HAT in identifying significant and symptomatic subclavian artery stenosis.
Methods
This was a retrospective review of patients who underwent carotid duplex examinations over a 2-year period (1/2000-1/2002) performed by one registered vascular technologist. In our vascular laboratory, all carotid duplex examinations include evaluation of the subclavian artery and, where visualized, the brachiocephalic artery. Because our study focused on the significance of subclavian artery stenosis, patients with >50% diameter reduction in either internal carotid artery, or those with bilateral subclavian artery stenosis, were excluded. Patients with lesions in the axillary or more distal arteries were also excluded, as were patients with upper extremity dialysis access fistulas and grafts. Significant subclavian artery stenosis was defined as >50% diameter reduction with a peak systolic velocity of greater than 250 cm/s, poststenotic turbulence, and abnormal monophasic flow distally. Subclavian artery occlusion was defined as absence of color flow in the subclavian artery with low-velocity monophasic or continuous flow distally, with or without evidence of collateral flow, and retrograde flow into the subclavian artery. Symptoms were those that were specific to the index upper extremity.
Brachial systolic pressures were obtained at the start of the study using standard cuffs. The AAI is calculated from the right and left arms as lower systolic blood pressure/higher systolic blood pressure. In our practice, we have defined an abnormal AAI as <0.9. The HAT is the precise measurement of the time from onset of systole to the peak of systole in the arterial Doppler spectral waveform. Care is taken to lower the baseline, increase the sweep speed to include 4 cardiac cycles, and lower the scale, so the waveform takes up 3-quarters of the spectral waveform space. This precision allows for consistent and accurate acceleration time measurements which are recorded in milliseconds. In every upper extremity, HAT was measured in the deep palmar arch on the ulnar and radial sides. The “best” (i.e., lowest) HAT value was used in the analysis. We have previously speculated that a “normal” HAT is ≤100 ms.1,2 The presence of asymptomatic and symptomatic subclavian artery stenosis was correlated with the IBP (≥15 and ≥20 mm Hg), AAI (<0.9 and <0.8), and HAT (≤100 or >100 ms).
