
Abstract
Introduction:
Surveillance for endoleak after endovascular aortic aneurysm repair with computed tomography angiography has the associated risks of radiation exposure and nephrotoxic contrast agents. The purpose of this study was to evaluate the performance of contrast-enhanced ultrasound in the detection of endoleak post–endovascular aortic aneurysm repair.
Methods:
A single-center retrospective cohort study was performed evaluating patients with abdominal aortic aneurysm treated with endovascular aortic aneurysm repair between October 29, 2017 and April 21, 2021 and follow-up imaging with both computed tomography angiography and contrast-enhanced ultrasound. The sample included 35 imaging combinations in 28 patients. Positive and negative results for detection of endoleak by contrast-enhanced ultrasound were tabulated as true positive, false positive, true negative, and false negative compared to computed tomography angiography and conventional angiography. Sensitivity, specificity, positive predictive value, and negative predictive value of contrast-enhanced ultrasound were calculated.
Results:
Out of 35 imaging combinations, endoleak was detected in 24 cases by computed tomography angiography and in 23 cases by contrast-enhanced ultrasound. Using computed tomography angiography as the reference standard, contrast-enhanced ultrasound yielded 96% sensitivity, 100% specificity, 100% positive predictive value, and 92% negative predictive value for endoleak detection. In the 23 cases of endoleak detection by both contrast-enhanced ultrasound and computed tomography angiography, contrast-enhanced ultrasound discerned the correct endoleak type in all 23 cases, while computed tomography angiography identified the correct endoleak type in 20 cases (P = .2333).
Discussion:
Endoleak detection by contrast-enhanced ultrasound appears at least equivalent to computed tomography angiography. Some of the advantages of contrast-enhanced ultrasound in the surveillance of endoleak after endovascular aortic aneurysm repair include an avoidance of radiation, elimination of nephrotoxic contrast agents, reduction in costs, real-time imaging, discerning flow directionality, and visualizing endoleaks in regions previously embolized with coils/plugs/liquid embolic agents. Limitations include operator dependence and variables that obscure the visual field including obese body habitus. With these advantages and excellent comparison data, contrast-enhanced ultrasound should be considered as a first-line imaging modality for long-term surveillance of endoleaks after endovascular aortic aneurysm repair.
Conclusion:
Contrast-enhanced ultrasound is a safe and viable option for long-term surveillance post–endovascular aortic aneurysm repair.
Keywords
Introduction
Abdominal aortic aneurysm (AAA) is a potentially devastating medical condition, resulting in 1% to 3% of all deaths in males aged 65 to 85 years in developed countries. 1 Endovascular aortic repair (EVAR) is a commonly used, safe, and effective treatment option for patients with AAAs.2-5 Risks of EVAR include endoleak, stent-graft migration, infection, and graft limb thrombosis, among others. 6
Endoleak is the most common complication after EVAR and is often asymptomatic, seen in 15% to 25% of patients within the first 30 days postintervention.7,8 Timely detection of endoleak is of particular concern, as previous studies showed that the presence of endoleak may predict aneurysm rupture after EVAR. 9 Lifelong surveillance of EVAR is necessary to minimize risk of complications or device failure and monitor for progression of aneurysm growth. 10
Contrast-enhanced computed tomography angiography (CTA) is the current reference standard for imaging surveillance after EVAR.11,12 Although effective, lifelong surveillance with CTA exposes patients to repeated doses of radiation, nephrotoxic contrast agents, and is associated with substantial costs.13-15 Computed tomography angiography also provides limited information with regard to flow directionality and hemodynamics of endoleaks. 16 Recently, contrast-enhanced ultrasound (CEUS) has emerged as a viable alternative to CTA for long-term surveillance after EVAR. 17
Studies have indicated that CEUS may be diagnostically equivalent to CTA for detection of endoleak after EVAR, with comparable sensitivity and specificity.18,19 In 2012, the European Federation of Societies for Ultrasound in Medicine and Biology published guidelines recommending the use of CEUS for detection and surveillance of endoleak after EVAR. 20 Some institutions in Europe have already integrated CEUS in their protocols for EVAR surveillance21; however, this imaging modality has not yet seen widespread application for this purpose in the United States. Reliable imaging quality, avoidance of radiation, lack of nephrotoxic contrast agents, ability to detect changes in real time, and cost-effectiveness make CEUS a promising diagnostic tool in endoleak detection.12,16,22,23 The purpose of this study is to outline our results and accuracy in a single-center experience using CEUS for detection of endoleak after EVAR.
