
Abstract
Introduction:
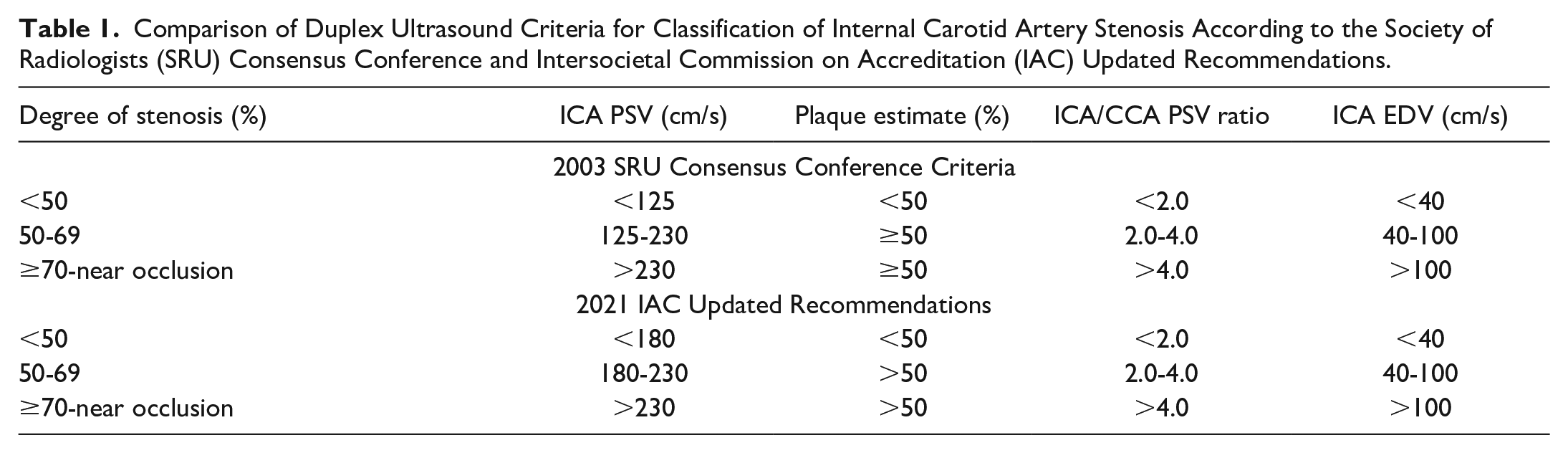
In 2021, the Intersocietal Accreditation Commission (IAC) introduced modified criteria for carotid duplex interpretation based on peak systolic velocity (PSV) and PSV ratio. The most significant change compared to the 2003 Society of Radiologists in Ultrasound (SRU) criteria involved re-defining the thresholds for <50 and 50% to 69% stenosis ranges. Patients identified in <50% vs 50% to 69% ranges may face different disease severity assignments, variable surveillance protocols, medical management approaches, and recommendations for intervention. Facilities may experience altered payment coverage, issues of staff re-training, and questions from referring physicians regarding patient treatment and disease management expectations. The objective of this study was to assess the impact of re-defining these stenosis ranges using the 2021 IAC criteria vs the SRU criteria.
Methods:
Anonymized patient data from carotid duplex examinations were collected as part of an internal laboratory quality improvement strategy. These data were analyzed in an electronic database using the IAC and SRU threshold criteria to determine the degree of carotid stenosis. Patients with normal arteries, unilateral studies, or complete occlusions were excluded.
Results:
Of the 1000 patients considered, 850 met the eligibility criteria. Using PSV: for the right carotid, 242 (28.5%) showed a change and 608 (71.5%) showed no change in stenosis classification; for the left carotid, 228 (27%) showed a change and 622 (73%) showed no change. All changes were a downgrading of disease to <50% stenosis. Using PSV ratio: for the right carotid, re-assignment of 53 (22% of changed, 6% of total cohort); for the left carotid, re-assignment of 48 (21% of changed, 5.6% of total cohort). All changes resulted in re-assignment to the 50% to 69% stenosis category.
Conclusions:
Implementation of the IAC criteria resulted in patients being re-assigned to lower stenosis categories (27% for PSV and 21% for PSV ratio). The impact of these changes on patient care and facility logistics needs careful consideration.