Comorbidity definitions included active smoking (smoker), diabetes requiring medication (diabetes), prior coronary revascularization (CAD), and hypertension requiring medications (HTN). Permission to perform the study was obtained through the Washington State University Institutional Review Board. Statistical analysis was performed using SPSS 28.0.1 (IBM Corp., Minneapolis, MN). Results are expressed as mean ± standard deviation. Univariate analysis was performed using the χ2 test for categorical data and independent t-test for continuous variables. All variables significant to a level of P ≤ .1 were entered into a logistic regression model to determine predictors of the outcomes in question. Statistical significance was taken to be P ≤ .05. Sensitivity, specificity, and negative and positive predictive values were calculated. 3
Results
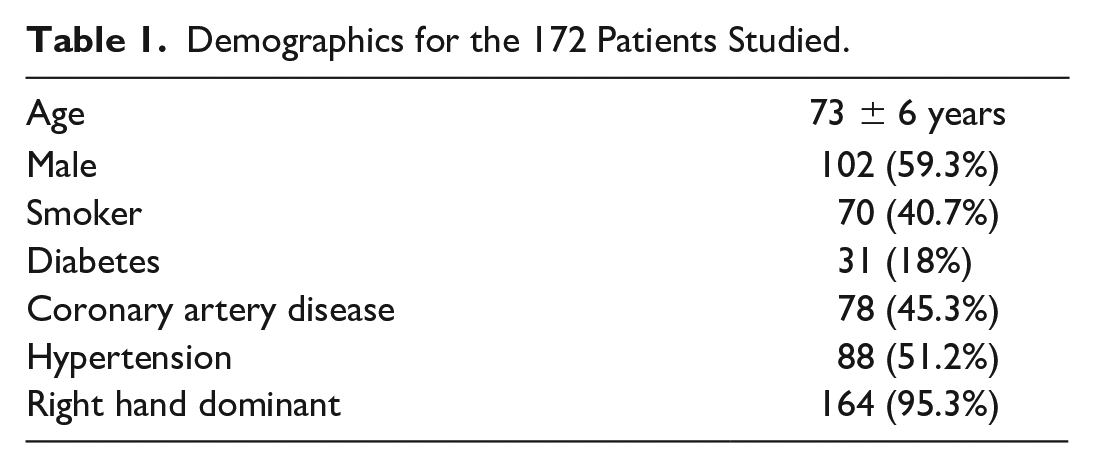
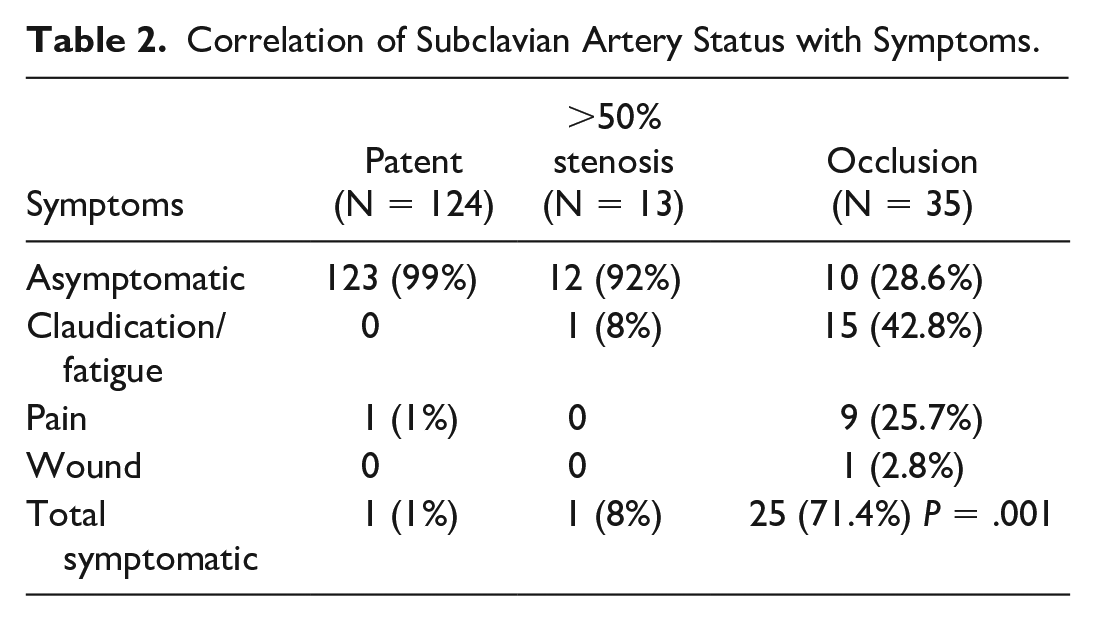
A total of 172 patients were included in the study, of whom 27 had unilateral arm symptoms (Tables 1 and 2). Of the patients included, none had positional (i.e., vertebrobasilar) symptoms. No patient had end-stage renal disease requiring dialysis, and no patient had stenosis of the brachiocephalic artery. One of the symptomatic patients had no significant subclavian artery stenosis, normal IBP, AAI, and HAT ≤100 milliseconds but had a history of prior nerve injury, and this patient was excluded from further analysis. Forty-eight patients had significant subclavian artery stenosis or occlusion, 26 of which had symptoms (Table 2). The population was predominantly male and right-handed. Two patients had undergone prior carotid-subclavian bypass procedures. Patients with occlusion were significantly more likely to have symptoms than those with stenosis. There was no difference in age between asymptomatic (74.7 ± 9.6 years) and symptomatic (72.1 ± 9.1 years, P = .228) patients. There were no differences between radial HAT (87.3 ± 27.6 ms) and ulnar HAT (86.4 ± 28.7 ms; P = .17).
Demographics for the 172 Patients Studied.
Correlation of Subclavian Artery Status with Symptoms.
