
Abstract
Introduction:
Transcranial Doppler (TCD) has been used to identify microembolic signals (MES) in individuals with carotid atherosclerosis (CAS). The MES are hypothesized to originate from unstable carotid plaque and have been identified in symptomatic and asymptomatic individuals with CAS. The purpose of this study is to examine the relationship of clinical risk factors for stroke (CRFs) and the presence of MES in patients with advanced CAS.
Methods:
Participants scheduled for carotid endarterectomy (CEA) (>60% stenosis NASCET and ACAS Criteria) were preoperatively evaluated for CRFs and the presence of MES with TCD. Kendall tau correlation coefficients, Pearson χ2, and logistic regression analysis were used to examine the relationship between MES and CRFs.
Results:
Participants (n = 89) had a median (interquartile range) age of 71 (13) years, 30 (33.7%) were female, and 53 (59.6%) were symptomatic. Microembolic signals were detected in 32 (36%) participants. There was significant evidence of association between MES with older age (P = .026) and male sex (P = .007). No other clinical variables showed significant association with MES (all P-values > .05). Logistic regression demonstrated that a model including age (P = .018), sex (P = .013) and hyperlipidemia (P = .083) was significantly associated with the presence of MES (P = .001).
Conclusion:
Microembolic signals were associated with older age and male sex in a cohort with advanced carotid atherosclerosis. Symptomatic status was not a predictor for MES in this cohort, suggesting that plaques in both symptomatic and asymptomatic individuals have the ability to release microemboli, highlighting the need for further work to be done to identify unstable plaques.
Introduction
Every year in the United States, over 795 000 people have a stroke, with over 75% of these cases being a first-time event. 1 Ischemic etiologies account for approximately 87% of all strokes. 1 Between 2017 and 2018, the stroke-related healthcare cost in the United States reached nearly $53 billion, including the cost of healthcare services, stroke-related medications, and missed days at work. 1 It is estimated that 5 silent strokes go unnoticed for every clinically recognized stroke in the United States, totaling up to 11 million cases of silent infarcts per year.2-4
Silent stroke is most often detected incidentally on imaging, and although these patients do not present with the classic stroke signs and symptoms, they may suffer from an increased risk for future cerebrovascular events and cognitive decline.3,5-8 In addition, the risk of cognitive decline due to a clinical stroke has been shown to be significantly amplified in patients with a history of silent infarcts. 7 Therefore, it is of great clinical interest to establish a screening tool for identifying patients at risk of subclinical stroke to address their modifiable risk factors.
Carotid atherosclerosis (CAS) is a well-established risk factor for ischemic stroke. The proposed mechanism for stroke in this patient population involves cerebral ischemia due to carotid artery stenosis or occlusion, and microemboli released from unstable plaques causing distal ischemia.2,6,9,10 The detection of these microemboli has been made possible by utilizing transcranial Doppler (TCD) which captures them as microembolic signals (MES), also known as high-intensity transient signals (HITS). 2 Studies have demonstrated that advanced CAS is associated with plaque instability and increased microembolism in both symptomatic and asymptomatic patients.6,11 This could explain why both symptomatic and asymptomatic individuals with advanced CAS may suffer from increased cognitive decline, especially in executive function, compared to control groups.5,6,12
This study sought to examine the relationship between the demographic and clinical characteristics of patients with advanced CAS and the presence of MES on TCD monitoring. Examining this relationship may provide further information for identifying subgroups of patients that are at highest risk for future stroke and/or cognitive decline.
Methods
Participants
Eighty-nine (89) participants with advanced CAS (>60% stenosis) were recruited in the University of Wisconsin Atherosclerotic Plaque Study Structural Stability of Carotid Plaque and Symptomatology (NIH funded study: R01 NS064034 PI: R. Dempsey). All participants were evaluated by a board certified neurosurgeon and met criteria for clinically indicated carotid endarterectomy (CEA); >60% stenosis of the carotid artery based on the North American Symptomatic Carotid Endarterectomy Trials (NASCET 1991) 13 criteria and Asymptomatic Carotid Artery Stenosis (ACAS 1995) 14 . This study was approved by the University of Wisconsin Health Sciences Institutional Review Boards, and all participants provided informed consent to participate.
