
Abstract
Deep vein thrombosis (DVT) is a serious condition, and if left untreated, it can lead to a pulmonary embolism. In patients with chronically occluded veins, other symptoms can develop, often grouped under the diagnosis of post-thrombotic syndrome (PTS). This case study describes the unusual finding of an acquired arterio-venous fistula (AVF) following a left leg DVT in a 78-year-old male patient. The patient had a history of previous DVT and multiple comorbidities, which may have contributed to his presenting symptoms of left leg swelling and pain. However, an unexpected connection between the sapheno-femoral junction and common femoral artery was identified with ultrasound, consistent in appearance with an AVF. The patient had no history of vascular injury or access in the groin. A literature review identified a retrospective study and 4 case reports describing similar clinical presentations, and further analysis highlighted the potential benefits of venous stenting in symptomatic patients. However, the mechanism of action for the formation of an AVF following DVT is unclear. One such factor that could explain this phenomenon is vascular endothelial growth factor (VEGF), which upregulates angiogenesis. In an occluded vessel, VEGF is dysregulated and may provide an explanation for the development of an AVF following DVT. This case study aims to raise awareness of the development of AVF in patients with a history of DVT. Our case shows that an acquired AVF can arise in patients without a history of vascular access or iatrogenic injury and may be potentially missed in patients diagnosed with PTS. The use of pulse wave Doppler in addition to compression and colour Doppler was key to identifying the AVF and providing important haemodynamic information.
Keywords
Introduction
Deep vein thrombosis (DVT) is a serious condition in which the development of a thrombus through the coagulation cascade arises within the deep venous system. Virchow’s triad encompasses the 3 main risk factors that can lead to the formation of DVT. These risk factors include venous stasis, endothelial injury, and hypercoagulability. 1 If left untreated, DVT can potentially lead to a pulmonary embolism and could result in serious complications or death.
Ultrasound is considered the most accurate non-invasive method for assessing DVT, using a combination of B-mode compressions and colour and spectral imaging to diagnose DVT. 2 The Wells score assesses the clinical probability of DVT, applying clinical criteria to determine whether an ultrasound scan is indicated. If the Wells score is negative, with a score of less than 2, a D-dimer assay is performed, which detects fibrin degradation products. 3 A positive D-dimer result indicates the need for ultrasound imaging to confirm or exclude DVT.
In cases of a previously diagnosed DVT, it can be challenging to assess whether the thrombus is acute or chronic in nature. Certain factors when performing an ultrasound assessment for DVT can help the user distinguish between acute and chronic thrombus. 4 The appearance of the thrombus in patients with an acute DVT includes echolucent thrombus and distended walls that are non-compressible using B-mode imaging. In patients with chronic thrombus, the vein may appear narrowed, with an echogenic lumen and potentially collateralised flow.
It is not uncommon for patients to have post-thrombotic syndrome (PTS) after a diagnosis of DVT, with 20% to 50% of symptomatic patients developing PTS within 2 years. 5 It is believed that PTS develops due to venous hypertension leading to a clinical presentation of edema, pain, and hyperpigmentation. 6 In more severe cases, 5% to 10% of patients will develop venous ulcers. 5 However, symptoms of PTS often overlap with those of chronic venous insufficiency and recurrent DVTs, 7 complicating the diagnosis in the absence of prior imaging.
Arterio-venous fistulas (AVFs) are an abnormal connection between an artery and a vein and are most commonly acquired through surgical intervention or trauma. 8 Congenital AVFs are less common and can occur anywhere in the body. On ultrasound, an AVF can alter the standard haemodynamics seen, with venous flow demonstrating pulsatility and increased diastolic flow in the arterial system. 9
This case study reviews the presentation of an AVF following a left leg DVT in a 78-year-old male patient and explores the potential mechanisms that could have led to this unusual finding. What makes this case interesting is the lack of evidence to suggest the AVF was congenital or acquired through surgical intervention or trauma, and the AVF visualised may have developed due to the DVT.