Patients with subclavian artery stenosis did have a significantly higher HAT than those without (with stenosis 122.7 ± 36.8 ms vs without 78.0 ± 5.1 ms, P = .0001). Patients with symptomatic subclavian artery stenosis also had a significantly higher HAT than those with stenosis who were asymptomatic (with symptoms 145.7 ± 32.9 ms vs without symptoms 80.2 ± 8.6 ms, P = .0001).
Multivariate analysis identified female gender and AAI < 0.9 to be correlated with subclavian artery stenosis or occlusion, while HAT > 100 milliseconds correlated with symptomatic subclavian artery stenosis (Table 3). This did not change when adding subclavian artery occlusion to the analysis. In terms of detecting or excluding significant subclavian artery stenosis, HAT >100 milliseconds performed less well in terms of sensitivity and negative predictive value compared to the other measurements (Table 4). However, in terms of symptomatic stenosis, HAT >100 milliseconds outperformed the other measurements in terms of positive predictive value (Table 5). The patients who had subclavian artery occlusion and were asymptomatic and had HAT ≤ 100 milliseconds were noted to have developed extensive collateral flow into the index upper extremity.
Univariate and Multivariate Analysis.
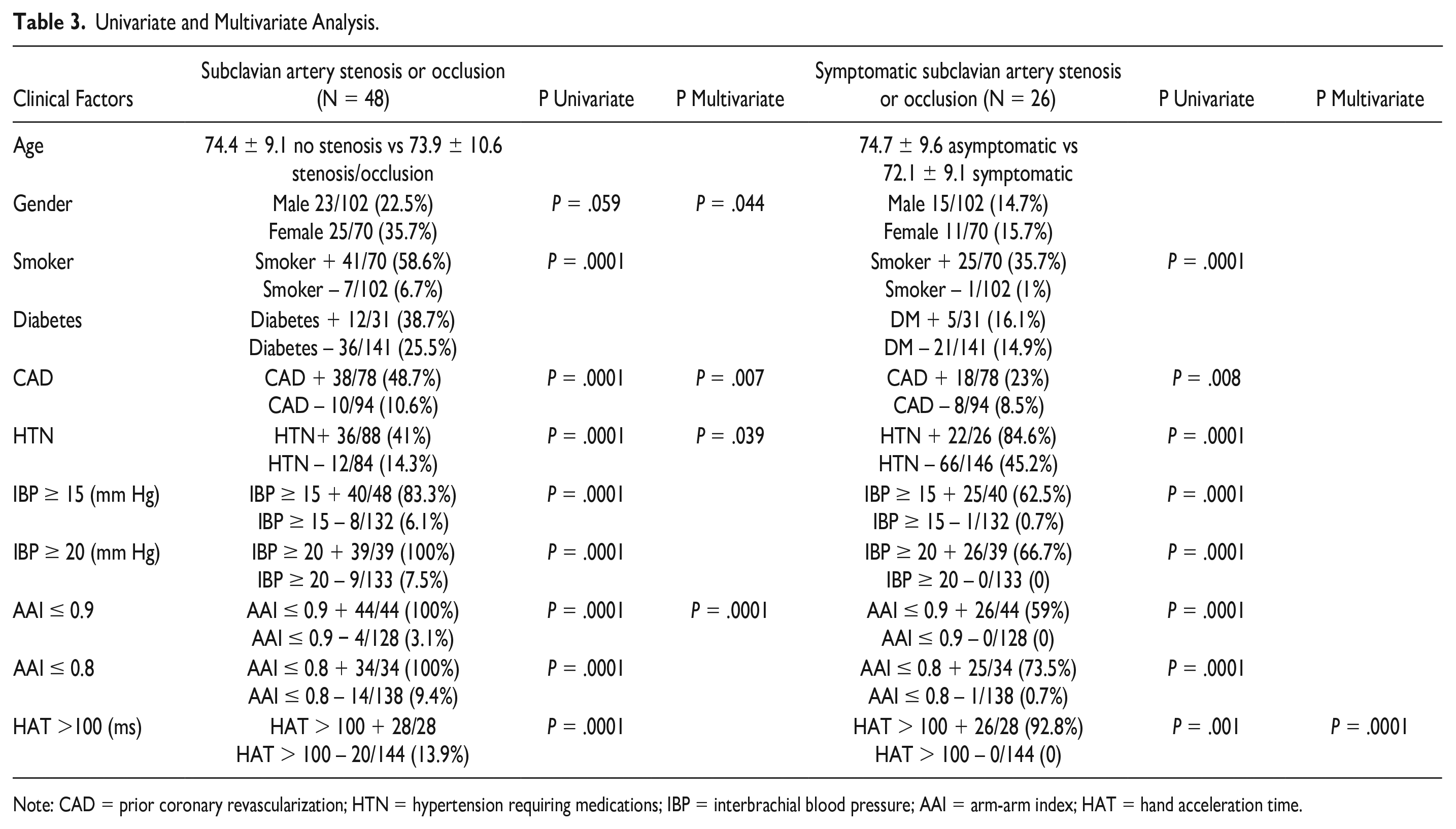
Note: CAD = prior coronary revascularization; HTN = hypertension requiring medications; IBP = interbrachial blood pressure; AAI = arm-arm index; HAT = hand acceleration time.
