
Abstract
Takayasu arteritis (TA) is a rare granulomatous vasculitis affecting large arteries, predominantly in young women. Vascular ultrasound is of immense value in disease assessment and longitudinal monitoring. We present a 2-time-point duplex ultrasound (DUS) comparison in a 39-year-old woman with TA, evaluated at diagnosis and after 8 years of medical immunosuppressive therapy without the need for surgical or endovascular revascularization. At baseline, carotid ultrasound demonstrated complete occlusion of the right common carotid artery (CCA), retrograde flow in the external carotid artery (ECA) supplying the internal carotid artery (ICA), and diffuse arterial wall thickening. At the 8-year follow-up, DUS revealed central color flow within the right CCA consistent with recanalization, persistent retrograde flow in the ECA, heterogeneous plaque formation within the ICA, progressive stenosis of the left common and external carotid arteries, restenosis of the proximal subclavian artery, and predominantly antegrade vertebral artery flow with early subclavian steal physiology. Tomographic imaging correlated well with the DUS findings. This case highlights the value of DUS in characterizing chronic vascular remodeling and hemodynamic adaptation in TA over time. Follow-up with DUS demonstrates both progression and partial improvement of arterial lesions under medical therapy, underscoring the importance of ongoing ultrasound surveillance in long-term disease management.
Keywords
Introduction
Takayasu arteritis (TA) is a chronic granulomatous vasculitis affecting large arteries, most commonly the aorta and its major branches. 1 The disease predominantly affects young women in the second and third decades of life, with preferential involvement of the common carotid, subclavian, renal, and vertebral arteries. 2
Due to the absence of disease-specific biomarkers, imaging plays a central role in the diagnosis and longitudinal assessment of TA. Duplex ultrasound (DUS) offers a non-invasive, radiation-free method for evaluating arterial wall morphology and hemodynamics, allowing differentiation between inflammatory, fibrotic, and chronic occlusive changes while supporting clinical decision-making.3,4
Duplex Ultrasound Technique
Duplex ultrasound examinations at both time points were performed using high-resolution linear-array transducers. For the 2016 scan, a Philips scanner was used while the 2024 exam was performed with a Siemens Acuson Sequoia machine. Standard grayscale (B-mode), color Doppler, and spectral Doppler images were obtained according to established vascular ultrasound protocols. Arterial segments were interrogated in longitudinal and transverse planes with careful optimization of gain, pulse repetition frequency, and wall filter settings. Doppler angle correction was maintained at ≤60 ° for accurate velocity measurements. Stenosis severity was assessed using peak systolic velocity criteria summarized in Table 1. and waveform morphology.
Carotid Doppler Stenosis Criteria.
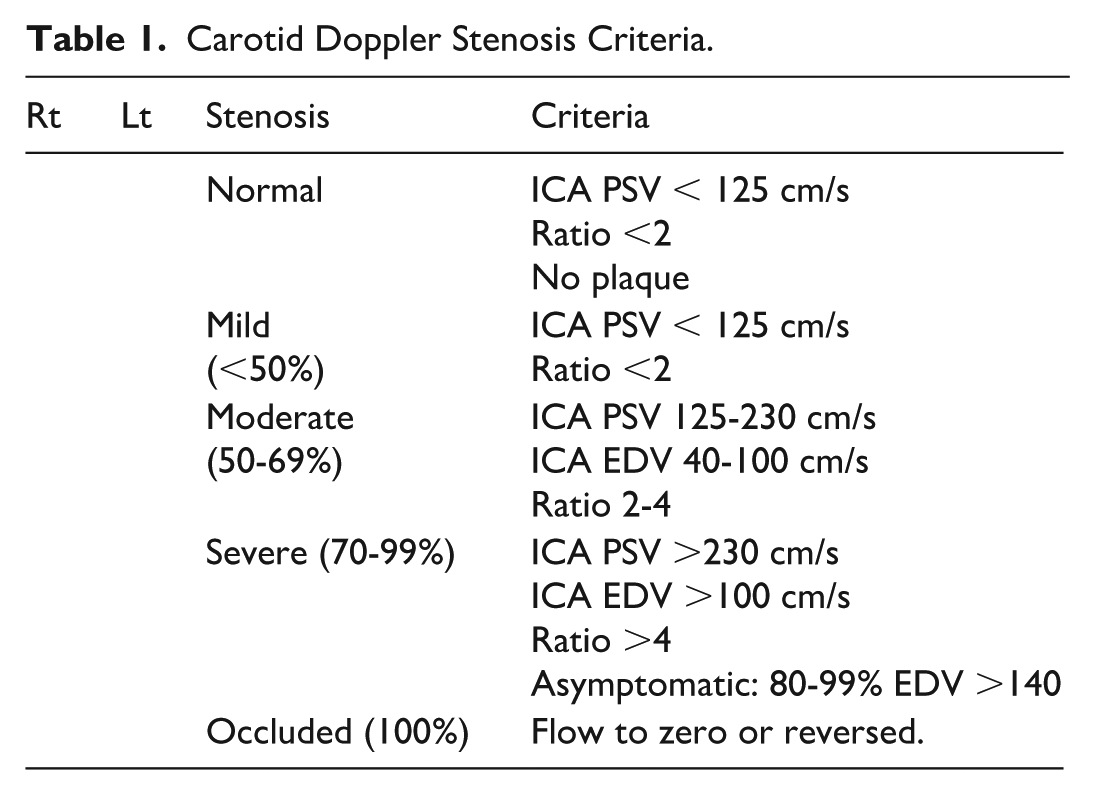
Occlusion was defined as the absence of detectable color and spectral Doppler flow, while patency was defined by the presence of intraluminal flow. All studies were performed by experienced vascular sonographers and interpreted by a registered physician in vascular interpretation (RPVI).
Ultrasound Features Characteristic of Takayasu Arteritis
In early TA, ultrasound typically shows intima-media thickening (IMT) of over 1 mm, with increased blood flow velocities beyond stenotic areas.3,4 A key sonographic feature is the “macaroni sign,” characterized by homogeneous, circumferential thickening of affected vessels, indicating edema or increased vascularity.5,6 Occlusions occur in later stages of the disease, marked by absent color Doppler flow in arteries filled with hypoechoic material, often with identifiable collateral flow due to the chronic nature of the condition.6,7
This case report compares recent DUS findings with those from the initial diagnosis in a 39-year-old American woman of Mexican descent with TA after 8 years of conservative therapy. It provides technical commentary on these findings, emphasizing the need for ongoing imaging and symptom monitoring.
Case Presentation
A 30-year-old American woman of Mexican descent initially presented in 2015 with progressive tachycardic episodes and recurrent headaches. Her past medical history was notable for a repaired ventricular septal defect in adolescence, recurrent ovarian cysts (one requiring surgical intervention) and anxiety attacks.
On physical examination at presentation, peripheral pulses were symmetric but globally diminished in all extremities, with similar blood pressure measurements in both upper extremities. A high-pitched systolic murmur was auscultated along the left sternal border with radiation to the neck, accompanied by prominent cervical bruits (left greater than right) and a left subclavian bruit. The patient reported intermittent tingling and numbness of the left arm and hand.
Initial vascular imaging in December 2015 demonstrated diffuse circumferential arterial wall thickening and luminal narrowing involving multiple large arteries. Carotid DUS revealed greater than 70% stenosis of the left internal carotid artery (ICA) based on elevated peak systolic velocities and 50% to 69% stenosis of the right ICA based on ICA-to-common carotid artery (CCA) velocity ratios, measured according to the North American Symptomatic Carotid Endarterectomy Trial (NASCET) criteria. Computed tomography angiography (CTA) of the neck showed diffuse wall thickening and high-grade luminal narrowing of the bilateral common and internal carotid arteries, brachiocephalic artery, and subclavian arteries. Additional imaging demonstrated circumferential wall thickening of the abdominal aorta and superior mesenteric artery. Based on characteristic clinical features and imaging findings, the diagnosis of TA was established using the American College of Rheumatology/European Alliance of Associations for Rheumatology (ACR/EULAR) classification criteria (Table 2.), with a total score ≥5.