Methods
A single-center retrospective cohort study was conducted. After obtaining approval from the Institutional Review Board, all patients from October 29, 2017 to April 21, 2021 who had a history of AAA treated with EVAR and follow-up imaging with both CTA and CEUS examining for endoleak were identified for this study. Patients who had more than one contrast-enhanced CTA/CEUS combination were included, and each combination of imaging was recorded. A combination, or an event, was defined as one CEUS and one CTA imaging study which occurred within 1 year of one another. Patients who had surveillance imaging with only CEUS or only CTA were excluded from this study.
A Boolean search engine (Primordial; Primordial Design Inc, San Mateo, California) was used to identify patients who previously had CEUS with sulfur hexafluoride microspheres (Lumason®, Bracco, Milan) as a screening tool for endoleak surveillance post-EVAR. Prism Boolean search terms included “Contrast Enhanced Ultrasound” and aneurysm, “Lumason” and aneurysm, “CEUS” and aneurysm, and “CEUS” and AAA. IntelliSpace PACS Radiology (Philips, Amsterdam) was then used to identify those who were also screened with CTA. Data collected included date of EVAR, AAA diameter prior to EVAR, date of CTA, detection of endoleak on CTA, type of endoleak on CTA, date of CEUS, detection of endoleak on CEUS, type of endoleak on CEUS, as well as angiographic results. Patients in the study population who underwent an aortic angiogram for confirmed or suspected endoleak after CTA or CEUS were also identified. Additional data points were collected for these patients including the date of angiogram, detection of endoleak on angiogram, and type of endoleak on angiogram. All data were entered in an encrypted Microsoft Excel spreadsheet and stored in a locked computer on campus.
Our study population included a sample size of 35 events, or combination CTA/CEUS, in 28 patients. Of these, 22 patients had 1 event, 4 had 2 events, and 1 had 5 events. Contrast-enhanced ultrasound and CTA were used to evaluate variables including AAA size at presentation, aneurysm sac size at presentation, and aneurysm sac size at follow-up. Graft types included Gore Excluder (Gore Medical, Flagstaff, Arizona), Endurant II (Medtronic, Minneapolis, Minnesota), Talent (Medtronic, Minneapolis, Minnesota), Zenith (Cook Medical, Bloomington, Indiana), and AFX (Endologix, Irvine, California).
CEUS Imaging Technique
Prior to administering contrast, a baseline duplex ultrasound was performed to evaluate the entire abdominal aorta and its branches. The evaluation utilized gray-scale, color, and spectral Doppler imaging of the entire length of the aorta and iliac arteries including the endograft. Attention was paid to any suspected area(s) of endoleak using conventional color Doppler imaging on low-flow setup and microflow imaging when available. The maximum transverse aneurysm diameter was measured and documented. After gaining a baseline understanding of the patient’s anatomy using duplex ultrasonography, contrast was prepared and injected. The imaging timer started immediately after the injection was completed, and video clips were recorded as the enhancing agent filled the endograft. Any enhancement seen outside the endograft lumen leaking into the excluded aneurysm sac was carefully timed and documented. At our institution, we typically perform two injections of Lumason® with agitated saline. The first injection of this mix is given as a 2.5 mL dose. The initial recorded video may last up to 3 minutes and additional snapshots are then recorded and sent for review. Before administering a second dose of the mix to confirm the imaging findings, and to ensure that residual of the microbubbles of the first injection is destroyed, a series of high mechanical index ultrasound pulses is released into the tissue until no enhancement is displayed on the image. This is a special function called “Flash” found under the “Contrast” protocol setup. If this function is not available, the technologist may continue to scan using “high power” set up for a few additional minutes until no enhancement is displayed on the image. Next, a second dose of contrast (2.5 mL) is administered, and the process is repeated. The imaging timer is reset while the second injection is being administered.
