
Abstract
Endofibrosis is a rare disorder affecting primarily young healthy athletes, often elite cyclists, or runners. In most published cases, the external iliac artery is affected but studies have shown that in some cases, other vessels may become affected as well. Diagnosing these patients often becomes a challenge since most patients are asymptomatic until being subjected to extreme conditions such as intense training or athletic competition. This is a case of a 41-year-old female elite cyclist and runner who presented with pain in her right thigh with heavy exercise. This case illustrates the need to include a full clinical assessment as well as additional testing immediately to avoid delaying care on patients who may get discharged due to their otherwise healthy presentation in normal conditions.
Keywords
Introduction
The exact pathophysiology of endofibrosis is not well known but is documented in numerous papers that it may lead to arterial stenosis, dissection and in rare cases adventitial cystic disease. It was first documented with cyclists in 1986 by Chevalier et al 1 and since then, multiple cases have been documented with a more extensive group of elite athletes including runners, rugby players and even cross-country skiers.2-4
Case Report
A 41-year-old woman presented with right thigh pain which progressively became worse over the past several years. The pain can be somewhat alleviated with slow walking; however, recently she reports the need to sit down to alleviate the pain. The patient has a history of hyperlipidemia and she previously smoked which she quit more than 10 years ago. She denies any prior cardiovascular surgeries.