Case Report
In June 2023, a 78-year-old male patient presented with a swollen left leg and pitting edema, with a Wells score of 3 and a raised D-dimer of 8.28 μg/mL. The patient had previously presented in June 2022, when ultrasound had identified an occlusive proximal DVT extending from the left popliteal vein to the external iliac vein (EIV) consistent with an acute DVT (Figure 1A and B).
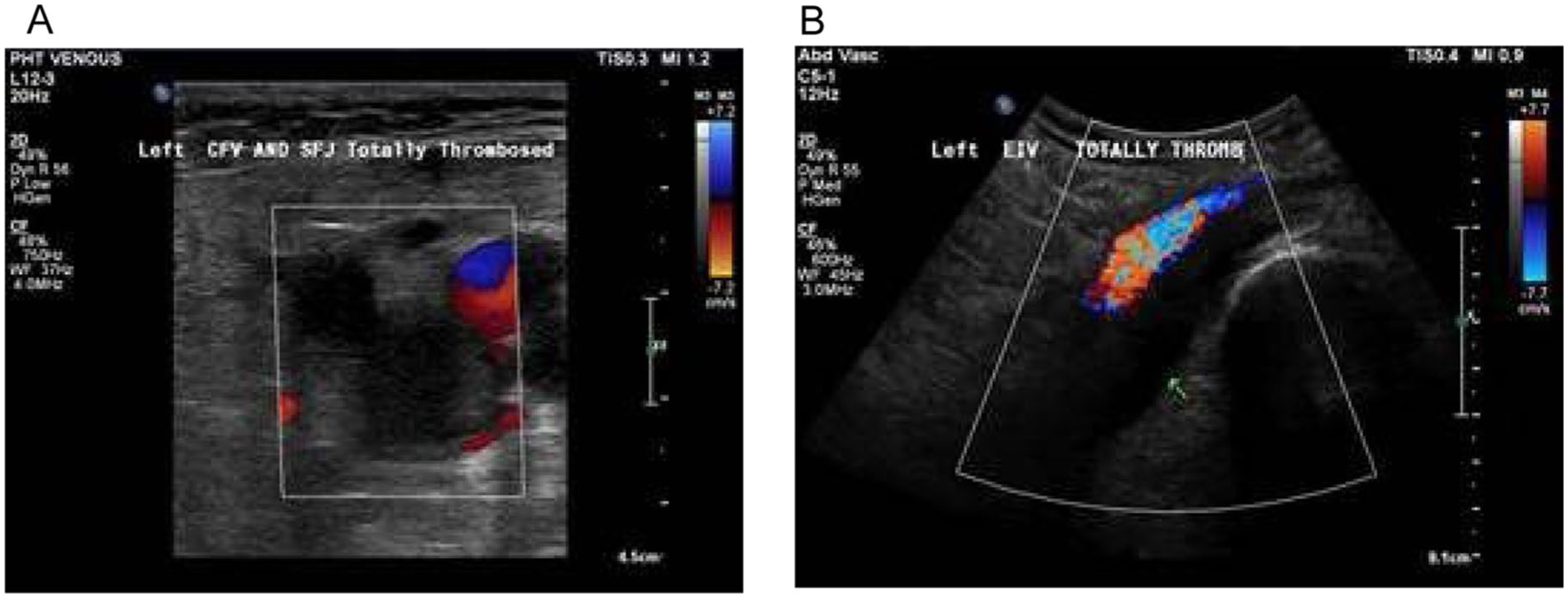
Colour ultrasound images from June 2022 demonstrating a totally thrombosed left common femoral vein (CFV) and sapheno-femoral junction (SFJ) (A) and external iliac vein (EIV) (B).
The patient had no family history of venous thromboembolism but did have several comorbidities, including hypertension, angina, and arthritis, which may have contributed to the symptoms of chronic pain and left leg swelling when the patient presented for ultrasound assessment a year later in June 2023.