Any Subclavian Artery Stenosis or Occlusion.
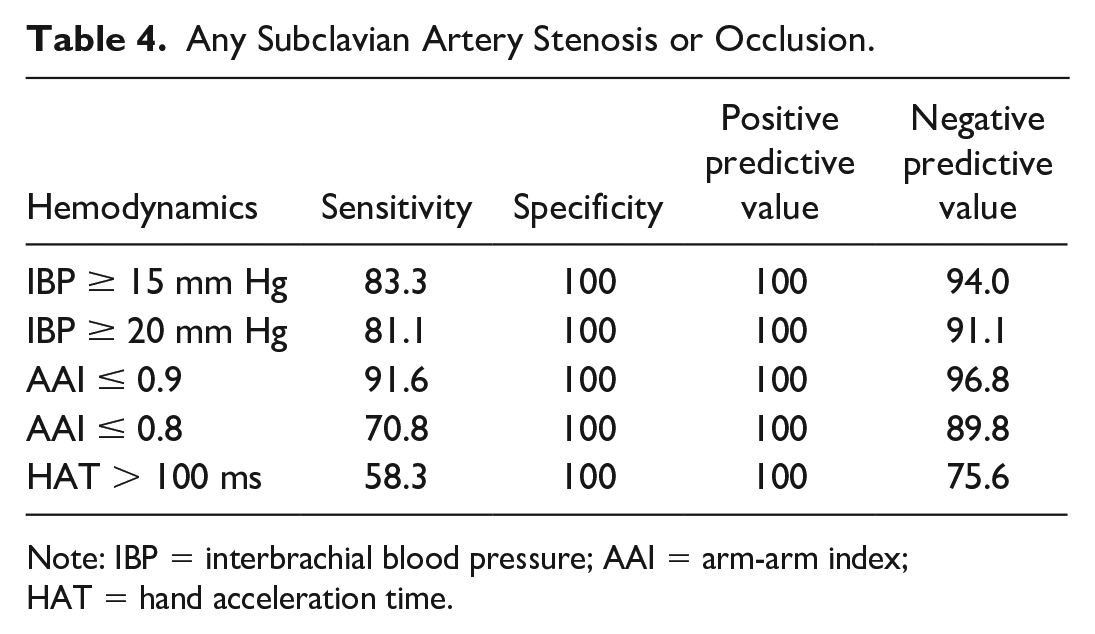
Note: IBP = interbrachial blood pressure; AAI = arm-arm index; HAT = hand acceleration time.
Symptomatic Subclavian Artery Stenosis or Occlusion.