2022 American College of Rheumatology/European Alliance of Associations for Rheumatology (ACR/ EULAR) Classification Criteria for Takayasu Arteritis.
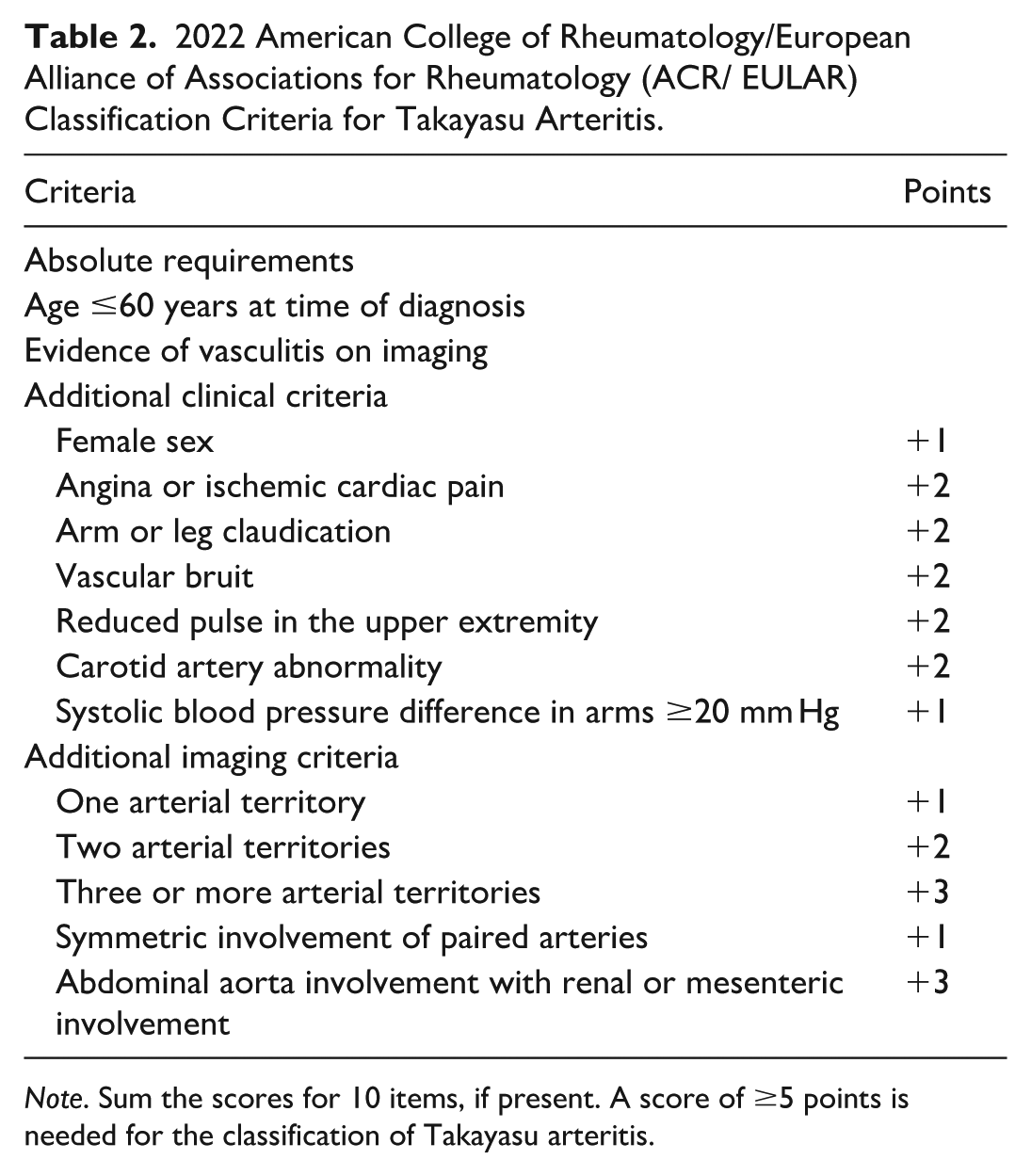
Note. Sum the scores for 10 items, if present. A score of ≥5 points is needed for the classification of Takayasu arteritis.
Clinical Course and Medical Management (2016-2024)
The patient was initially treated with systemic glucocorticoids and immunosuppressive therapy. Methotrexate was used first but discontinued due to inadequate response, and she was transitioned to rituximab infusions in 2016. Despite treatment, carotid DUS performed in 2016 demonstrated progression to complete occlusion of the right CCA with distal reconstitution and persistent stenosis of the left carotid and subclavian arteries.
Subcutaneous tocilizumab therapy was initiated in mid-2016, resulting in improvement of headaches and left upper extremity paresthesia. Over subsequent years, the patient experienced periods of clinical stability while on tocilizumab, with repeated normalization of inflammatory markers, including erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). However, during multiple intervals of intentional or unintentional cessation of tocilizumab (notably in 2018, 2019, and 2021), she developed symptoms of generalized inflammation (severe fatigue, headaches, myalgias, fever) and symptoms of ischemia including left arm paresthesia, prompting the reinitiation of therapy. These episodes occurred despite persistently normal inflammatory markers, consistent with suppression of acute-phase reactants during interleukin (IL)-6 blockade.
Throughout the disease course, disease activity was defined clinically, based on the recurrence of inflammatory and ischemic symptoms, progression of physical examination findings (including diminished pulses and audible bruits), and interval imaging changes, rather than laboratory markers alone. Neurologic evaluations, including transcranial Doppler studies performed in 2020, demonstrated preserved intracranial flow and cerebrovascular reserve, with no evidence of completed stroke. Given the absence of critical ischemia, preserved cerebral perfusion, and the increased risk of complications associated with revascularization during active inflammatory disease, surgical or endovascular intervention was repeatedly deferred in favor of continued medical management with close surveillance. The patient’s longitudinal clinical course, imaging findings, laboratory results, symptoms, and treatment modifications are summarized in Table 3 which can be found in supplemental material.
Comparison of Early (2016) and Late (2024) Duplex Ultrasound Findings
Diagnosis of TA was confirmed in 2016 by carotid DUS, which demonstrated complete occlusion of the right CCA with visualization of collateral flow (Figure 1A). Eight years later, follow-up DUS performed in 2024 revealed restoration of central intraluminal color flow within the right CCA (Figure 1B), consistent with recanalization or, less likely, neovascularization from the adventitial vasa vasorum. The central distribution of color flow favored partial recanalization. This finding suggests hemodynamic improvement in a previously occluded segment, although it does not imply complete reversibility of disease, as flow in the right ECA remained retrograde, providing blood supply to the right ICA. A summary of the major duplex ultrasound findings and vascular changes observed between 2016 and 2024 is presented in Table 4 which can be found in supplemental material.