Keywords
Introduction
The use of clinically relevant ultrasound interpretation criteria is critical to appropriate reporting of carotid studies in the vascular laboratory setting. The 2003 Society of Radiologists in Ultrasound (SRU) Consensus Criteria are widely used for carotid duplex ultrasound interpretation.1,2 The Intersocietal Accreditation Commission (IAC) has recently published alternative criteria. 3
Prior to the North American Symptomatic Carotid Endarterectomy Trial (NASCET), 4 a variety of published carotid interpretation criteria, such as the Radiographics (Bluth) 4 or University of Washington (Strandness) 5 criteria, were widely used. Furthermore, many laboratories used internally developed and validated local criteria. The NASCET findings are widely accepted as the definitive clinical guidance for managing patients with symptomatic carotid disease.4,6-10 However, the NASCET used a definition of stenosis and diagnostic ranges that were not consistent with the previously used interpretation criteria.4-6 As a result, updated clinically relevant criteria were required. In response to this, the SRU convened a consensus panel in 2003 to develop relevant carotid reporting criteria consistent with clinically important definitions and ranges. 1
The SRU recommendations have been widely accepted and generally have replaced other criteria in most laboratories in North America.1,2,7,11,12 The findings have been validated in clinical use and in a variety of trials and widely endorsed.11-17 An IAC report suggests that the SRU criteria are being more widely implemented, 2 although other criteria or internally validated criteria have been accepted by IAC for vascular laboratory accreditation. 15 The IAC and others have recognized concerns about the 2003 SRU Consensus Criteria.2,3,18-22
The IAC conducted their own study and published alternative recommendations in 2021. 2 The IAC study included a series of patients who underwent both carotid duplex ultrasound and a catheter carotid angiogram and used pre-determined “optimized” sensitivity, specificity, and other parameters. This study, although supported by the IAC in 2021, 15 has not been independently validated, and the clinical impact of its implementation has not been determined.
The implementation of new guidelines can be difficult with issues of acceptance, perceived need for practice change, timelines in modifying protocols, staff time, and monetary costs needed to implement and internally validate the new recommendations. 23 Knowledge translation principles can be applied to understand these issues.24,25 Approximately 50% of developed guidelines for clinical practice are implemented and many of these do not receive widespread uptake.22,23 Continuous improvement strategies, as applied in a quality improvement/assurance approach, can guide implementation strategies and document impact on clinical practice. 25 However, the impact an accreditation-mandated strategy is not well-studied and is unclear. 2
Study Objective and Aims
The main objective of this study is to determine whether changing carotid interpretation criteria from the 2003 SRU Consensus Criteria to the 2021 IAC Carotid Criteria will result in a reclassification of degree of carotid stenosis in individual patients. The differences between the 2 sets of criteria for the most relevant categories are presented in Table 1. The specific aims of this study are: (1) to compare the SRU Consensus Criteria and the IAC Carotid Criteria using real-world data and (2) assess the impact of any differences in interpretation for potential change in classification of degree of stenosis.
Comparison of Duplex Ultrasound Criteria for Classification of Internal Carotid Artery Stenosis According to the Society of Radiologists (SRU) Consensus Conference and Intersocietal Commission on Accreditation (IAC) Updated Recommendations.
Methods
This study is a retrospective review performed in a quality improvement format using previously collected carotid velocity data. All data sets were anonymized and held in a secured electronic file. The data set utilized for this study was defined by the following parameters:
Inclusion criteria are as follows:
Velocity data from bilateral carotid duplex studies for atherosclerotic disease.
Studies with interpretation reports completed and signed off prior to December 31, 2021.
Exclusion criteria are as follows:
Complete occlusion of the internal carotid artery.
Common carotid artery occlusion, common carotid artery stenosis, vertebral artery occlusion, or subclavian steal.
Unilateral or incomplete studies (ie, missing a velocity from any of the required IAC carotid anatomic sites).
Normal arteries (normal velocity parameters and no visible disease present).
Previous carotid artery intervention (endarterectomy or stenting).
The framework for this study followed a quality improvement approach consisting of:
1. Carotid duplex examinations were retrospectively pulled in sequence from a single IAC accredited vascular laboratory in the United States.
2. Velocity parameters from these studies were analyzed independently for degree of stenosis using the 2003 SRU Consensus Criteria and the 2021 IAC Carotid Criteria.
a. Using the SRU criteria: peak systolic velocity (PSV) and PSV ratio were applied to all patients.
b. Using the IAC criteria: PSV was applied to all patients and the PSV ratio was applied selectively as recommended.
3. The interpreted degree of stenosis determined using the SRU and IAC criteria were compared and tabulated for agreement and disparities.
To determine whether the calculations and the database could be used to replicate real world analysis, data from 1000 consecutive patients were collected, inclusion and exclusion criteria were applied, and the data set from the resulting patients was analyzed.