Medical History
Past medical history, family history, and social history were extracted from the medical chart and study database for each participant. Cardiac embolic risk factors were categorized as low and high according to the Guidelines for the Use of Echocardiography in the Evaluation of a Cardiac Source of Embolism. 15 Participants were considered high-risk or low-risk for cardiac embolism if they had any of the high-risk or low-risk conditions as described by Saric et al. 15 Percent stenosis was determined by medical imaging (computed tomography angiography, ultrasound, or magnetic resonance angiography). Three participants had CAS reported as a range; the average of the minimum and maximum was used in those cases. Five patients participated in the study twice for bilateral, clinically indicated CEA. In those cases, the data from the second presentation were excluded.
Transcranial Doppler and Identification of MES
Transcranial Doppler was performed for all participants within 30 days before undergoing CEA. The TCD examinations were performed with the SONARA Digital Bilateral Systems Transcranial Doppler systems (Natus, Middleton, Wisconsin) using 2.0-MHz transducers. Two transducers were used simultaneously over the trans-temporal window to record the Doppler signals from the left and right middle cerebral arteries and were monitored for 60 minutes (range 14-60 minutes, early termination of monitoring was mostly due to discomfort with the TCD helmet). In 12 participants, only one side was monitored due to lack of a TCD window on the other side. Microembolic signals were identified using the emboli detection software on the SONARA Digital Bilateral Systems Transcranial Doppler system. The MES were distinguished from artifacts using the criteria defined by the Consensus Committee of the Ninth International Cerebral Hemodynamic Symposium: (1) high-intensity signal, (2) unidirectional, (3) short duration (<300 ms), and (4) audible noise (for example a chirp or thud). The complex mode was used to identify high-frequency oscillations associated with circulating emboli. A blinded physician reviewer and 2 observers reviewed all MES and distinguished those suggestive of microemboli from artifacts based on meeting at least 4 out of the 5 criteria mentioned above. The MES were recorded for both surgical and nonsurgical sides. The TCD monitoring time was monitored with the TCD system and a wall clock. For this paper all individuals with TCD monitoring performed for any time period were included.
Statistical Analysis
Statistical analysis was performed using SPSS software, Version 27.0 (IBM Corporation, Armonk, New York). Kendall tau correlation coefficients were used to examine the relationship between continuous clinical variables (age, body mass index, systolic blood pressure [SBP] and diastolic blood pressure [DBP], percent CAS) and the binary presence/absence of MES. Pearson χ2 test was used to compare categorical clinical variables with the presence/absence of MES. Logistic regression analysis with backward selection was used to examine the relationship between a dependent variable (presence/absence of MES) and multiple independent continuous and categorical clinical variables.
Results
Baseline Characteristics
Eighty-nine participants were included in this study (Table 1). The participants had a median (interquartile range [IQR]) age of 71 (13) years old, 33.7% were female, and 96.6% were white. There were 53 participants with symptomatic CAS (59.6%) based on their history of ipsilateral stroke (for example, symptoms of speech and/or motor deficits) or transient ischemic attack as determined by a neurosurgeon, 17 participants with a prior history of contralateral CEA, and 63 participants with a history of a cerebrovascular event both ipsilateral or contralateral to the CAS. Table 1 provides a summary of participants’ baseline characteristics. The majority of patients were on statin therapy (73%) and aspirin (86.5%).
Demographic and Clinical Characteristics of the Participants. Table 1a Contains the Continuous Variables and Table 1b Contains the Categorical Variables (n = 89).