The scan completed in June 2023 identified an occlusive thrombus extending from the popliteal vein to the mid-femoral vein (FV) with partial flow in the proximal FV and common femoral vein (CFV). The FV was small calibre, and the presence of patent channels of flow proximally demonstrated recanalisation through chronic post-thrombotic changes (Figure 2A and B). The location of the thrombus was also consistent with the previously diagnosed DVT and suggested that the presenting chronic symptoms were more consistent with the presence of PTS.
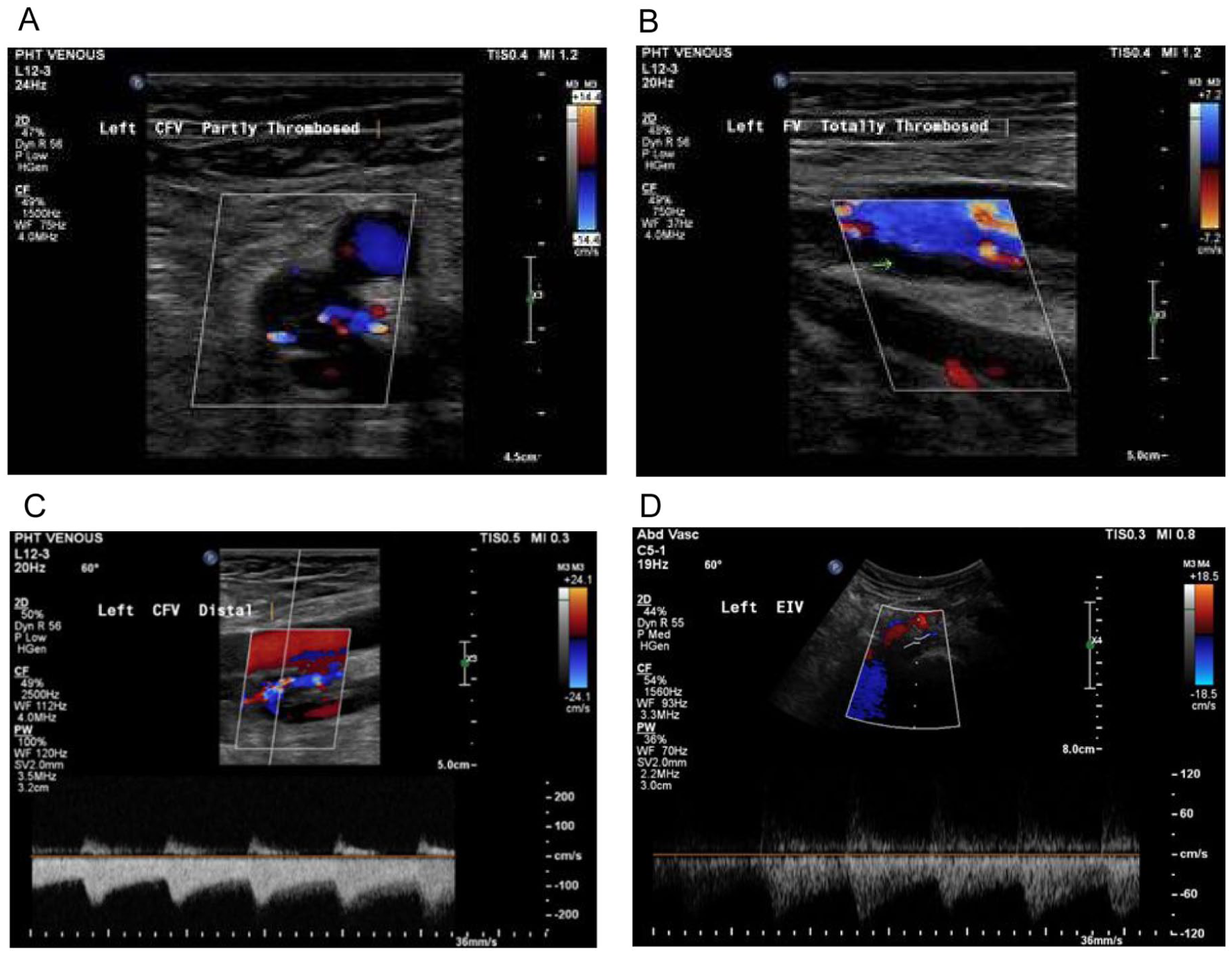
Colour ultrasound images from June 2023 demonstrating the small calibre totally thrombosed mid-femoral vein (FV) (A) and partial flow in the common femoral vein (CFV) with the appearance of recanalisation (B). Pulsatile arterialised flow can be visualised in the recanalised flow in the distal CFV (C) and the widely patent external iliac vein (EIV) (D).