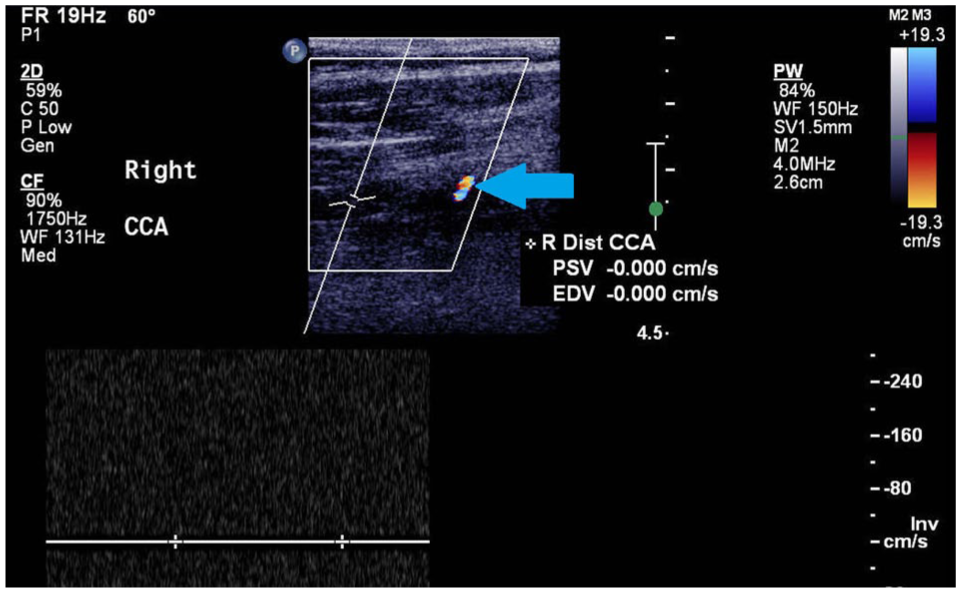
Occlusion in the right common carotid artery.
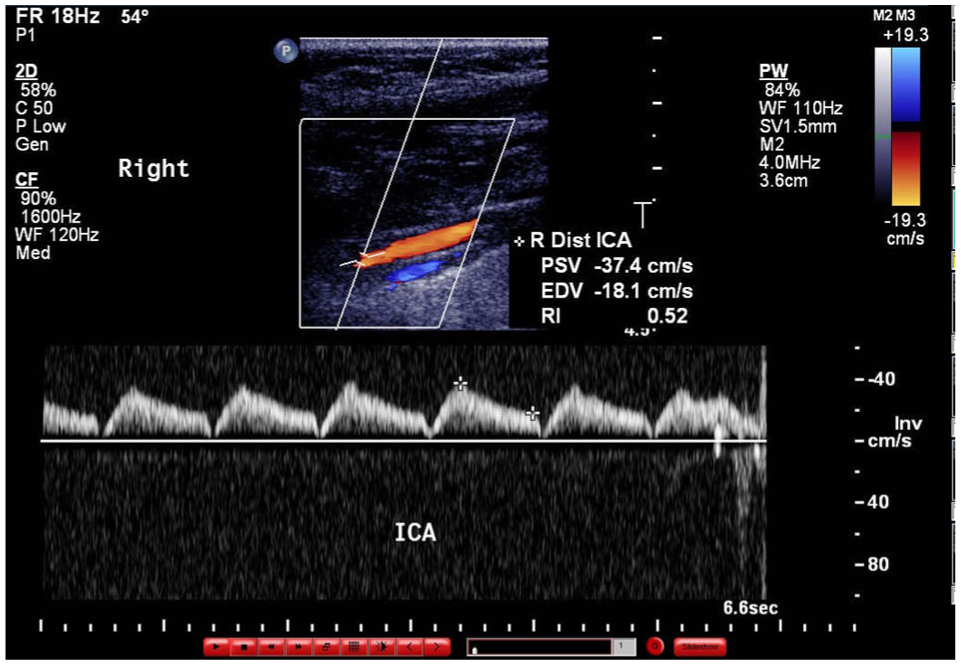
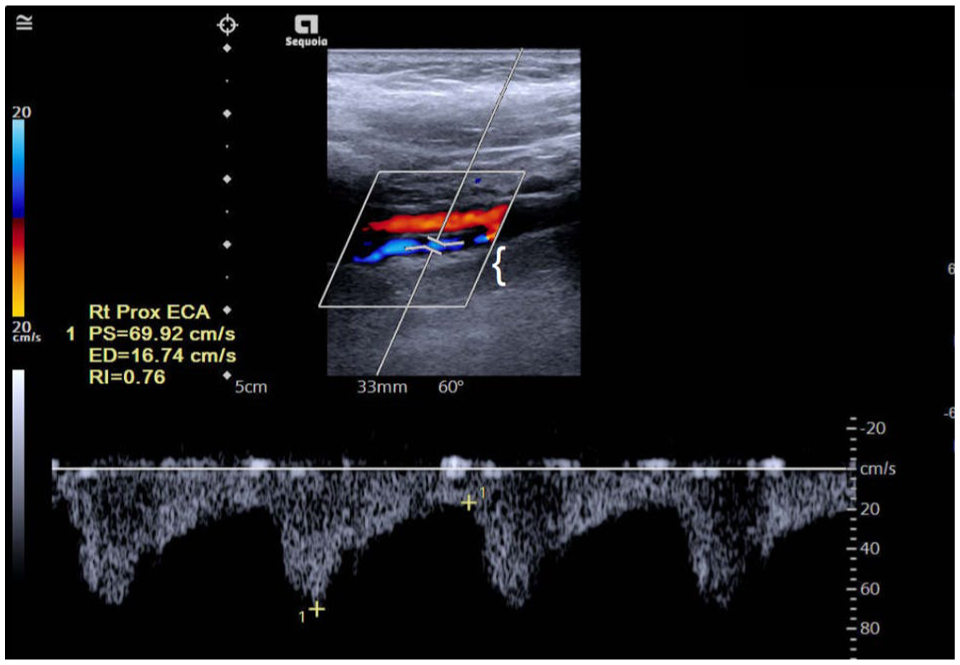
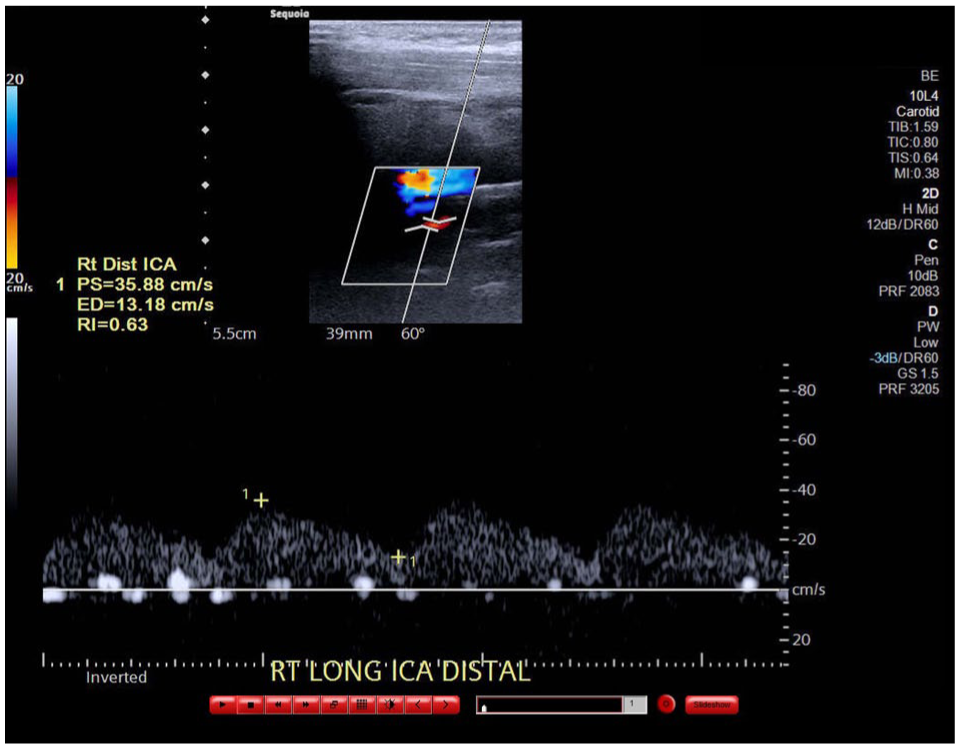
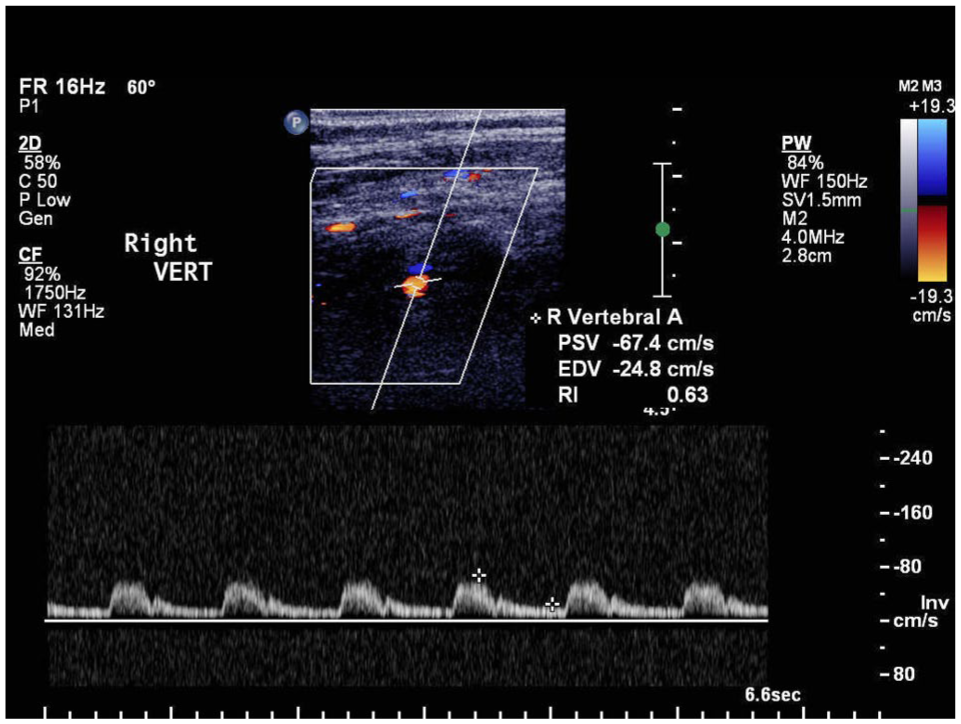
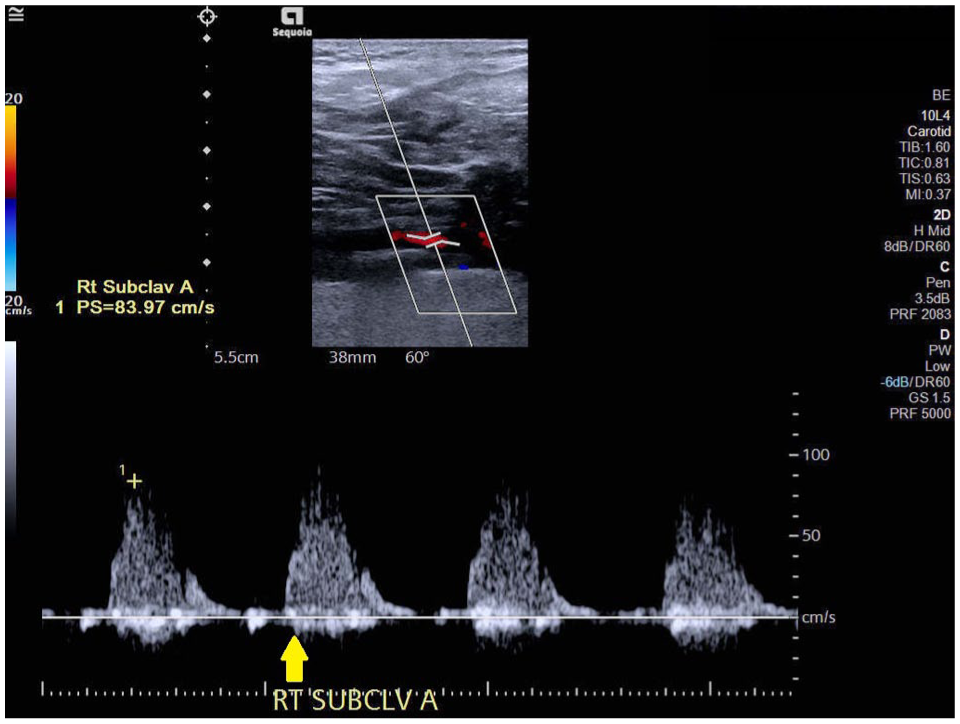
Comparison of the 2 time points demonstrated heterogeneous vascular evolution. In 2016, retrograde flow in the right ECA supplying the right ICA was observed (Figure 1C), with no significant change noted on the 2024 examination (Figure 1D). The right ICA remained patent in both 2016 and 2024, with persistent retrograde flow in the right ECA supplying the right ICA (Figure 1E and F). Spectral Doppler interrogation of the right proximal subclavian artery showed progression to abnormal monophasic waveforms by 2024, consistent with increased proximal stenosis (Figure 1G and H). The right vertebral artery demonstrated predominantly antegrade flow with a small systolic flow reversal, producing a characteristic “V”-shaped waveform notch suggestive of early subclavian steal physiology (Figure 1I and J).