Once contrast is administered, we can then discern the type of endoleak. Enhancement of a type I and type III endoleak is seen within the aneurysm sac at the same time that contrast becomes visible within the endograft lumen. In some cases, it may be difficult to appreciate the difference between a type I and type III endoleak solely based on contrast timing. However, in rare instances with contrast administration, defects may be appreciated in the walls of the endograft. In type II endoleaks, contrast is typically seen within the excluded aneurysm sac several seconds after contrast is seen filling the endograft lumen. The filling of the sac is in the delayed phase.
Statistical Analysis
Following data collection, positive and negative results for detection of endoleak by CEUS were tabulated as true positive (TP), false positive (FP), true negative (TN), and false negative (FN) as compared to those for CTA and angiogram. These results were organized in 2 × 2 tables and values for sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated. Additional comparisons were performed between the accuracy of the diagnostic angiogram compared with CEUS and CTA respectively as the reference standard. Again, TP, FP, TN, and FN were tabulated and using 2 × 2 tables, sensitivity, specificity, PPV, and NPV were calculated.
Furthermore, a study was then conducted to compare the type of endoleak identified between CTA and CEUS. Patients from the original sample who had an endoleak detected on both the CTA and CEUS were included. Then, each CTA/CEUS combination was given a concordant or discordant indicator. Discordant data points underwent further scrutiny by an independent reviewer (BJS, BRF) to understand which imaging method correctly identified the endoleak type. A Fisher’s exact test was performed, and associated P values were recorded. P values less than .05 were considered statistically significant.
Results
Study Population
Cohort characteristics can be seen in Table 1.
Cohort Characteristics.
Note. EVAR = endovascular aortic aneurysm repair; AAA = abdominal aortic aneurysm; CEUS = contrast-enhanced ultrasound; CTA = computed tomography angiography.
CEUS Compared With CTA
Out of 35 screening combinations, endoleak was detected in 24 cases by CTA and in 23 cases by CEUS. Using CTA as the reference standard, there was 1 FN, 0 FPs, 11 TNs, and 23 TPs. Contrast-enhanced ultrasound yielded a sensitivity of 96%, specificity of 100%, PPV of 100%, and NPV of 92% when compared against CTA.
Angiography Compared With CEUS and CTA
In 16 of the 35 events, the patients also underwent an aortic angiogram. Using CEUS as the reference standard, there were 2 FNs, 1 FP, 1 TN, and 12 TPs. In this case, angiography yielded 86% sensitivity, 50% specificity, 92% PPV, and 33% NPV. When using CTA as the reference standard, there were 2 FNs, 0 FPs, 1 TN, and 13 TPs. In this case, angiography yielded 87% sensitivity, 100% specificity, 100% PPV, and 33% NPV.
Comparison of Endoleak Detection Type
In 23 of the 35 cases, both CEUS and CTA identified an endoleak. Within this set, CTA detected 3 type I endoleaks, 19 type II endoleaks, 0 type III endoleaks, and 0 type IV endoleaks. Two of the 23 CTAs were unable to discern the type of endoleak. Contrast-enhanced ultrasound detected 5 type I endoleaks, 18 type II endoleaks, 1 type III endoleak, and 0 type IV endoleak. After imaging was read by an independent reviewer, it was found that there were 20 concordant and 3 discordant endoleak reports between imaging modalities.
One discordance was found because the CTA appeared to show filling of the aortic sac which was believed to be from a feeding lumbar artery supplying the sac posteriorly. This indicates a type II endoleak. However, CEUS and angiography showed a definitive type III endoleak via the left iliac limb leak through the graft material (Figure 1).