Indirect arterial physiologic testing was performed using a Vasculab GSX with a 3-cuff method documenting pressures, pulse volume recordings (PVR), and Doppler waveforms at the ankle, metatarsal, and great toe level. Initial testing showed a resting ankle/brachial index (ABI) of 0.82 on the right and 1.29 on the left. PVR tracings at rest on the right showed an absence of dicrotic notch, a decrease in amplitude and delay in the upstroke of the tracing when compared to the left. Post exercise, the ABI showed a significant drop in ABI on the right to 0.28 (Figure 1).
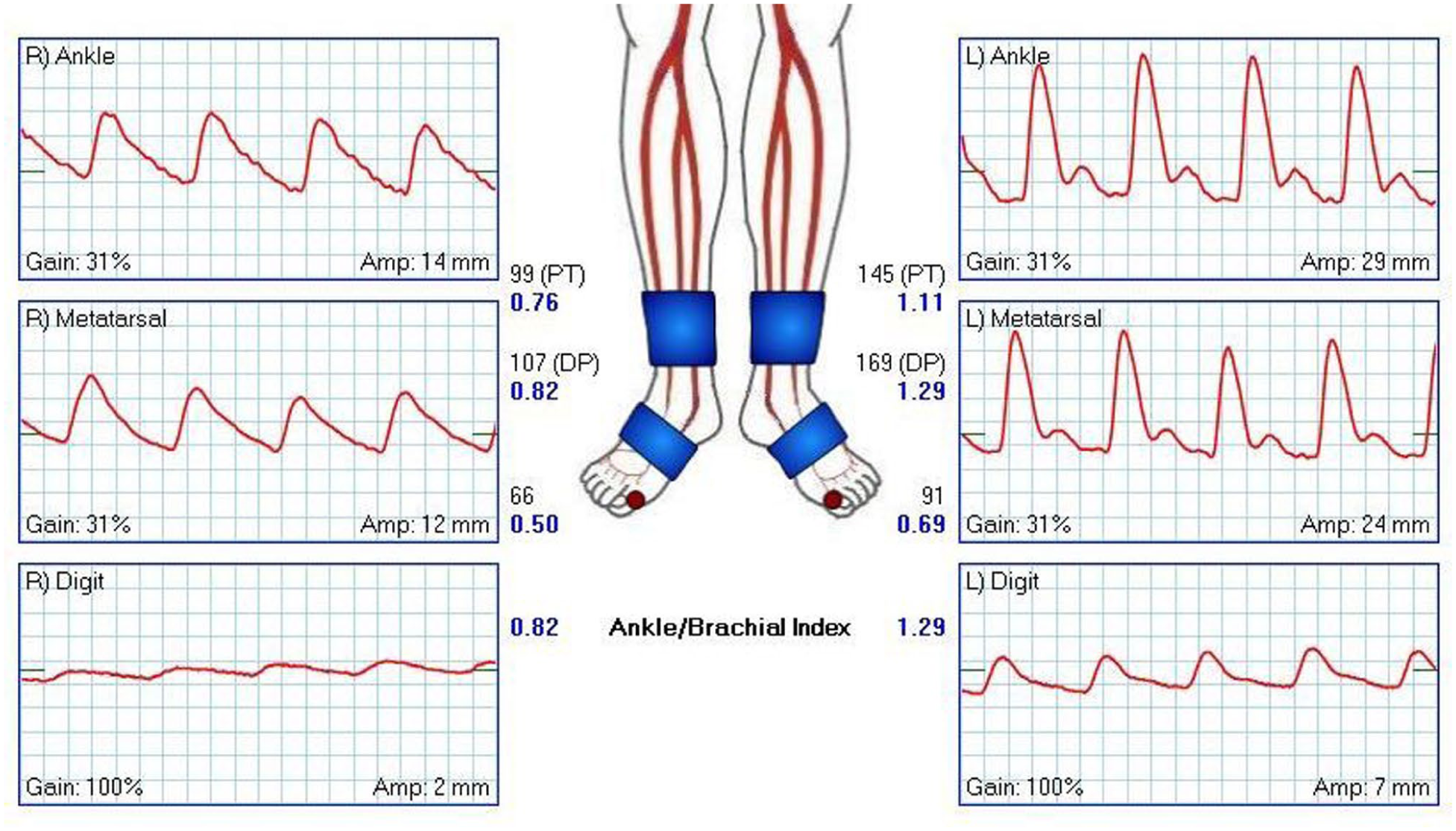
PVR tracings at the ankle, metatarsal, and great toe bilaterally.
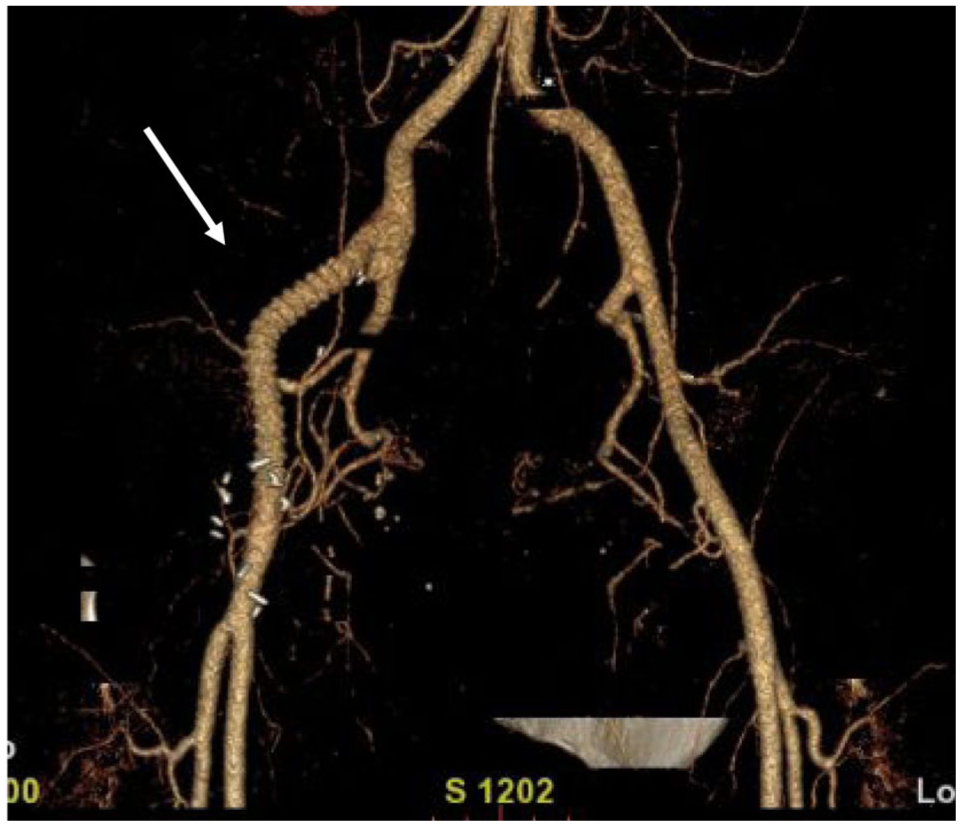
Duplex imaging was performed on a GE Logiq E9 and showed dampened and post stenotic waveforms in the common femoral artery on the right. Further investigation revealed an occlusion of the external iliac artery (EIA) which was confirmed with a computed tomography angiography (CTA) of the abdomen with contrast. No other initial abnormalities were documented at this time. The vascular team determined the best treatment would be to perform a thrombectomy and a bypass graft. The surgery was successful, the patient was discharged 3 days later and scheduled for her follow-up testing and office visits (Figure 2).