However, upon further examination with Doppler ultrasound, the flow in the small channels of what was considered recanalised flow in the proximal FV and CFV, as well as the flow in the patent vessels more proximally, revealed pulsatile arterialised waveforms consistent with those seen in the presence of an AVF (Figure 2C and D).
This was not present on the previous scan in June 2022, and further examination revealed an unusual connection between the sapheno-femoral junction (SFJ) and the left common femoral artery (CFA) with an arterialised waveform, with high velocities seen at the SFJ (Figure 3A and B).
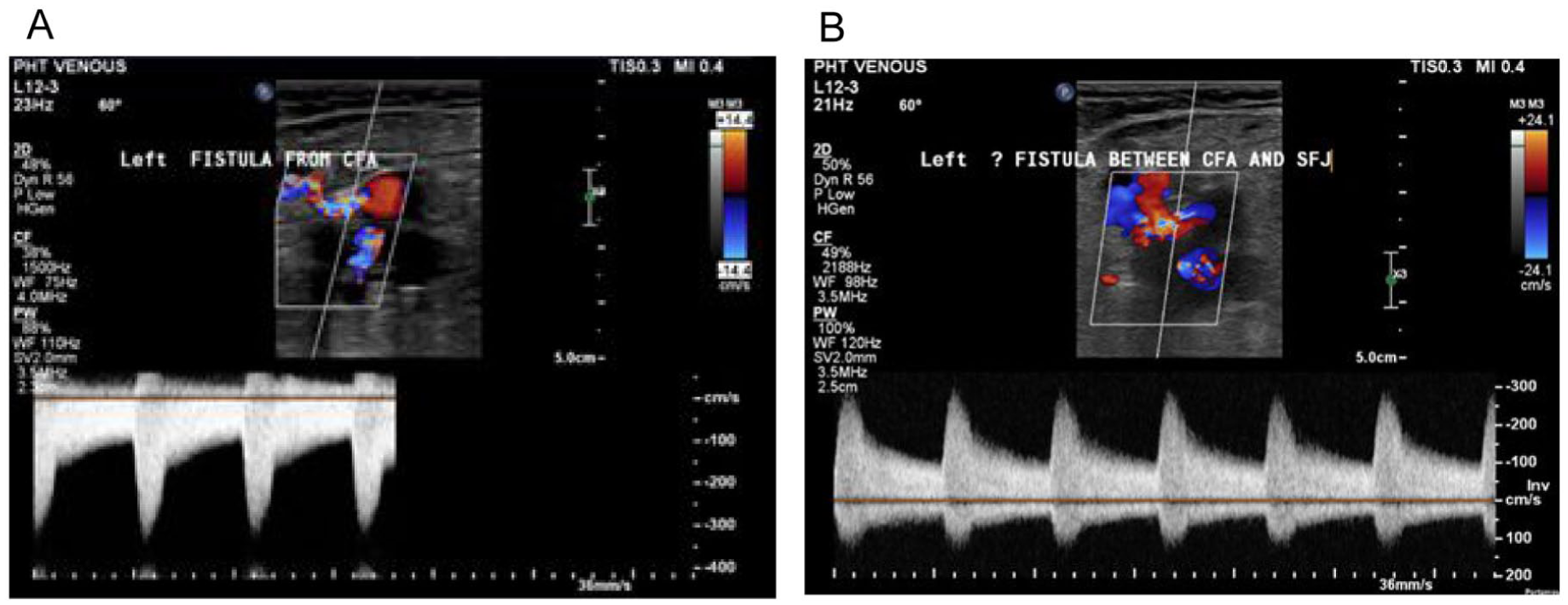
Doppler ultrasound images from June 2023 demonstrating a connection between the common femoral artery (CFA) and the sapheno-femoral junction (SFJ) (A and B) with an arterialised waveform and high velocities at the SFJ.