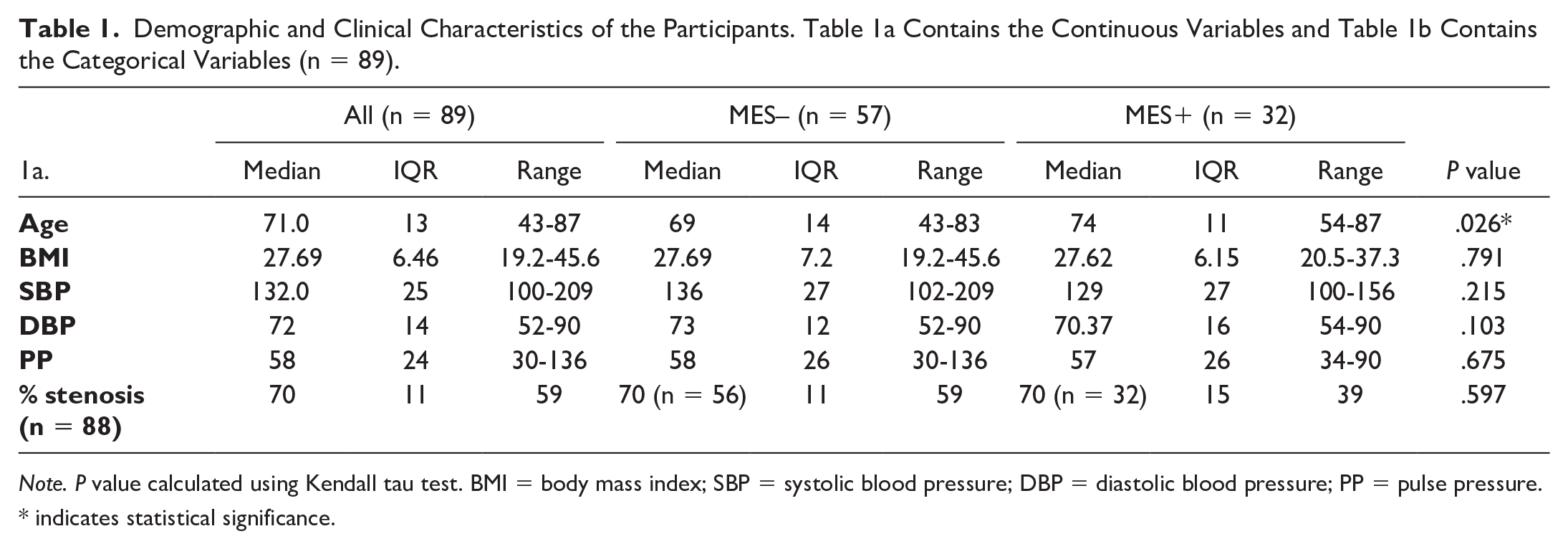
Note. P value calculated using Kendall tau test. BMI = body mass index; SBP = systolic blood pressure; DBP = diastolic blood pressure; PP = pulse pressure.
indicates statistical significance.
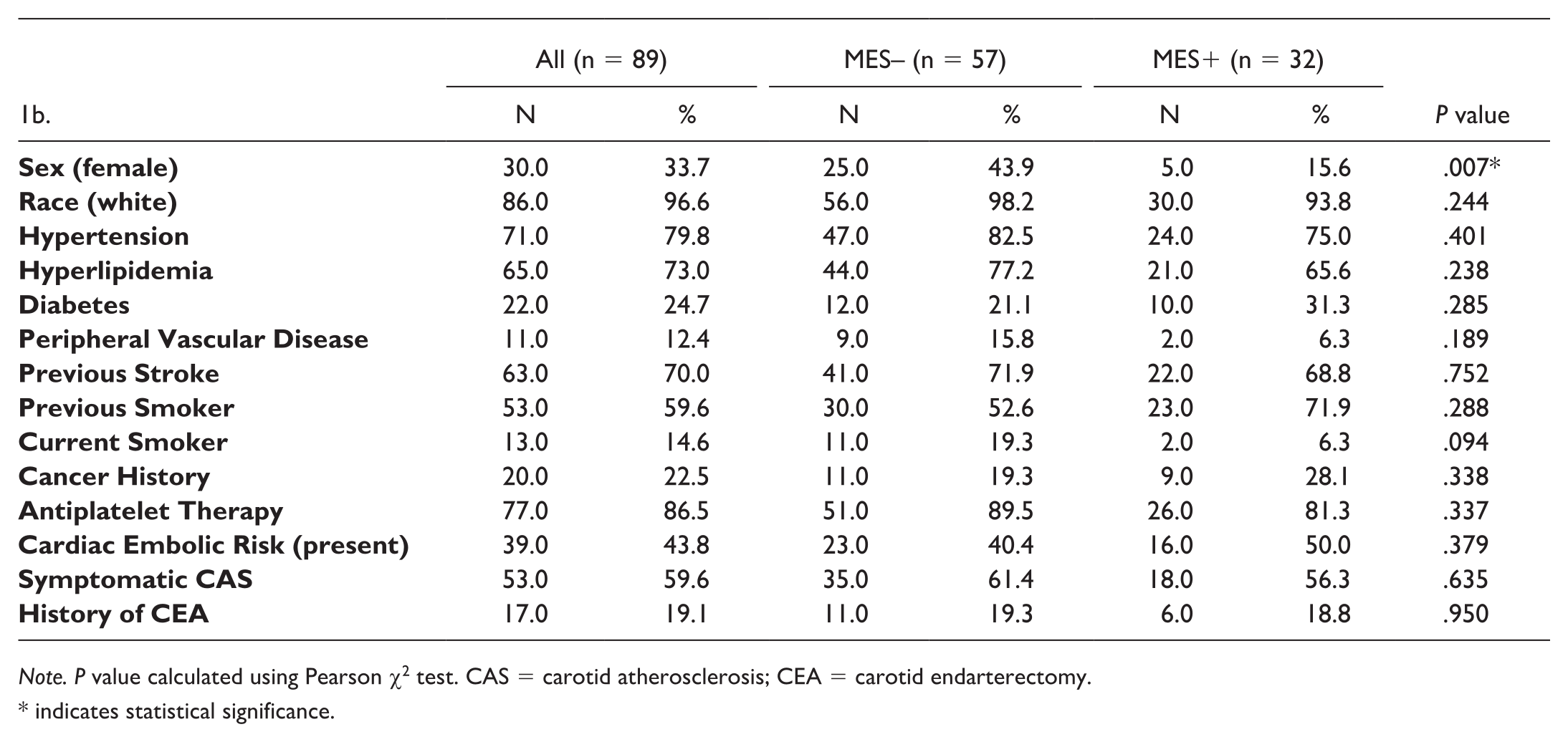
Note. P value calculated using Pearson χ2 test. CAS = carotid atherosclerosis; CEA = carotid endarterectomy.
indicates statistical significance.
MES and Clinical Characteristics
Eighty-nine participants underwent TCD monitoring for MES for 60 minutes (range 14-60 minutes, early termination of monitoring was mostly due to discomfort with the TCD helmet). Twelve patients had TCD on one side only due to no window on one side. The baseline clinical characteristics of patients who had MES (MES+) and those who did not (MES–) were compared. Significant evidence of association was noted between age (P = .026, Figure 1), sex (P = .007, Figure 2) and the presence of MES. No other clinical variables demonstrated an association with the presence of MES (P values > .05, Table 1). The carotid artery stenosis on the surgical side was available for 88 participants (median = 70%, IQR = 11, min = 40%, max = 99%). There was no statistically significant difference between the percent stenosis of participants with MES (median = 70%, IQR =15) and those without MES (median = 70%, IQR = 11) (P value = .597).

Average age of patients with and without MES. Significant difference is noted between the 2 groups (P = .028).