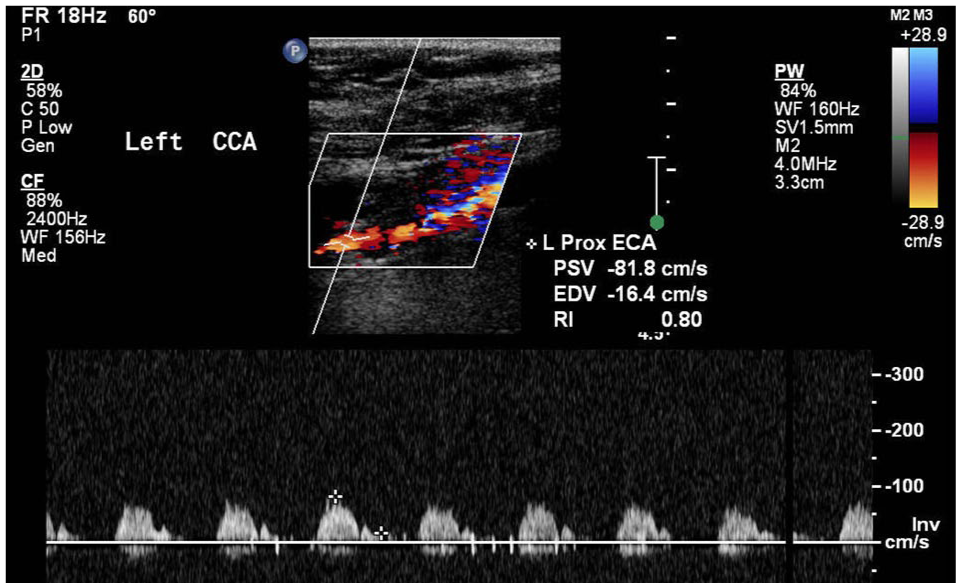
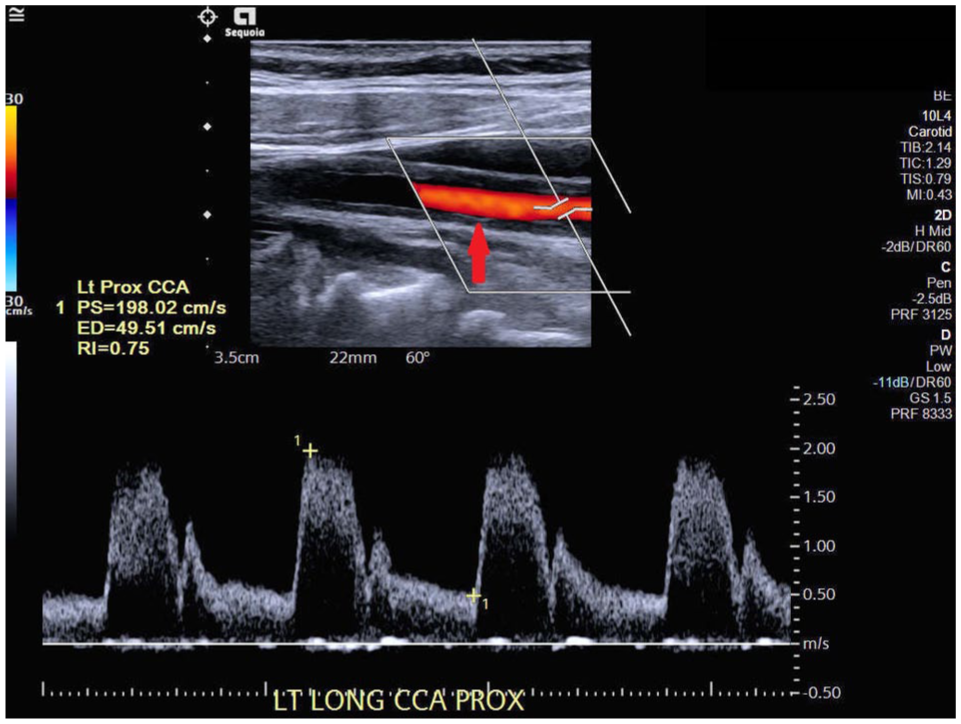
At initial diagnosis, arterial wall thickening of the left CCA resulted in disturbed color flow and elevated velocities (Figure 2A). By 2024, DUS demonstrated progression of stenosis, exceeding 50% in the proximal and mid segments and greater than 70% in the distal segment (Figure 2B). The left ECA exhibited an elevated peak systolic velocity exceeding 150 cm/s, consistent with greater than 50% stenosis (Figure 2C and D). While narrowing of the left ICA was present in 2016 (Figure 2E), the 2024 examination demonstrated heterogeneous plaque extending into the proximal ICA with less than 50% stenosis (Figure 2F).
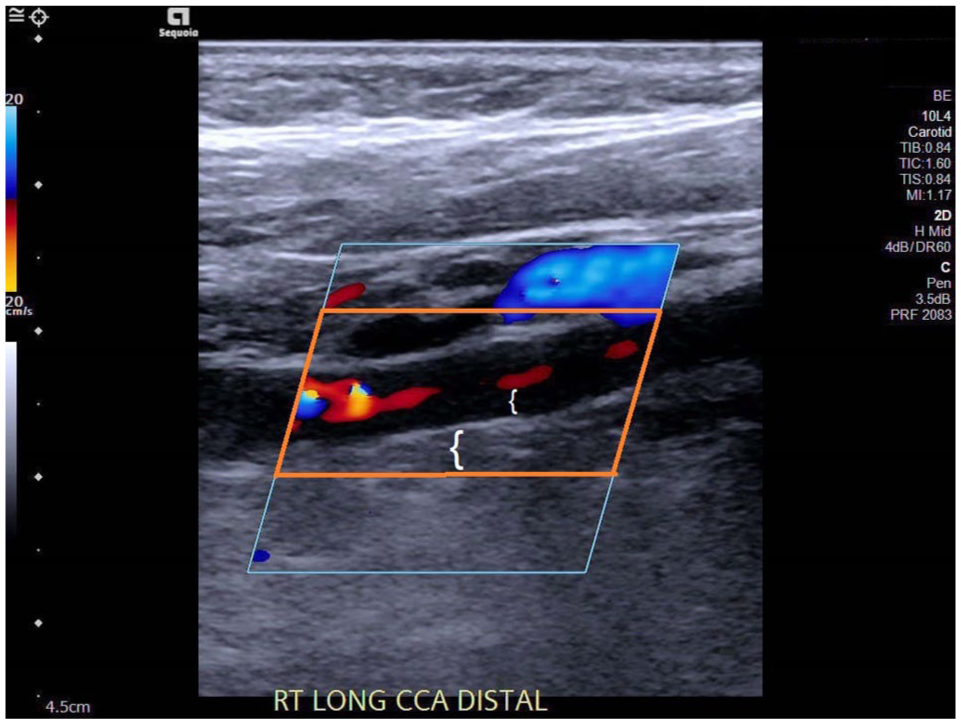
Recanalization in the right common carotid artery with reduced velocities in the mid and distal segment.
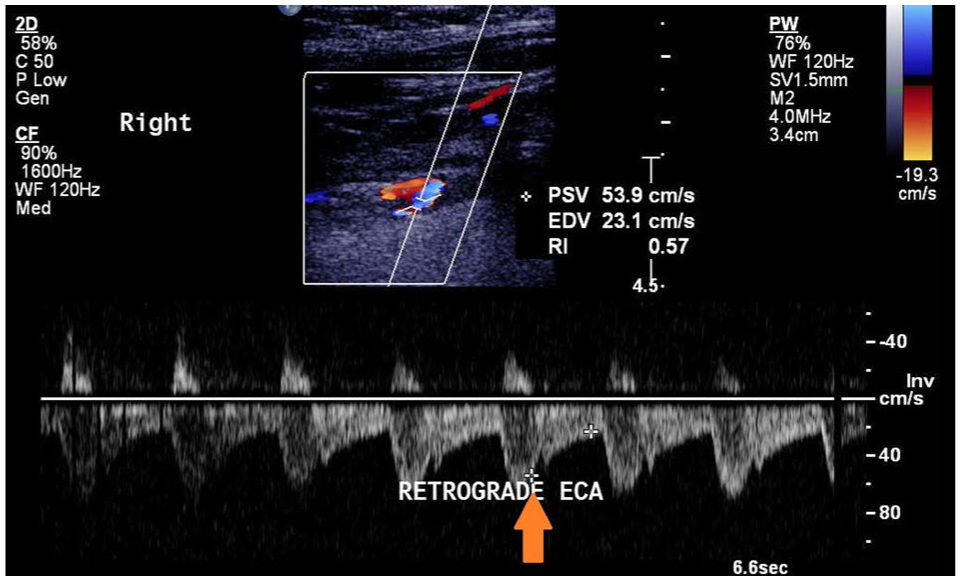
Retrograde flow in the right external carotid artery (blue color Doppler), feeding into the internal carotid artery with anterograde flow (red color Doppler). No significant change noticed eight years later.
Scan of the same arterial segment eight years later reveals no significant change.
The right internal carotid artery is patent. Retrograde flow in the right external carotid artery, feeding into the right internal carotid artery was observed.
Retrograde flow in the right external carotid artery, feeding into the right internal carotid artery was confirmed.