This raised suspicion of an iatrogenic injury; however, the patient reported no history of vascular access through the groin, and this was confirmed from the patient’s medical notes. The patient was indefinitely treated with apixaban. At a subsequent follow-up with the vascular consultant, the patient reported a reduction in swelling and was discharged, with ongoing management limited to treatment of the DVT with anticoagulation. The patient has not undergone further vascular imaging since 2023 and has remained asymptomatic with respect to both the DVT and the AVF.
Both duplex ultrasound assessments completed in June 2022 and June 2023 were performed using a Philips EPIQ 7 ultrasound system. Two broadband transducers were utilised according to vessel depth and anatomical location: a linear array transducer (12-3 MHz) and a curvilinear array transducer (5-1 MHz). To ensure diagnostic accuracy, image optimisation was achieved through adjustment of imaging depth, focal zones, and time gain compensation to maximise spatial resolution. Colour Doppler pulse repetition frequency and gain were optimised to demonstrate the direction of flow and turbulence within the AVF. Spectral Doppler was used for haemodynamic assessment, which enabled the assessment of flow characteristics, with angle correction maintained at ≤60° to minimise velocity measurement error.
Discussion: Comparative Analysis of Arterio-Venous Fistula Development Post-Deep Vein Thrombosis
Previous case studies and reports have described similar presentations. These are summarised in Table 1. A study conducted by Labropoulos et al 10 aimed to investigate the development of AVF in patients following DVT. Their findings identified 25 incidences of AVF formation in 22 patients with either acute or acute-on-chronic thrombus. The majority of AVFs were identified within the deep venous system, with 32% involving the CFV. While uncommon, these findings highlight that AVF formation can occur following DVT, reinforce the relevance of our patient’s presentation, and suggest that AVF may be under-recognised when evaluating patients following DVT.
Literature Analysis of Acquired Arterio-Venous Fistulas Following DVT.