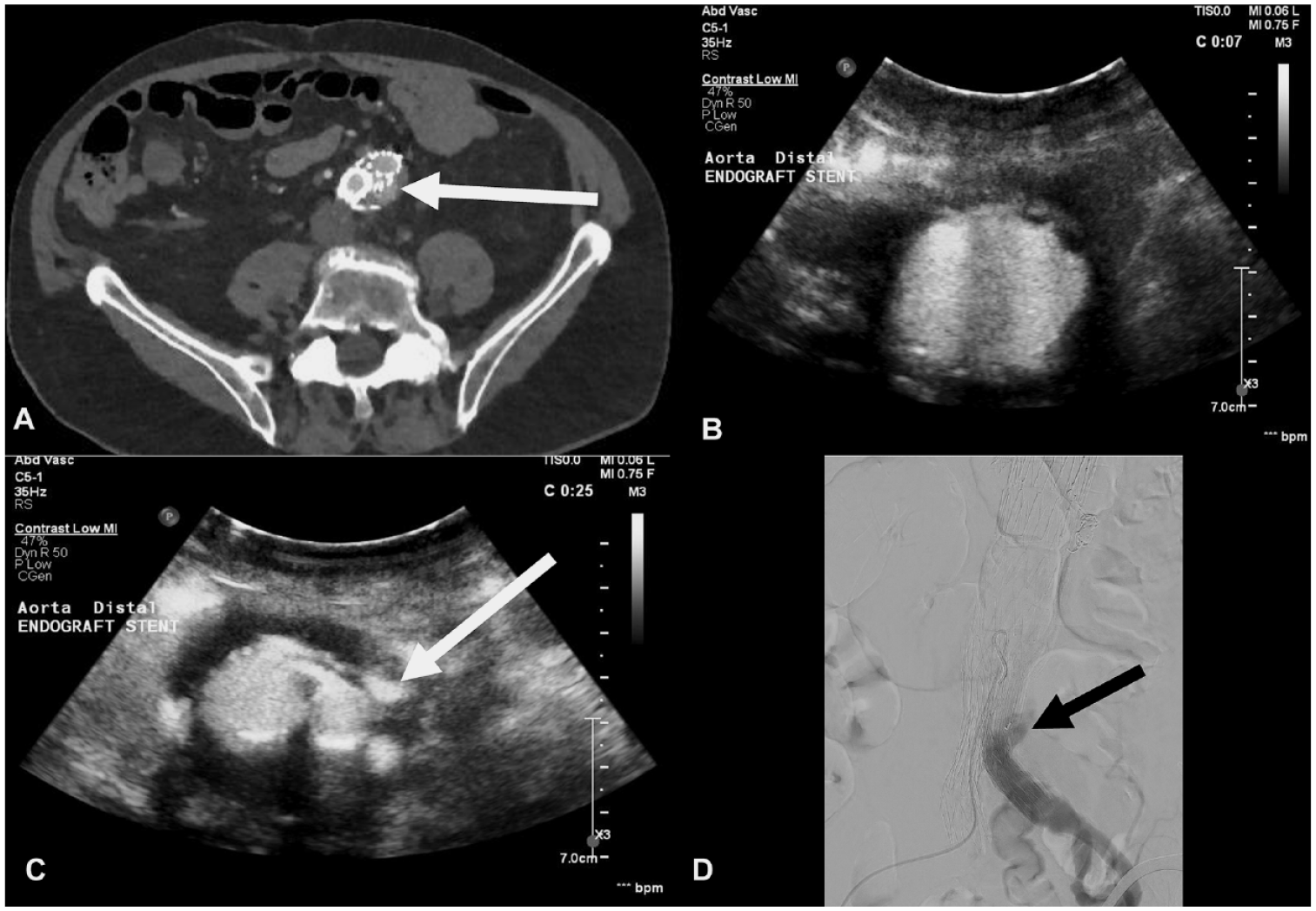
Images of CTA, CEUS, and CA with evidence of endoleak. (A) Filling of the aortic sac external to endograft believed to be from a feeding artery supplying the aneurysm posteriorly on CTA (arrow). (B) CEUS showing filling of the proximal endograft. (C) Lower, early filling of the sac via the left common iliac artery through the graft, consistent with a type III endoleak (arrow). (D) Type III endoleak from the left common iliac artery was confirmed on angiogram.
Another discordance was identified because the abdominal CTA showed an opacification of the posterior aortic sac at the region of the superior aspect of the graft, which could be due to a type I or type II endoleak. The CEUS, however, distinguished that the endoleak is consistent with a type IA endoleak (Figure 2).