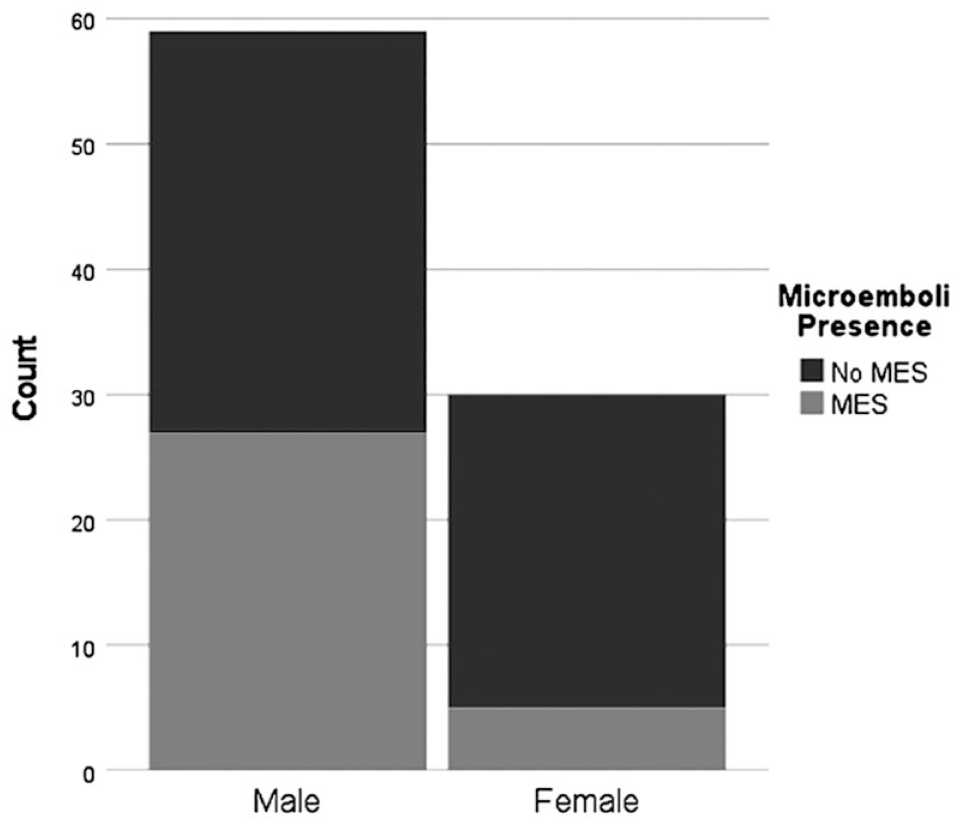
Presence of MES in male and female patients. Significant difference is noted between the 2 groups (P = .007).
MES in Relation to Treatment Groups
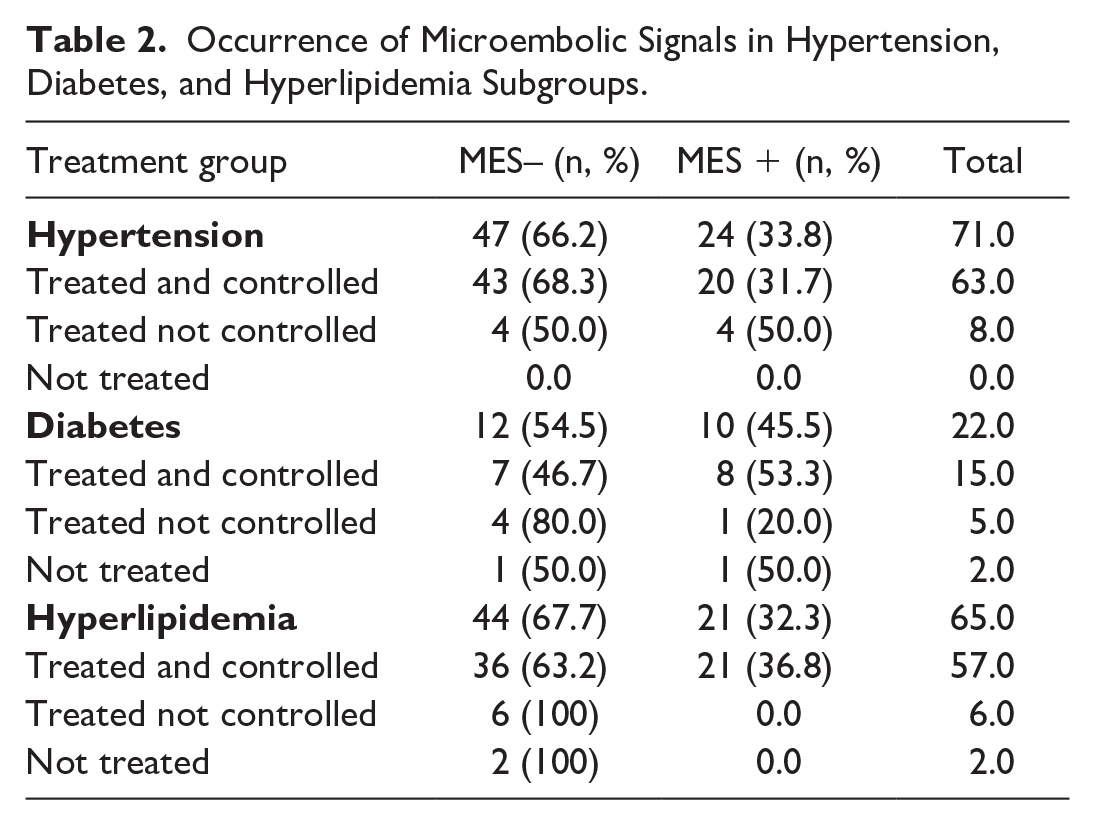
Participants with hypertension, diabetes, or hyperlipidemia were divided into 3 subgroups according to their treatments: treated and controlled (patients who are adherent to maximal medical therapy or values within normal limits; hypertension: SBP < 120 mmHg, DBP < 80 mmHg; diabetes: A1c <5.7%; hyperlipidemia: total cholesterol <200 mg/dL, low-density lipoprotein <100 mg/dL); treated not controlled, and not treated. None of the subgroups demonstrated significant association with the presence of MES (Table 2) (all P values > .05).