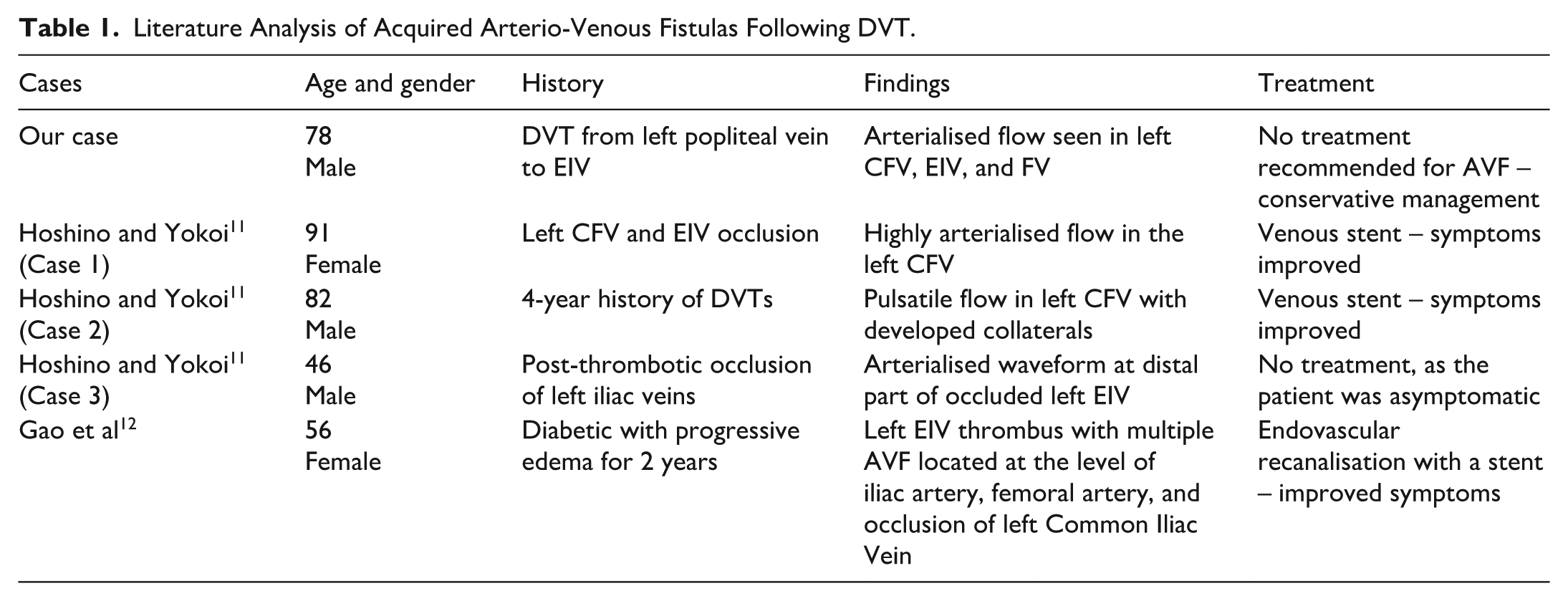
Further case studies have shown similar findings, emphasising the rarity and probable oversight of acquired AVF in patients with PTS. The first case study reported by Hoshino and Yokoi in their 2022 paper11 demonstrated similar findings to our patient. A 91-year-old female had a previous history of DVT in her left leg and presented with left leg swelling and pain 6 months after the original DVT diagnosis. An ultrasound scan identified a high-velocity arterialised waveform in the left CFV consistent with the presence of an AVF. Further analysis with contrast-enhanced computed tomography showed extensive collateral vessels within the left groyne. The case described that, as the patient continued to have worsening symptoms, a venous stent was inserted to cover the section with the fistula. This led to a significant improvement in the patient’s symptoms, and a subsequent ultrasound post-procedure demonstrated a return to a normal phasic, venous waveform in the CFV.
The second case reported by Hoshino and Yokoi11 also reported similar findings in an 82-year-old male patient with a 4-year history of DVT. Venous stenting again resulted in significantly improved symptoms after 52 months of follow-up. A further case study by Gao et al12 reported treatment for a patient suffering from an acquired AVF following DVT of the left CFV.12 This patient was also treated with a venous stent and endovascular recanalisation, which led to significant improvements in her symptoms at 4 years post-procedure, with subsequent ultrasound confirming the restoration of normal venous waveforms following stenting.
These cases suggest that venous stenting may be a viable treatment option for symptomatic patients with an acquired AVF post-DVT; however, a third case reported by Hoshino and Yokoi11 describes an incidental finding of an AVF in a 46-year-old male patient who remained asymptomatic after 18 months of surveillance. This case required no intervention, suggesting that not all cases are symptomatic and warrant intervention.
Venous Stenting – A Viable Option for Symptomatic Patients?