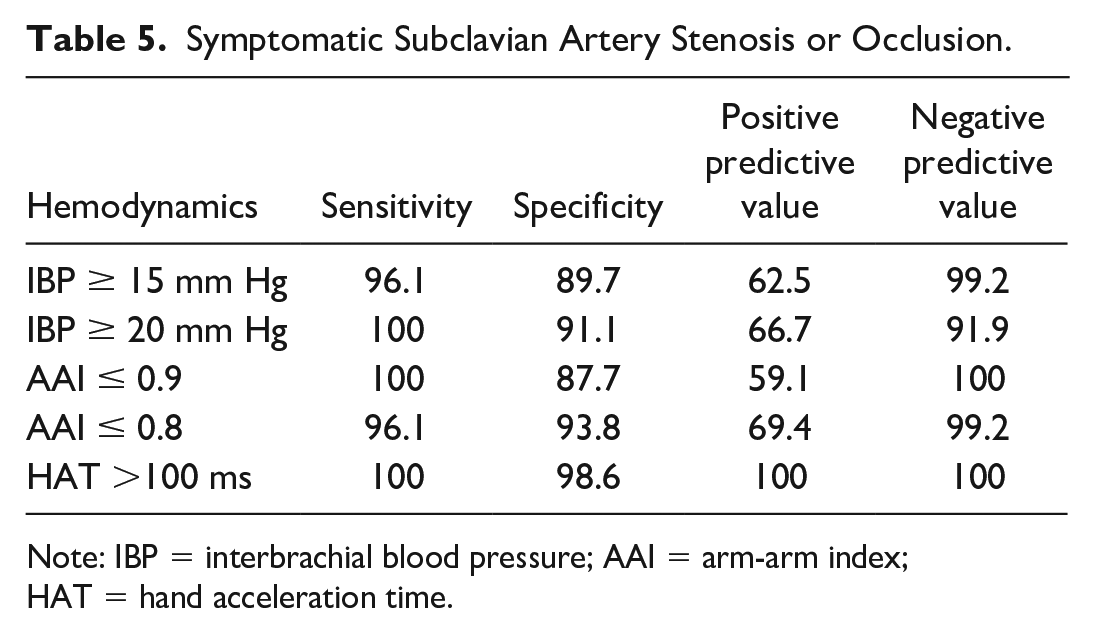
Note: IBP = interbrachial blood pressure; AAI = arm-arm index; HAT = hand acceleration time.
Of the 26 patients with symptoms, 12 underwent revascularization (including 2 who had a prior carotid-subclavian bypass with occlusion), 10 by open surgical revascularization and the remainder by endovascular stenting. In all cases at follow-up, IBP was ≤10 mm Hg, AAI > 0.9, and HAT ≤ 100 (range: 60-90) milliseconds. Incidental note was made that “abnormal” IBP, AAI, and HAT all correlated with a history of prior coronary artery intervention (Table 3).
Discussion
Differences in IBP have, absent traumatic injury or brachial embolization, been attributed to subclavian artery pathology. Brachiocephalic arterial stenosis may also affect the right arm pressure; however, this would be detected during carotid duplex, either directly by visualization, or indirectly by reduced common carotid flow. Significant subclavian artery stenosis has been defined as >50% diameter reduction. 4 Using IBP to screen for subclavian artery stenosis has a number of clinical implications. Differences in IBP (including >10, >15, and >20 mm Hg) have been linked to difficulty in managing hypertension in the outpatient setting, increased incidence of peripheral arterial disease as well as relevant but occult coronary and carotid disease, complications following carotid intervention (in part due to errors in blood pressure management), and all-cause increased cardiovascular morbidity and mortality.4-8 Up to 10% of patients have an IBP difference of >10 mm Hg, with associated increased risk of cardiovascular events, and the risk appears to increase with an IBP of >15 mm Hg. 8
Huibers and colleagues found that an IBP of >20 mm Hg had a sensitivity of 23% and specificity of 98% for identifying significant unilateral subclavian artery stenosis. 4 Deser and colleagues noted in their study that 65% of patients with an IBP of ≥20 mm Hg had significant subclavian artery stenosis. 8 A recent meta-analysis noted that with each 5 mm Hg IBP difference, even in asymptomatic patients, there was an increased risk for all-cause mortality, cardiovascular mortality, and cardiovascular events. 9 The authors recommended an IBP value of 10 mm Hg as the upper limit of normal. Thus, evidence of significant IBP differences (assuming that there is not bilateral disease) at the very least suggests that patients be counseled about lifestyle and risk factor modification.