3D reconstruction using computed tomography angiography of the abdomen obtained following initial ultrasound testing showing occluded right external iliac artery and multiple collateral vessels.
When she returned for a follow-up 1 year later, indirect arterial testing was performed and showed a normal ABI of 1.12 at rest; however, when the patient was exercised, she had a drop in the ABI to 0.70. A CTA of the abdomen with contrast was again performed at this time and revealed an occluded ilio-femoral bypass graft. The patient was taken to the interventional radiology department and underwent an additional thrombectomy to reopen the bypass graft (Figure 3).
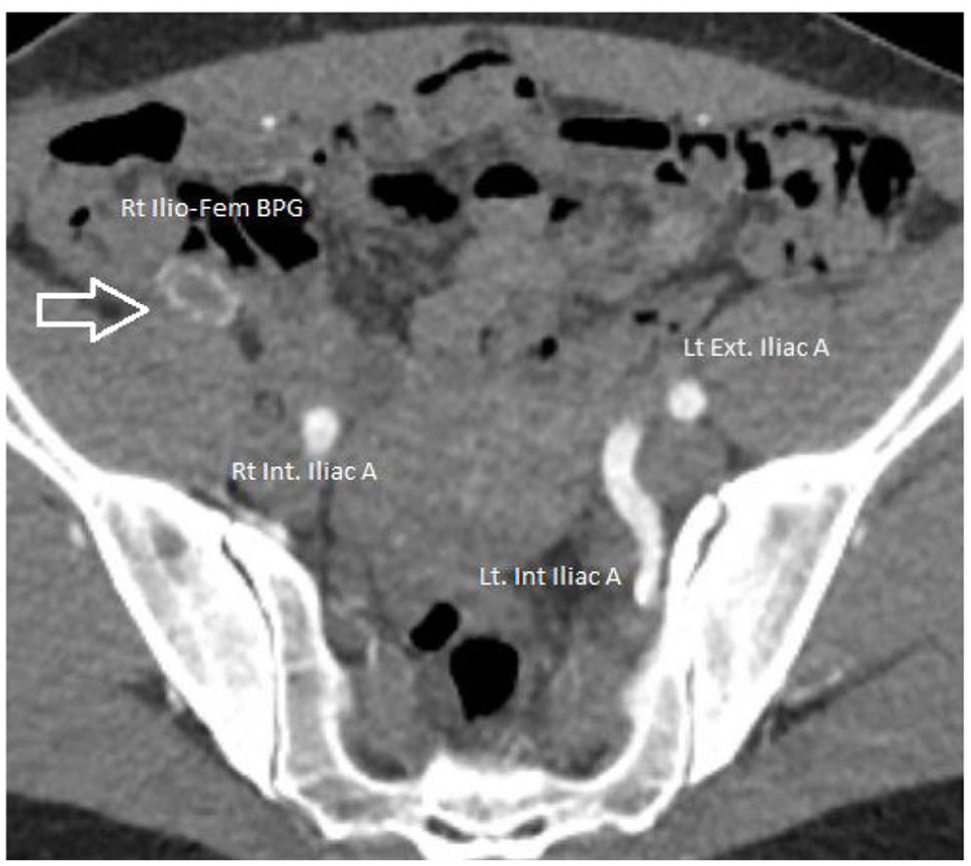
Postoperative computed tomography angiography of the abdomen showing occluded right ilio-femoral bypass graft.