A retrospective study conducted by Yuan and colleagues analysed the potential benefits of different interventions in patients with an acquired AVF with PTS. 13 The study compared standard compression therapy with venous hypertension-relieving therapy (VHRT), which included venous stenting, femoral-to-femoral bypass, and arterial embolisation. Although outcomes for the individual intervention types were not described, this study clearly demonstrates a significant improvement in symptoms for patients who were treated with VHRT, compared to standard compression therapy, which showed no significant change in symptom burden at 12 months. Of the 17 patients in the study who underwent VHRT, 4 were treated with a femoral-femoral bypass, 7 were treated with venous stenting, and the remaining 6 patients were treated with arterial embolisation. Arterial embolisation led to a high recurrence rate of AVF (66.7%), with 2 of these patients subsequently treated with venous stent insertion, supporting the potential benefit of venous stenting over other clinical interventions.
Although our patient was conservatively managed with improvement to his symptoms, this study highlights an alternative approach to the management of symptomatic PTS patients with an acquired AVF. In comparison to standard compression therapy, venous stenting led to improvement in symptoms demonstrated 1 month post-procedure, highlighting the potential benefits of venous stenting in symptomatic patients.
Vascular Endothelial Growth Factor – A Potential Mechanism for the Development of Arterio-Venous Fistula Without Iatrogenic Injury?
There is evidence to suggest potential mechanisms that may contribute to the development of an AVF following DVT. The formation of an acquired AVF is thought to occur through the process of angiogenesis, where the formation of new blood vessels, resulting from the activation of multiple pathways, drives vascular growth.
One important regulator of angiogenesis is vascular endothelial growth factor (VEGF), a key signalling protein involved in several physiological processes, including angiogenesis and regulation of the coagulation cascade. 14 Within the VEGF family, VEGF-A is a key mediator of angiogenesis, promoting the formation of new blood vessels. Vascular endothelial growth factor signalling activates multiple pathways that enhance endothelial cell proliferation, migration, and vascular permeability, processes that influence endothelial function and angiogenesis. 15
Hypoxia is a key stimulus for VEGF-mediated vascular remodelling and new blood vessel formation, and this association is well established. Forsythe et al 16 demonstrated that over-expression of hypoxia-inducible factor-1 (HIF-1), a transcription factor stabilised under hypoxic conditions, results in increased VEGF-A expression, supporting the role of hypoxia-driven VEGF signalling in vascular adaptation.
In this case, the patient’s chronically occluded FV is likely to have generated a hypoxic environment. Under hypoxic conditions, HIF-1 and VEGF-A are upregulated, leading to enhanced activation of downstream signalling pathways that promote endothelial activation and angiogenesis. The increased expression of VEGF in patients with DVT, and its role in promoting new blood vessel formation, align with anecdotal observations in DVT patients who often present with patent collateral vessels or bifid systems that were not reported on the original diagnostic scan. It is therefore plausible that the upregulation of VEGF may have contributed to the development of acquired AVF in our patient.
Conclusion
This case study highlights the interesting finding of an AVF in a patient with a previous history of DVT, with no iatrogenic injury or congenital disease. Ultrasound assessment of venous flow characteristics using spectral Doppler, in addition to compression ultrasound and colour Doppler, particularly in the groin, is key to identifying the presence of an AVF as well as providing important haemodynamic information regarding the venous flow both proximally and distally.
Previous case studies have demonstrated similar presentations to our case and have reported the clinical effectiveness of venous stenting in symptomatic patients. However, in patients who are asymptomatic or with improving symptoms, intervention may not be necessary, as it may lead to further risks for the patient, and conservative management may only be required.
While the mechanism for AVF formation following DVT is unclear, the evidence gathered suggests that VEGF, specifically VEGF-A, may have a significant role in the development of new blood vessels in a hypoxic environment. Given the favourable conditions formed in our patient from the DVT, this may potentially explain why the AVF developed.
This case study aims to raise awareness that acquired AVF could potentially arise in patients without a history of vascular access and iatrogenic injury, especially those with a history of DVT, and is something to consider alongside the diagnosis of PTS.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.