Occurrence of Microembolic Signals in Hypertension, Diabetes, and Hyperlipidemia Subgroups.
MES in Relation to Cardiac Embolic Risk Factors
The participants were stratified into no-risk, low-risk and high-risk for cardiac embolism according to the Guidelines for the Use of Echocardiography in the Evaluation of a Cardiac Source of Embolism. 15 The no-risk category is for patients without conditions that put them at a high or low risk for cardiac embolism according to Saric et al 15 risk stratification. Fifty participants had no cardiac source of embolism and of which 16 (32%) had MES recorded at least on one side (Table 3). The presence and side of MES in the no-risk group (n = 16) did not significantly correlate with the side of planned surgery (P = .078). Participants with a cardiac source of embolism (n = 39) had MES in 16 patients (41%); the difference between the 2 groups was not statistically significant (P = .379). No statistically significant correlation was discovered when examining the difference between the high-risk and low-risk categories (Table 3).
Occurrence of Microembolic Signals in the Embolic Risk Factors Subgroups.
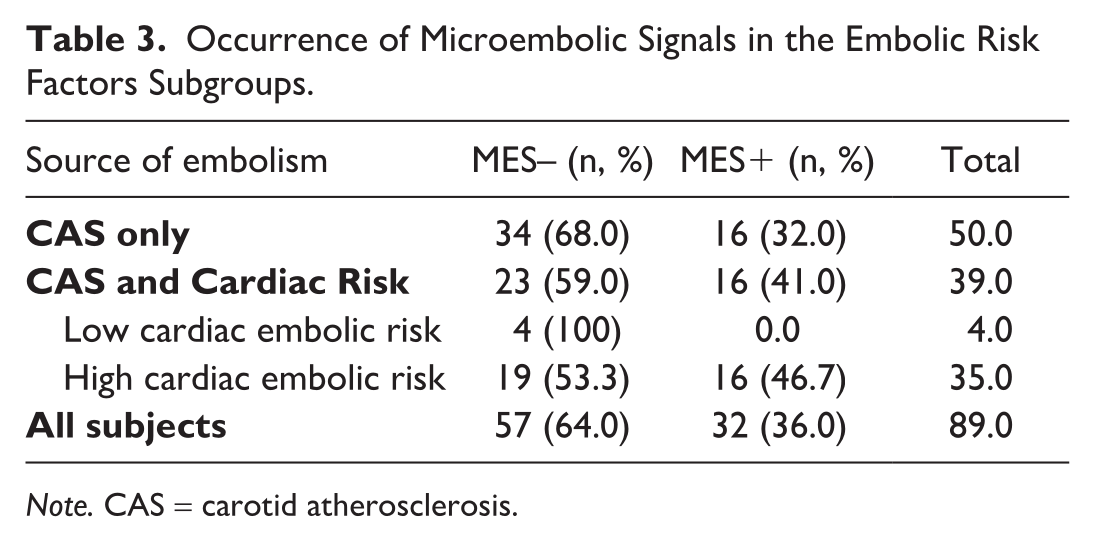
Note. CAS = carotid atherosclerosis.