Our results suggest that measurement of brachial systolic pressures, whether reported as an absolute difference (IBP) or as an index (AAI), is useful to screen for subclavian artery stenosis. In particular, an AAI <0.9 appears particularly efficacious. In theory, describing the IBP difference as a ratio may mitigate influences such as blood pressure medication and low cardiac output. However, for identifying patients whose symptoms are caused by the subclavian artery pathology, a HAT >100 milliseconds appears to have the highest correlation. Patients with subclavian stenosis and normal HAT had evidence of collateral perfusion, predominantly from the vertebral artery in proximal lesions. Our patients did not have “subclavian steal syndrome” which is classically a syndrome of vertebrobasilar insufficiency in the setting of subclavian artery stenosis or occlusion. Labropoulos and colleagues found that symptomatic subclavian steal syndrome correlated with IBP differences of >40 mm Hg. 10 However, our patients had upper extremity claudication symptoms, and IBP differences were more sensitive to this presentation.
Our study has a number of limitations. It is retrospective, single-center, single-vascular technologist, and a relatively small sample size compared to larger series. There is a significant chance for bias because patients who were referred specifically for subclavian artery stenosis (with or without symptoms) may have had a more focused and potentially more accurate assessment. Arm pressures were measured only once. In general, when measuring blood pressure, 2 or 3 measurements are recommended. Obtaining pressure readings after the duplex study, and after a period of rest, may be more accurate as well.
Defining significant subclavian artery stenosis by duplex ultrasound can be problematic. We used duplex waveform criteria of a peak systolic velocity greater than 250 cm/s, poststenotic turbulence, and abnormal monophasic flow distally. Mousa and colleagues suggested that a peak systolic velocity threshold of 240 cm/s correlated well with a >70% diameter reduction. 11 On the contrary, while this may be more precise in detecting lesions that are causing symptoms, in some cases visualization is difficult. In addition, the presence of a subclavian artery stenosis at the >50% level has, as discussed, been correlated with identifying asymptomatic patients at risk for other vascular disease. The difficulties that may be encountered in accurately measuring peak systolic velocity also stress the importance of other, easier to obtain, assessments such as IBP differences in screening for this condition. A potential strength of this study is that this was a group of patients with unilateral focal subclavian artery pathology.
Conclusion
Because of the clinical importance of identifying subclavian artery stenosis, an AAI <0.9 appears to be a useful adjunct when screening patients, either in the primary care setting, the vascular surgery setting, or when performing a carotid duplex examination. In patients who have subclavian artery pathology and unilateral arm symptoms, the use of HAT may, in some settings, help define whether these lesions are the cause or not. An AAI <0.9 and IBP ≥15 or ≥20 mm Hg are effective in ruling out subclavian artery stenosis (>50% diameter reduction) and occlusion with or without symptoms. An HAT >100 milliseconds is an effective tool to confirm that arm symptoms are indeed related to subclavian artery pathology rather than other causes; however, there is not enough data to support this as an absolute criterion, and more work needs to be done in this area.
Brachial systolic pressure differences (whether described as IBP or AAI) are important measurements to collect when performing a carotid duplex scan. We recommend that patients undergoing a carotid duplex should, at the very least, have arm pressures and IBP recorded. Even in asymptomatic patients, identifying subclavian artery stenosis can prompt lifestyle modifications and further cardiovascular evaluation, as the risk of adverse cardiovascular events appears to be increased. In patients undergoing coronary or carotid interventions, this can be critical, and in patients being managed for hypertension, this is also important information, so the results of medical management can be more accurately tracked. In most cases, patients with arm symptoms who have been identified as having subclavian artery stenosis or occlusion will be candidates for revascularization. However, HAT may be potentially valuable to use when the clinical picture is confusing and may help to identify patients whose arm symptoms might indeed benefit from intervention.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.