The patient returned 2 years later for a CTA of the abdomen with contrast which showed continued patency of the bypass graft at that time; however, her symptoms were returning so an arterial duplex was performed. The ultrasound showed a patent ilio-femoral bypass graft with adequate flow throughout and multiphasic waveforms in the common femoral artery. The cause of her symptoms is unknown at the time of this paper (Figures 4 and 5).
3D reconstruction using computed tomography angiography of the abdomen obtained at the 2-year follow-up stage.
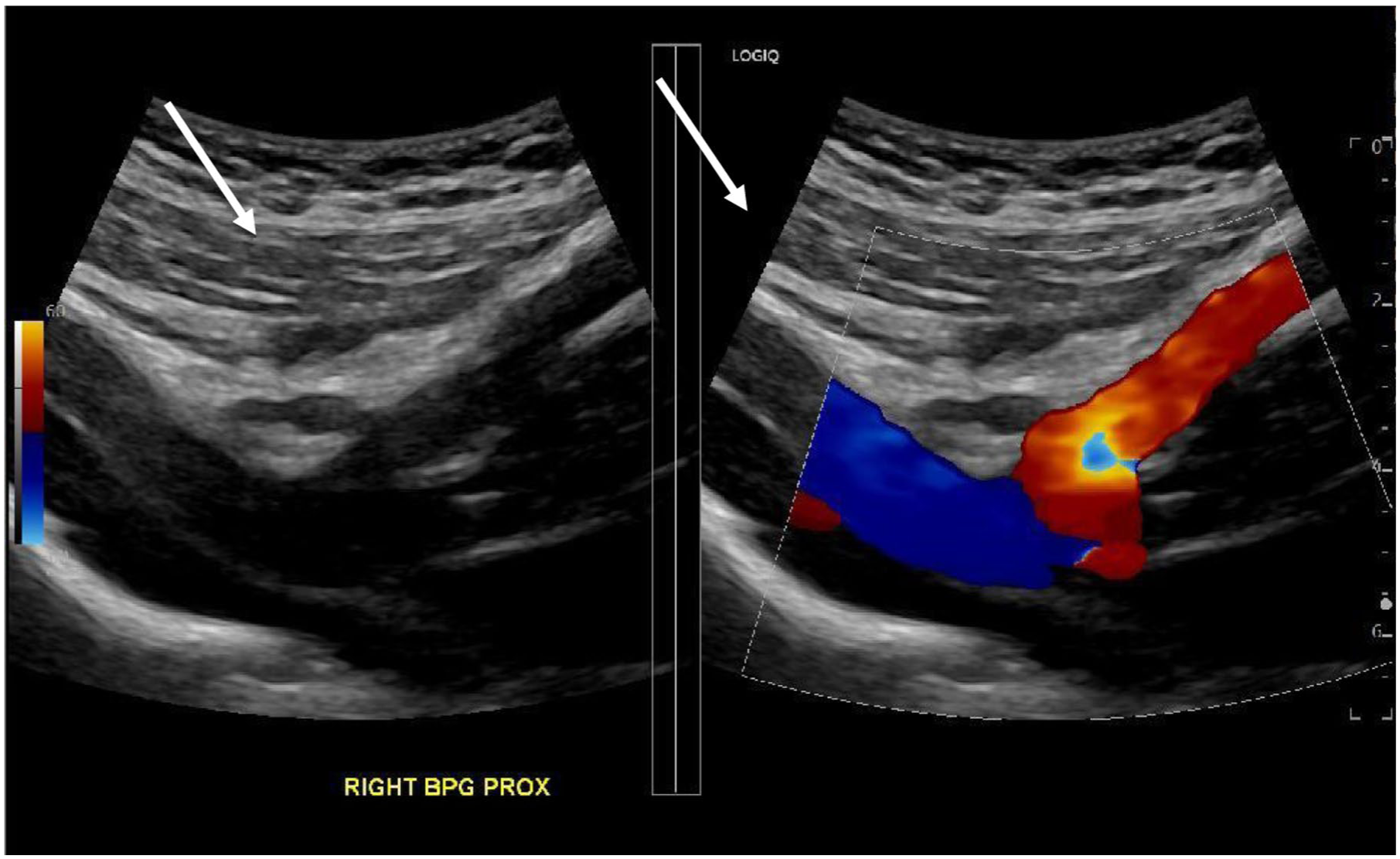
Ultrasound obtained at the 2-year follow-up stage showing patency of the ilio-femoral bypass graft.