Logistic Regression Model
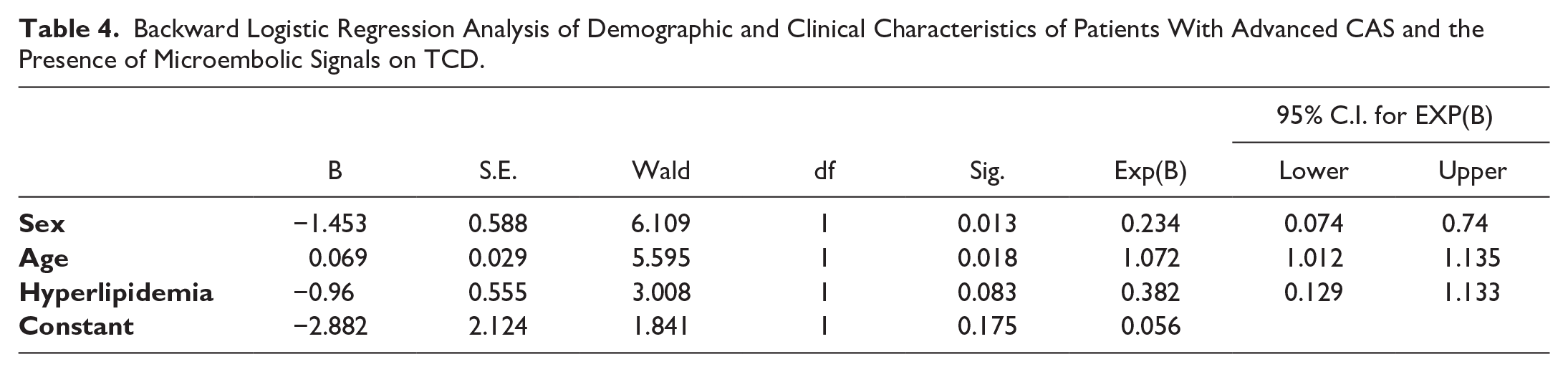
A backward logistic regression was performed to ascertain the effects of the clinical characteristics on the occurrence of MES as observed by TCD. The selected logistic regression model was statistically significant, χ2(3) = 15.611, P = .001. Of the clinical variables included in the model, age (P = .018) and sex (P = .013) were statistically significant (Table 4).
Backward Logistic Regression Analysis of Demographic and Clinical Characteristics of Patients With Advanced CAS and the Presence of Microembolic Signals on TCD.
Discussion and Conclusion
The detection of microemboli in the cerebral blood circulation in the form of MES has been made possible by the TCD embolus detection algorithm. These particles range between 20 and 100 µm and can be related to carotid plaque instability leading to silent or clinically overt embolic stroke. 6 The present study demonstrates a significant relationship between male sex and older age and the presence of MES on TCD in patients with advanced CAS.
Microembolic signals have been detected in patients with a variety of clinical risk factors, including CAS (both intracranial and extracranial) and cardiac sources of embolism such as atrial fibrillation and mechanical heart valves. 16 Despite the majority of our participants receiving antiplatelet therapy (86.5%), MES were present in 36% of them at least on one side. The presence of MES despite antiplatelet therapy is consistent with findings reported by others.17-20 Furthermore, previous work has demonstrated that the presence of MES is not affected by anticoagulation either, which highlights the nonthrombotic nature of these particles.17,19 We have also previously demonstrated a direct relationship between macroscopic plaque ulceration score and the frequency of MES. 12 Together, these findings support the hypothesis that MES could be caused by cholesterol crystals, platelet aggregates, or plaque debris released from unstable CAS. Previous studies have shown an increased frequency of MES in patients with CAS compared to control groups and demonstrated a significant relationship between these signals and cerebrovascular events.9,10,21-23 These findings highlight that large carotid artery plaques are major risk factors for MES.