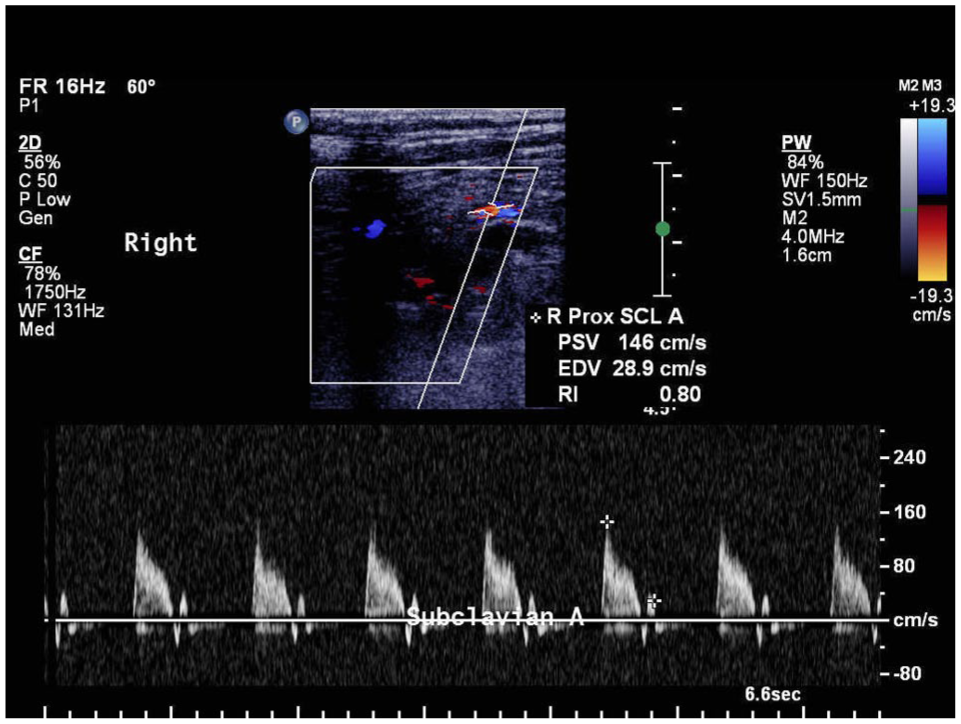
Normal waveform, elevated velocities in the right subclavian artery.
There is abnormal monophasic Doppler waveforms in the right proximal subclavian artery, suggestive of more proximal stenosis.
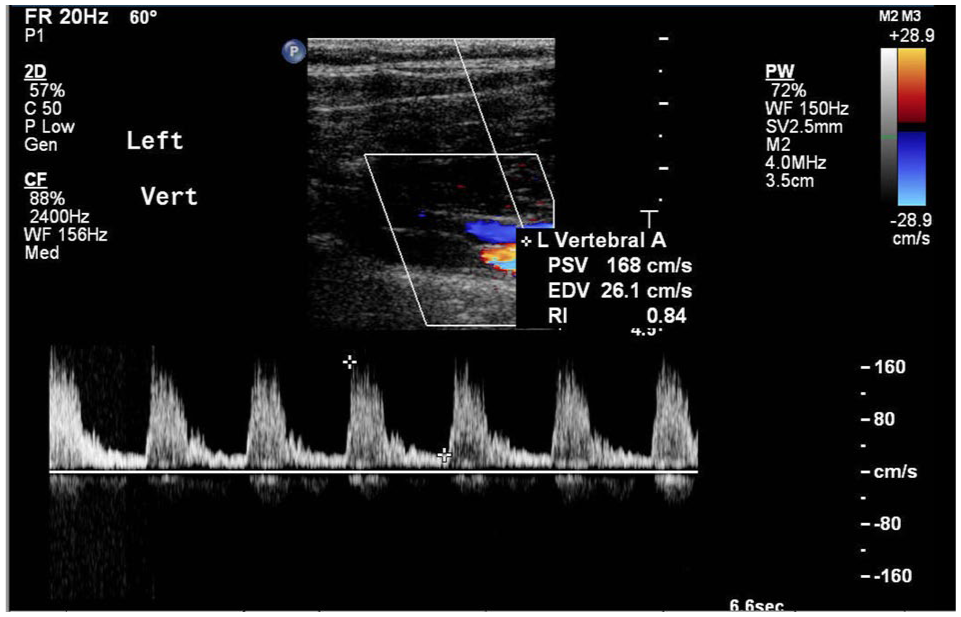
Normal waveform and velocities in the right vertebral artery.
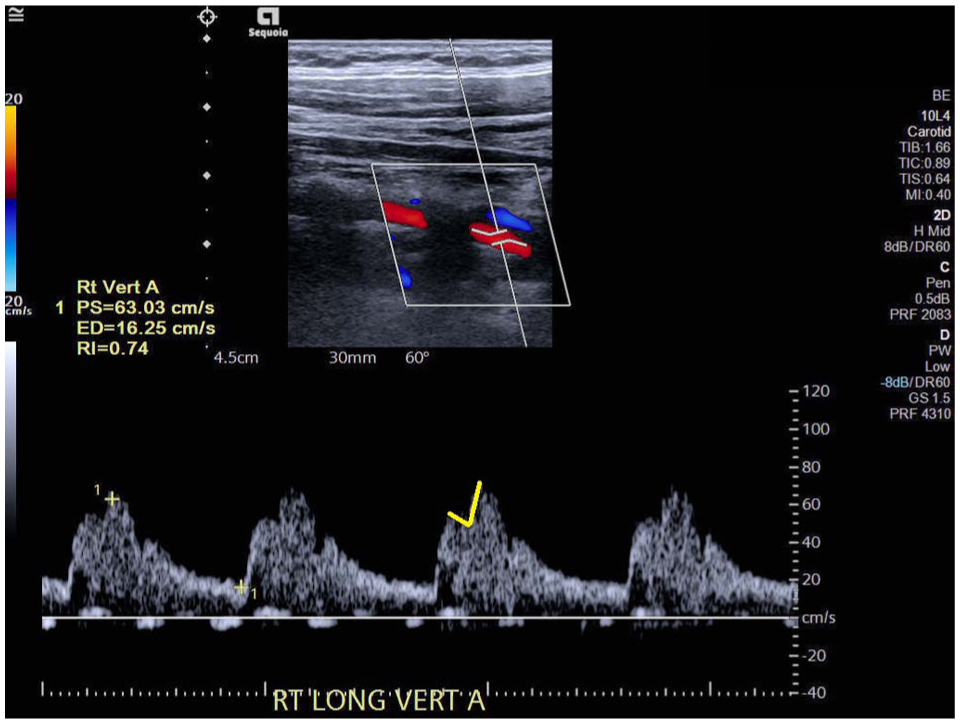
There is predominantly antegrade flow noted in the right vertebral artery with minimal reversed flow as noted by the “ V “ shape cut out in the waveform at the top of the systolic peak. (yellow marking).