Data Analysis
Analysis was done based on the involved arteries and the patient. All arteries were interpreted by the PSV and PSV ratio as recommended by the SRU and IAC carotid criteria publications, and the interpretation results were tabulated. Both descriptive approaches were applied to characterize concordance or variance (disparity) in results using common parameters. Each of the interpretation categories were assayed: <50%, 50% to 69%, and 70% to 99% stenosis.
Results
Of the 1000 consecutive patients screened, data from 850 patients met the inclusion criteria. All patients had bilateral studies, resulting in 1700 carotid arteries available for the study. Using the PSV for the interpretation of the 850 patients, 242 (28.5%) had a change in the interpretation of the right carotid and 608 (71.5%) showed no change in classification. On the left side, 228 (27%) demonstrated a change and 622 (73%) had no change in the results. All changes resulted in a decrease in the degree of assigned stenosis from the 50% to 69% range based on the SRU criteria to <50% based on the IAC criteria. Additional analysis was done by including the PSV and PSV ratio, as recommended in the IAC document. Inclusion of the PSV ratio resulted in the re-assignment of 53 patients (22% of changed, 6% of total cohort) for the right side and 48 (21% of changed, 5.6% of total cohort) on the left side. These changes reassigned these patients back to the higher 50% to 69% category. The clinical impact on patients as defined by each interpretation was determined with 27% re-assigned by PSV and 21% by the combination of PSV and PSV ratio.
Discussion
Atherosclerotic carotid artery disease is characterized by plaque with or without stenosis; complete occlusion can also occur. The degree of carotid stenosis is used as a surrogate for the risk of transient ischemic attacks or stroke, although plaque characteristics and other factors are also considered to be important in some individuals. The clinically relevant ranges of stenosis used in the United States for recommending surveillance, medical treatment, or surgical interventions are defined by the findings of the NASCET for symptomatic patients.4,6-10 Guidance for surveillance or intensive medical management is taken from this study and others.8,26
Clinical decision-making is defined by the NASCET with surgical intervention recommended in symptomatic patients with an acceptable risk profile and a 50% to 69% or 70% to 99% stenosis.4,7,8,12,13,17 For the symptomatic patient with a 70% to 99% stenosis, the risk of stroke is approximately 27% at 18 months, and the benefit of surgery is reflected in the number needed to treat (NNT) of 6. For the patient with a 50% to 69% stenosis, the risk is approximately 8% and the benefit is positive with an NNT of 12. Most patients with the higher-grade (70%-99%) stenosis would be offered intervention; selected patients with the lower-grade (50%-69%) stenosis would also be considered for intervention. 8 For those not having intervention, optimal medical management and close surveillance would be recommended.8,26 There is no benefit from intervention for patients with <50% stenosis or a complete internal carotid occlusion; variable levels of medical treatment and ultrasound surveillance may be offered to these patients.4,26 In some situations, surveillance options may be altered by insurance coverage for <50% stenosis. From a clinical perspective, identifying patients at risk who would benefit from intervention is a priority.
Identifying the range of carotid stenosis with an acceptable degree of accuracy is the goal of carotid duplex ultrasound; however, many factors influence this goal. Carotid duplex ultrasound studies require a qualified and experienced technologist using high-quality equipment and following a standardized protocol.27-29 Training and credentialing of vascular technologists are regulated through the American Registry for Diagnostic Medical Sonography (ARDMS) and other bodies. 30 Multiple acceptable protocol standards are available, including those from the IAC, Society for Vascular Ultrasound (SVU), and others.27-29 Facility accreditation, through the IAC, American College of Radiology (ACR), and others,15,28,31 has been shown to help promote quality testing. Interpretation of the data obtained from the carotid duplex study leads to the vascular laboratory report that should guide management.31,32 Therefore, establishing appropriate criteria and encouraging wide-spread and consistent use should promote quality patient care.3,8,33
Although there is a frequent call for accurate reporting and concern regarding varying reporting criteria,1-3,8,12,14,15,18-22,34 it is recognized that there is no “magic number” that will define the degree of stenosis.1,3,8,34,35 The SRU Consensus Criteria require consideration of the PSV, PSV ratio, and B-mode image in all patients to determine degree of stenosis. 1 The IAC Criteria rely on the PSV as a stand-alone parameter and suggest addition of the PSV ratio in situations of uncertainty. 3
Furthermore, ultrasound findings can be confounded by patient factors such as cardiac output, arrhythmia, multiple or tandem lesions, tortuous arteries, and plaque characteristics. Technical factors such as placement and size of the Doppler sample volume, angle correction, and appropriate machine settings, can affect the data. Comparison to a “gold standard” such as computed tomography (CT) or catheter angiography and patient selection for such assessment can also be confounded by the inaccuracy of those studies. Selection of ultrasound velocity ranges and ratios to address accuracy, consistency with reported studies, clinical practice, and confounding variables, requires careful consideration.1,3,16,36-38
Attempts to define optimal criteria based on statistical cut-points for sensitivity, specificity, accuracy, and other parameters are also open to debate and interpretation.1,3,11,14,22,36,38 A judgment to increase sensitivity will yield a higher percentage of positive studies, and fewer patients with disease will be missed. Some patients, however, may be classified as having disease that is more severe. As a corollary of this, the specificity will be decreased, meaning some patients with no disease will be characterized as having disease.