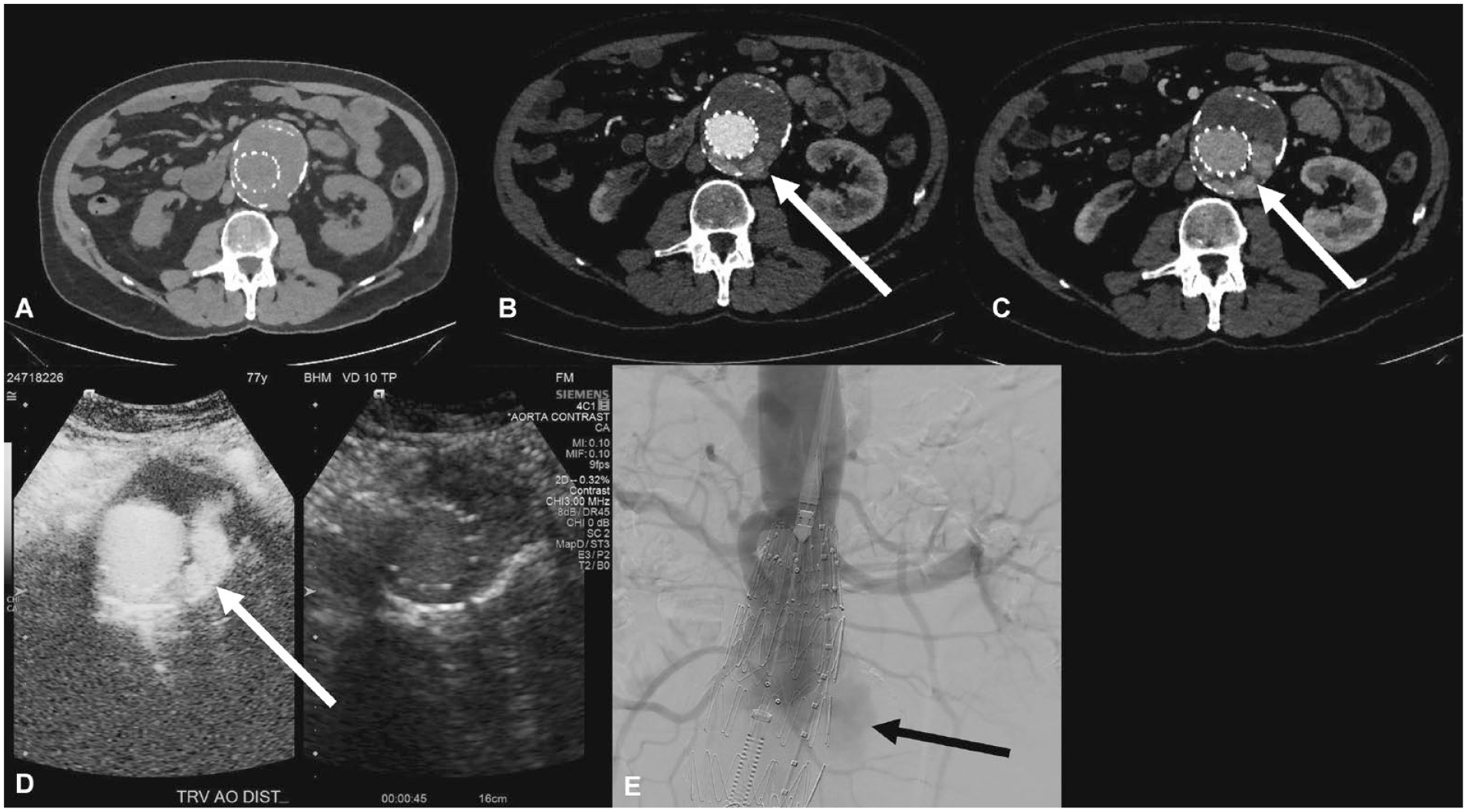
Images of CTA, CEUS, and CA with evidence of endoleak. (A) Precontrast. (B) Arterial phase. (C) Delayed phase. CTA shows opacification of the posterior aortic sac at the region of the superior aspect of the graft. This could be due to a type I or type II endoleak. (D) CEUS shows filling of the excluded sac and within the superior aspect of the graft in early phase of the acquisition consistent with type IA endoleak. (E) Angiogram confirms type IA endoleak.