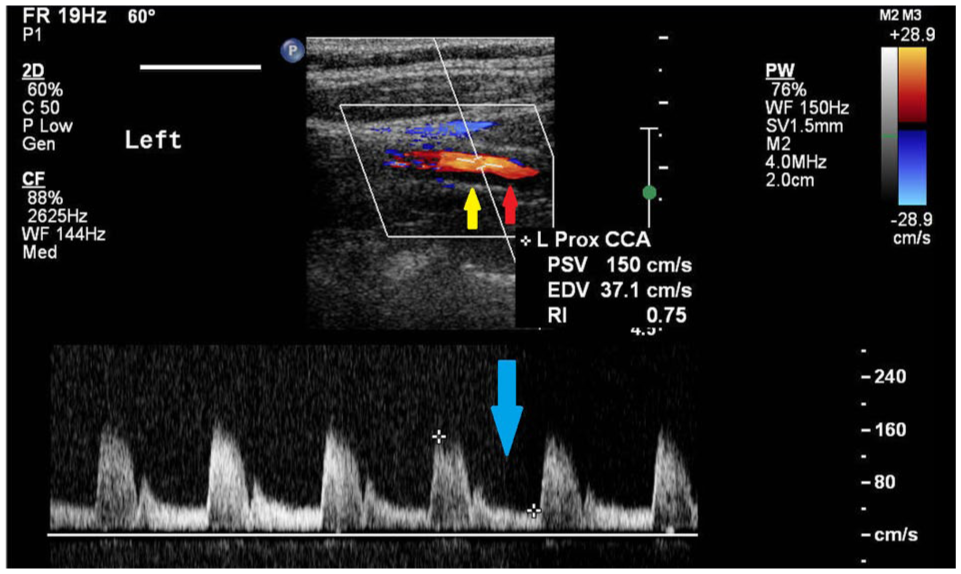
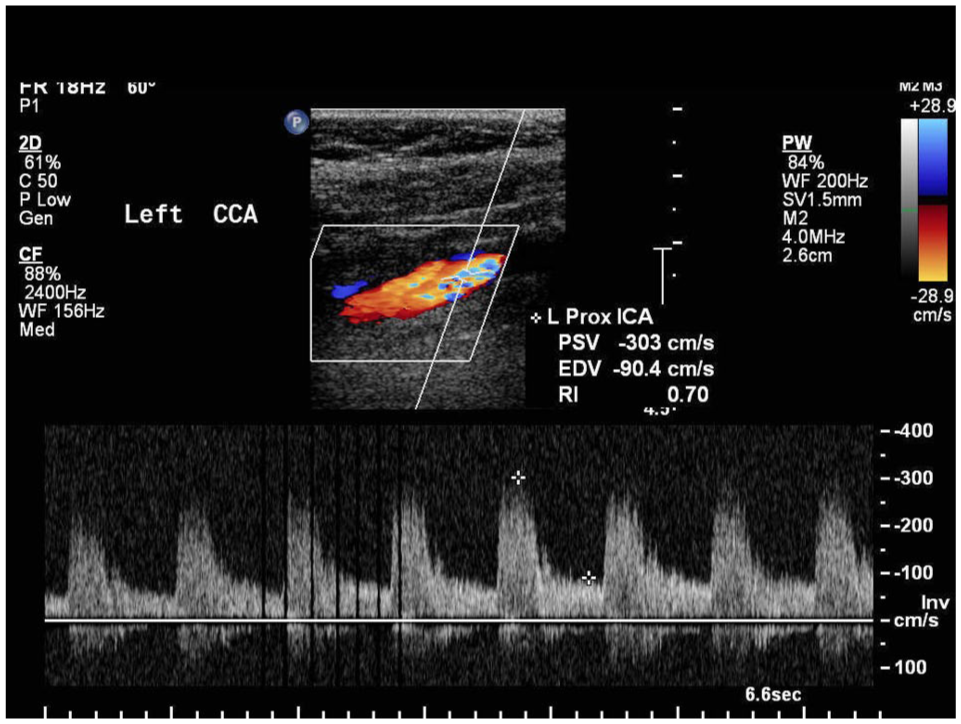
Arterial wall thickening in the left common carotid artery (LCCA) causing elevated velocities and disturbed color flow throughout the vessel.
Significant stenosis was identified in the proximal and middle (>50%) and distal (>70%) segments of the LCCA.
Normal low resistance pattern in the left external carotid artery.
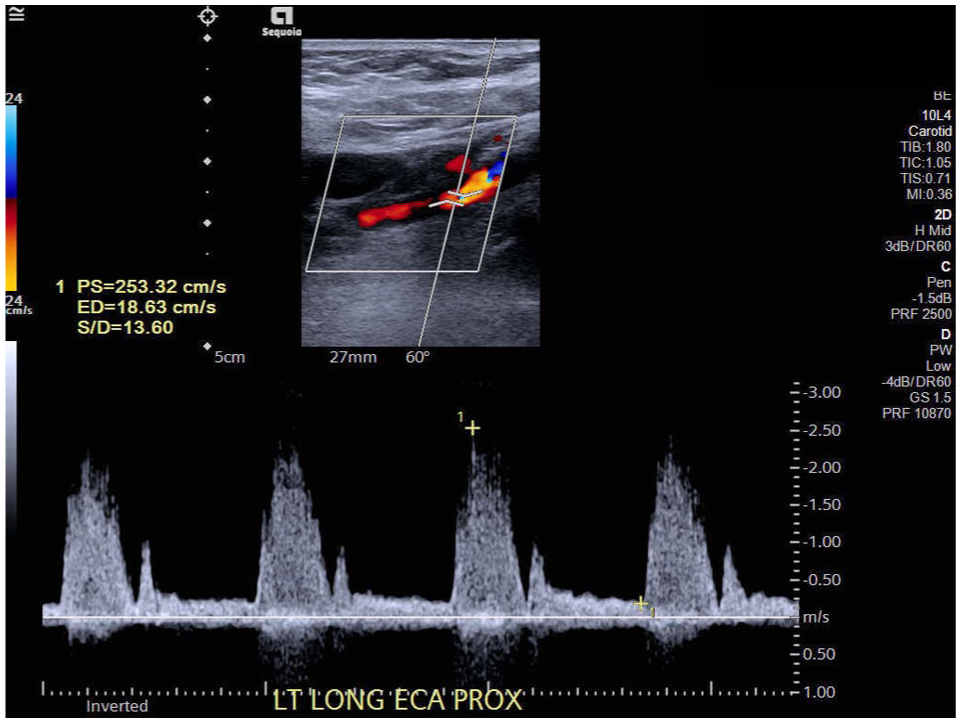
Elevated velocity in the left external carotid artery indicates a greater than 50% stenosis. (PSV >150 cm/s).
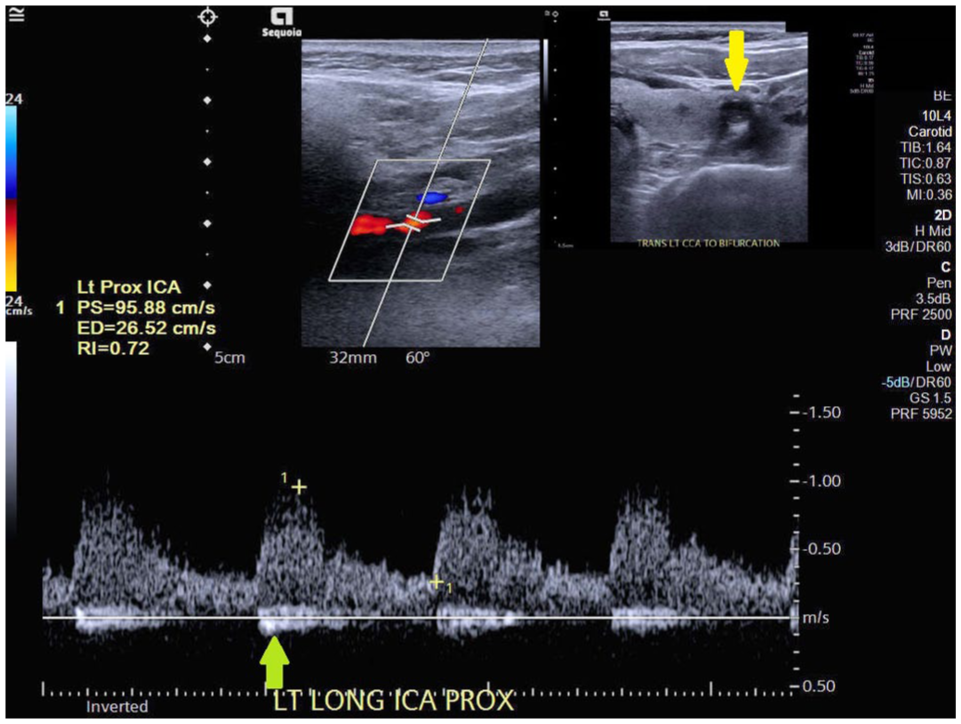
Narrowing of the left internal carotid artery (ICA). There are elevated velocities throughout the internal carotid artery.