Discussion
Endofibrosis primarily is thought to be caused by the repetitive stress and compression of the external iliac artery due to the increase in size in the muscles responsible for typical hip flexion. In some reported research, excessive vessel length and hip joint hyperflexion can increase the likelihood of endofibrosis causing the artery to thicken and narrow. This creates intimal thickening of the vessel walls leading to muscle cramping, weakness, and often significant pain during intense workouts. The unique presentation typically associated with patients with endofibrosis, the appropriate testing will prove to be an important tool in the initial diagnosing stage. With elite athletes, determining and isolating a problem is often the hardest part due to their extreme training requirements and otherwise above average physical fitness. This patient presented with pain that limited her bicycle training by several miles; however, her physical conditioning allowed her to recover quickly and continue to perform at a level higher than the average patient. Traditional protocols and methods of testing are focused on the typical patient population for structure and consistency and in cases such as this, established protocols do not provide sufficient information and must be adjusted appropriately.
Typical testing should include the assessment of blood vessels in the abdomen and groin including the common and external iliac arteries as well as the common femoral, profunda, and superficial femoral arteries. An ABI at rest and with exercise is the ideal first choice for testing. When done appropriately, this provides significant information regarding the perfusion, or lack of perfusion, of the blood during extreme workouts. Once determined there is a decrease in perfusion, duplex imaging of the external iliac and common femoral arteries will provide additional specific information as to the location and degree of the disease process. At this stage, any findings should be correlated with CTA/MRA or intravascular ultrasound (IVUS) which is also utilized for more specific diagnoses and in some cases treatment.
Treatment for endofibrosis can be complicated and requires significant planning and thought. Often an embolectomy/thrombectomy can be utilized if detected early or ilio-femoral endarterectomy and bypass if discovered in a chronic state. Minimally invasive percutaneous thrombectomy is usually the first option due to its minimally invasive approach which only requires a small incision in the groin and a sheath to be placed within the external iliac artery. A wire can be inserted and advanced into the contralateral artery and through the diseased segment. A balloon is then inflated within the segment, opening the artery and restoring blood flow to the area. In the case of a more chronic or complete occlusion, a more aggressive approach with bypass of the affected area may the appropriate treatment.
Conclusions
Endofibrosis is one of the more challenging disease processes to evaluate and treat. This case is a reminder to have the proper testing protocols in place and make all efforts to perform a thorough clinical history and physical examination. Without the knowledge of the patient’s exercise routine throughout all stages of testing and a structured follow-up protocol, this patient may have gone undiagnosed and possibly never treated. At times, vascular medicine will focus on the palliative care aspect and will approach cases like this with a way to improve the patient’s quality of life first, then only investigate it further if needed. Often, cases like this are treated incorrectly and the true causes go unnoticed and undiagnosed unless they return with specific symptoms.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.