The final discordance in the data set was identified because the CTA showed opacification of the aortic sac outside of the graft on the arterial phase, which could be due to a type I, type II, or type III endoleak. The CEUS, however, showed immediate filling of the sac outside the stent-graft, suggesting a type I and/or a type III endoleak (Figure 3).
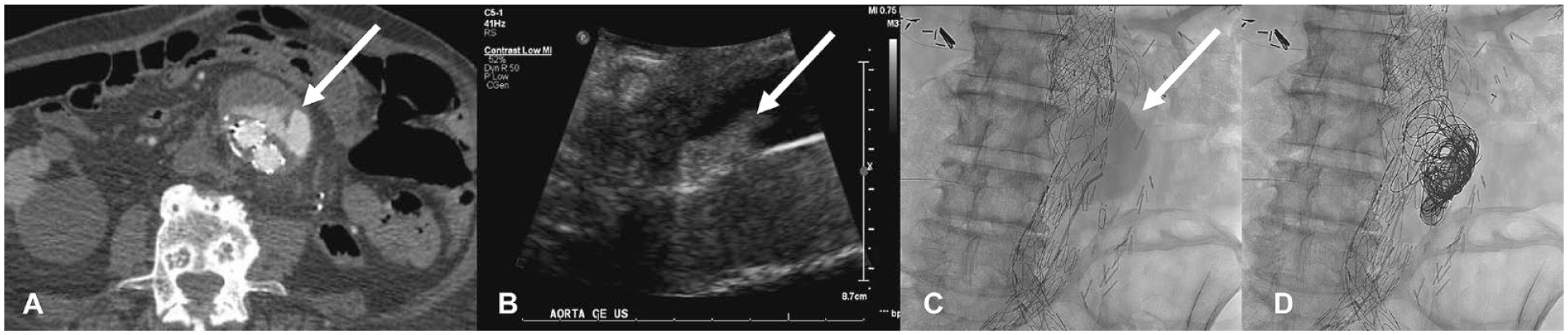
Images of CTA, CEUS, and CA with evidence of endoleak. (A) Abdomen and pelvis CTA shows opacification of the aortic sac outside of the graft on arterial phase, which could be due to type I, type II, or type III endoleak. (B) CEUS shows filling of the sac outside the stent-graft, simultaneously with the graft, suggestive of type I endoleak or a type III endoleak. (C) Angiogram confirms type III endoleak, which was successfully treated (D) with coil embolization and relining of the graft.
In one discordance that was excluded from our cohort, the CTA showed a significant streak artifact from previous Onyx (Medtronic, Minneapolis, Minnesota) embolization, obscuring visualization of an endoleak on CTA imaging. In this case, CEUS was used to correctly identify the endoleak and its associated type (Figure 4).

Images of CTA and CEUS. (A) CTA of the abdomen and pelvis shows significant hyperdense artifact from embolization material; this makes it infeasible to evaluate for endoleak. In the same patient, (B) transverse. (C) longitudinal. CEUS shows delayed filling of the aortic sac posteriorly, consistent with a type II endoleak. Note the lack of artifact created by the embolization material.
After scrutiny of the discordant imaging sets, it was found that CEUS discerned the correct endoleak type all 23 times, while CTA identified the correct endoleak type in 20 out of 23 events. These results, however, were not statistically significant (P = .2333) in this sample.
Discussion
Due to the need for lifetime surveillance of endoleak after EVAR and taking into consideration the accuracy of CEUS, it is important to highlight the benefits of CEUS as a sustainable imaging modality for long-term surveillance. These include the avoidance of radiation and nephrotoxic contrast agents, as well as reduction in cost.13-15 Some other considerations regarding endoleak detection include CEUS’s ability to visualize the aorta and its main branches in real time, to visualize endoleak after interventions with coils/plugs/liquid embolic agents, and to discern flow velocities and directionality. 21 These benefits can help ameliorate several of the shortcomings of CTA.