Among the demographic and clinical characteristics examined in the present study, older age and male sex demonstrated strong evidence of association with the presence of MES (Table 1b). This suggests that males and older patients with advanced CAS are at an increased risk for the sequelae of chronic cerebral microembolism, including cognitive decline and risk for future stroke. To our knowledge, this is the first study to demonstrate this relationship. Several studies have previously examined the relationship between the demographic and clinical risk factors of patients with advanced CAS and the presence of MES and found no significant relationship between the 2 except for Spence et al 19 who observed significant correlation with smoking status, claudication, and homocysteine.10,20,24-27 These studies have mainly focused on the presence of MES on the ipsilateral side, while, in the present study, MES monitoring was performed bilaterally for the majority of patients. The reason for monitoring MES bilaterally is that atherosclerosis is a systemic disease, and its sequelae could be due to plaque instability at any location. Age and male sex are established risk factors for atherosclerotic plaque formation and instability, which could explain why these characteristics are significantly associated with MES.28-30
Interestingly, symptomatic status was not a predictor for the presence of MES in the present cohort. Therefore, both symptomatic and asymptomatic CAS appear to be susceptible to releasing microemboli. This finding may explain why both symptomatic and asymptomatic patients with CAS have an increased risk for cognitive decline.5,6,12
One of the questions examined in the present study was whether cardiac risk factors for emboli were associated with increased occurrence of MES in patients with advanced CAS. To answer this question, the participants were stratified into 3 groups based on their risk for cardiac embolism according to the Guidelines for the Use of Echocardiography in the Evaluation of a Cardiac Source of Embolism. 15 The 3 groups were no-risk, low-risk, and high-risk. Patients with high risk for cardiac embolism were more likely to have MES compared to patients with no cardiac risk factors (46.7% vs 32%, respectively), however, this relationship was not statistically significant (P > .05). Previous work by Sliwka et al 18 has shown no significant correlation between MES different cardiac conditions including atrial fibrillation, dilation cardiomyopathy, and aortic and mitral valve stenosis among others. Other studies, have shown a strong correlation between atrial fibrillation, artificial valves, and the presence of MES; however, unlike the present study, those studies included broader patient populations, while the current study specifically focused on patients with advanced CAS.31,32
In summary, MES were associated with age and sex in a cohort with advanced CAS. Symptomatic status was not a predictor for MES in this cohort, suggesting that plaques in both symptomatic and asymptomatic individuals have the ability to release microemboli. This work highlights the need for further investigation to better refine risk stratification for patients with advanced CAS by identifying specific characteristics of unstable plaques that contribute to MES and stroke risk.
Some of the limitations of the present study include the small sample size and the retrospective nature of the analysis. The absence of a statistically significant result in the present study does not prove that none exists due to the limited negative predictive power of the smaller sample size. In addition, we monitored the patients for up to 60 minutes on each side and recorded MES that were observed during that period. Any MES occurring outside of our timeframe were not accounted for in the present analysis. Finally, no adjustments have been made for multiple statistical comparisons made in this study.
Footnotes
We would like to thank all individuals who participated in this study.
Declaration of Conflicting Interests
Adil: None; Mitchell: Elsevier, author textbook chapters, and W. L. Gore & Associates contracted research grants to University of Wisconsin-Madison, consulting Acoustic Range Estimates.; Cook: Honaria from AbbVie Inc., Actelion Pharmaceuticals, Athira Pharma, Bayer HealthCare Pharmaceuticals Inc, Merck Research Laboratories, Sanifit Inc, KBP Biosciences USA Inc and salary support through contracts with BioCardia Inc., Pfizer, Alnylam Pharmaceuticals, Cytokenitics, Theravance Biopharma, GSK, Regeneron Pharmaceuticals, Novartis, Goldfinch Bio, Palladio Biosciences; Maybock: None; Meshram: None; Varghese: Drs. Varghese, Hermann and Dempsey have a patent (Varghese T, Dempsey RJ, Hermann BP. Characterization of vulnerable plaque using dynamic analysis. US2009/0198129 A1). We are grateful to Siemens Medical Solutions USA, Inc., for providing the S2000 Axius Direct Ultrasound Research Interface (URI) and software licenses; Wilbrand: None; Dempsey: None.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported NIH grants F31 HL 141008, R01HL147866, R01 NS064034 and 2R01CA112192. This work was also supported in part by the University of Wisconsin–Madison Office of the Vice Chancellor for Research and Graduate Education with funding from the Wisconsin Alumni Research Foundation.