The SRU Consensus Criteria were developed through a review of the literature and discussion amongst an expert panel. 1 The SRU panel chose lower PSV and PSV ratio thresholds to identify more patients who might benefit from intervention through a higher sensitivity. This, of course, decreased the diagnostic specificity. The SRU paper addressed the clinical relevance of the criteria and identified specific topics for further study and discussion.
The IAC Carotid Criteria were developed by aiming for specific statistical cut points based on ultrasound and angiographic data on a limited number of patients. 3 The IAC study promotes higher specificity and overall accuracy by choosing higher PSV values or by the addition of the PSV ratio, resulting in decreased sensitivity. Hence, there is the potential for “missing” some patients with significant disease. The clinical impact was not specifically addressed in the IAC paper. 3
The study presented here confirms that fewer patients will be identified with 50% to 69% stenosis (a group that may benefit from more aggressive treatment) with 27% of patients being re-classified by PSV using the IAC Carotid Criteria as compared to the SRU Consensus Criteria. The addition of the PSV ratio partially ameliorates this, with 21% being re-classified. In practice, an additional cadre of 21% to 27% of patients would be managed with less frequent surveillance and standard medical risk factor management based on the IAC Carotid Criteria, as opposed to being offered intervention or more aggressive medical management and surveillance, as may have been considered with the SRU Consensus Criteria.
It is recognized that uptake of guidelines and standards to improve patient management are frequently difficult to implement.23,38,39 In the setting of the use of the carotid criteria, local factors, historical clinical approaches, published guidelines, and practitioners’ comfort level may all play a role. The cost of retraining and modification of systems should not be a major factor but may present a barrier. Reassignment of patients from one disease category to another, with no real change in their disease, may cause confusion. Potential misunderstanding on the part of the referring physician and the patient will need to be addressed. Billing or reimbursement issues may also depend on the category of disease; hence, coverage of surveillance or intervention should be investigated. Effective implementation will require a broad-based approach with careful consideration and education. 9
Generally, accrediting agencies have promoted standards and allowed for individual variations within acceptable margins.2,28 The impact of an accrediting body mandating interpretation criteria separate from clinical considerations is not known. Although the IAC survey in 2012 showed that 67% of respondents favored an IAC-mandated interpretation schema, there was no supporting data identifying the potential impact of such a strategy. 2
Conclusion
The IAC has developed criteria for the interpretation of carotid duplex studies that address pre-determined statistical cut-off points for sensitivity, specificity, and other parameters. The recommended approach is based on a limited sample of duplex ultrasound and angiographic findings and does not address the potential clinical impact of these criteria. Compared with the SRU Consensus Criteria, the IAC Carotid Criteria resulted in 21% to 27% of patients being re-assigned to the <50% stenosis category by PSV and PSV ratio thresholds. The impact of these changes on patient care and facility logistics needs further study and careful consideration.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article:
DLW—Principal Investigator, Society for Vascular Ultrasound, Vascular Laboratory Research Grant, January 2023. Principal investigator, Canadian Society for Vascular Surgery, Clinical Investigator Award 2022. Co-author, SRU Carotid Consensus 2003.
DMW—Co-investigator, Society for Vascular Ultrasound, Vascular Laboratory Research Grant January 2023. Co-investigator, Canadian Society for Vascular Surgery, Clinical Investigator Award 2022. Journal for Vascular Ultrasound Editorial Board Member.
EMW—Co-investigator, Society for Vascular Ultrasound, Vascular Laboratory Research Grant, January 2023. Co-investigator, Canadian Society for Vascular Surgery, Clinical Investigator Award 2022. Paid employee MAP-Centre for Urban Solution Unity Health Toronto, Toronto, ON, Canada.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.