Previously published literature has shown that CEUS is at least equivalent to CTA with regard to endoleak detection and classification. A systematic review and meta-analysis by Harky et al published in 2019 examined 1773 patients with a history of EVAR across 18 studies and showed no significant difference between CEUS and CTA in the detection rate of endoleak types I-III on follow-up surveillance. 23 This study showed that CEUS had a significantly higher sensitivity in detection of all endoleak types compared with CTA (98% vs 83%, P = .001), and showed no significant difference in specificity between CEUS and CTA (93% vs 99%, P = .28). 23 A prospective study by Bredahl et al on 278 patients with a history of EVAR showed that CEUS and CTA were diagnostically equivalent with regard to endoleak detection rates. They suggest that CEUS may replace CTA in EVAR surveillance programs. 18 A retrospective study by Chisci et al on 880 patients with a history of EVAR and at least 1 year of follow-up showed that CEUS surveillance yielded 100% sensitivity and 100% specificity in detection and classification of endoleaks. 21 In this study, there were no instances of FPs or FNs with CEUS, while CTA misclassified 2 type II endoleaks both of which were correctly identified and classified by CEUS. 21
In our study, CEUS was found to have a sensitivity of 96%, specificity of 100%, PPV of 100%, and NPV of 92% with CTA as the reference standard. Given these results, we found that CEUS was at least equivalent to CTA in detection of endoleak post-EVAR. When analyzing cases in which both CEUS and CTA detected an endoleak, CEUS discerned the correct endoleak type in 23 out of 23 events, while CTA was correct in 20 out of 23 cases. A larger sample size would be required to establish significance behind CEUS’s ability to better discern endoleak type than CTA.
In our experience, endoleak detection by CEUS appears superior. In one case, a patient underwent multiple endoleak interventions due to his CTA showing a recurrent type II endoleak. The use of CEUS helped determine that the correct endoleak was a type III endoleak, which ultimately altered the treatment course. Although in this case the patient’s endoleak required further intervention, CEUS was pivotal in appropriately directing the patient’s treatment plan to accurately address the endoleak. Since the CEUS showed a type III endoleak arising from the left iliac limb, we were able to plan our approach to target and reline the left iliac limb of the graft. This prevented us from performing other approaches such as translumbar access to evaluate for a type II endoleak. This case demonstrates one example of how CEUS can make a significant impact with regard to directing appropriate medical therapy for patients with endoleak after EVAR.
While CEUS has many benefits, this imaging modality entails some limitations. The use of CEUS is operator dependent, thereby limiting the visualization of endoleaks in the hands of an inexperienced sonographer. In one CEUS screening within our cohort, the endoleak was missed because it was above the anatomical area investigated by the sonographer. Other limitations include obese body habitus, ascites, gaseous abdominal distension, and the patient’s ability to cooperate with the exam. Also, the relative inability to detect fractures or separation of the metal skeleton from the endograft is a significant factor. 21
Limitations of this study include a small patient sample size, lack of standardization of follow-up, incomplete medical records, and evolution of technique. Follow-up visits were scheduled on a case-by-case basis with variable timing and CEUS frequency. Future studies may improve upon these limitations by including a larger sample size and standardizing the image technique with regularly scheduled patient follow-ups throughout the duration of the study.
Given the safety, accuracy, and reduction in costs, we believe that CEUS should be considered as a first-line imaging modality for long-term surveillance of endoleaks after EVAR. In our practice, CEUS is now used as the primary modality of imaging follow-up. Computed tomography angiography is used for additional trouble-shooting or preplanning prior to any needed intervention.
Conclusion
Contrast-enhanced ultrasound is a safe, accurate, and cost-effective imaging modality to evaluate for endoleaks after EVAR. Given the reliable imaging quality, avoidance of radiation, lack of nephrotoxic contrast agents, ability to detect changes in real time, and cost-effectiveness, CEUS is a viable option for long-term surveillance after EVAR.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: James F. Benenati, MD is the Chief Medical Officer of Penumbra, Inc.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Baptist Health South Florida IRB (approval protocol number: 1721247).