Less than 50% stenosis in the left bulb and internal carotid artery. There is heterogenous plaque in the bulb extending into the proximal internal carotid artery (yellow arrow).
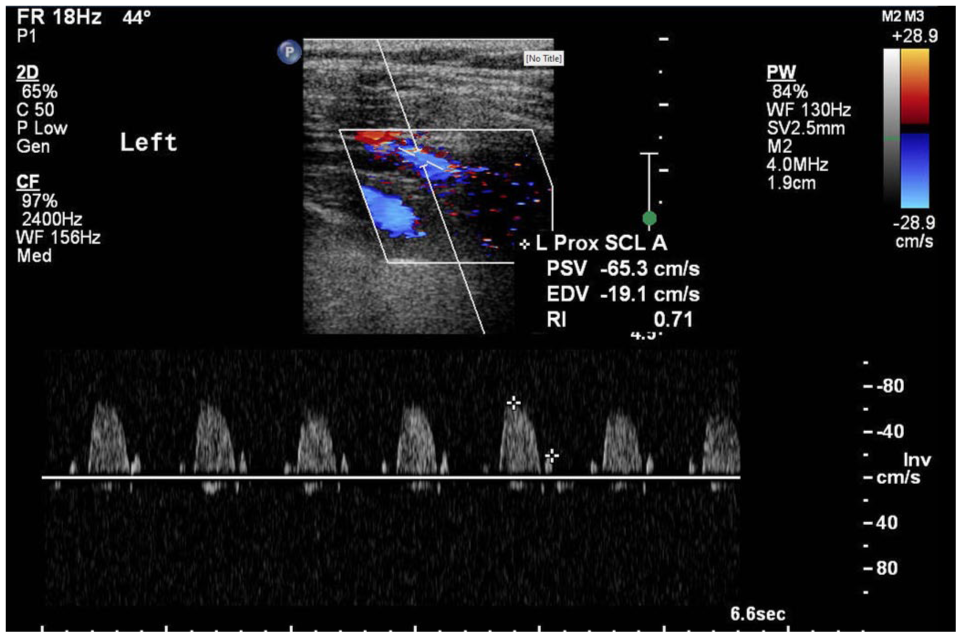
Normal, high resistance pattern in the left subclavian artery.
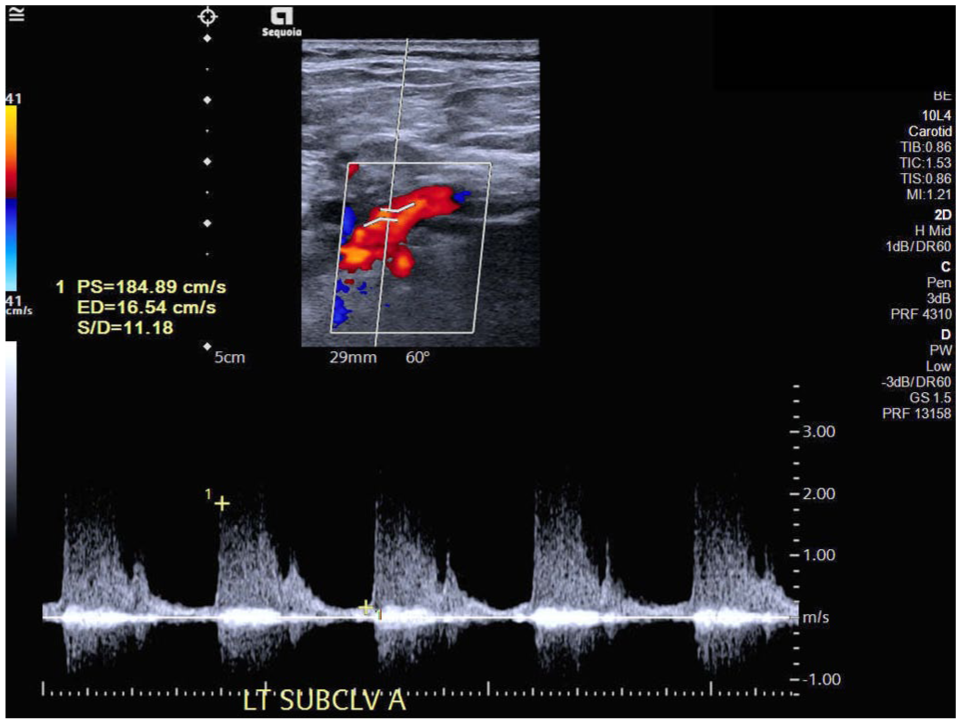
Elevated velocities in the proximal left subclavian artery suggests disease progression.
Normal, anterograde flow in the left vertebral artery.
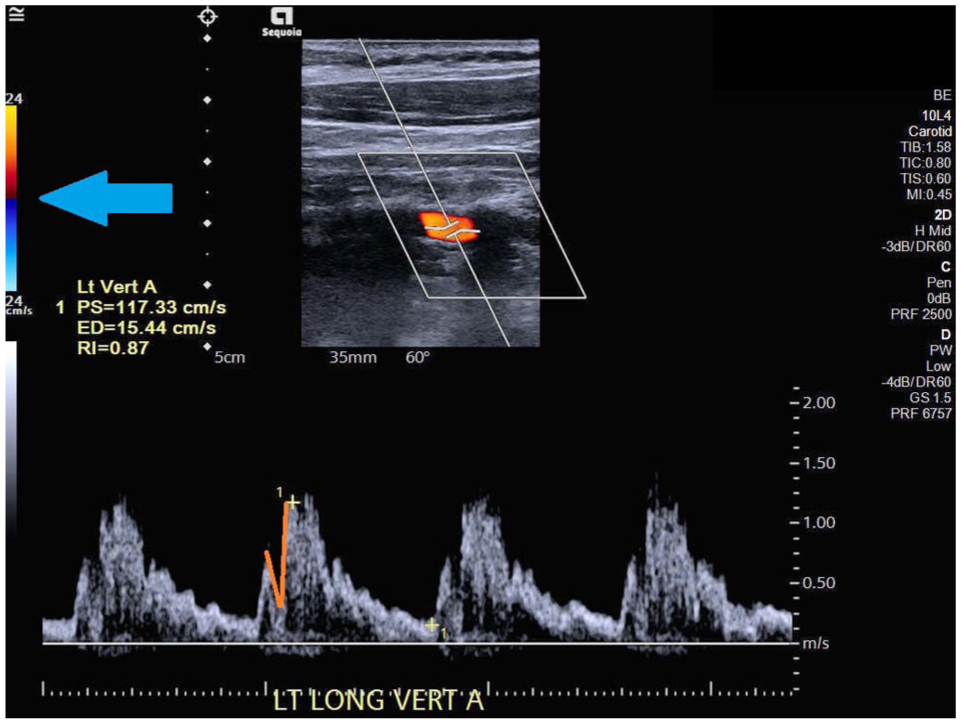
“V” shape cut out (near rabbit sign) noted in the left vertebral artery suggests proximal stenosis in the left subclavian artery. (orange marking).
Additional progression was noted in the left proximal subclavian artery, with elevated velocities compared to the 2016 examination (Figure 2G and H). The left vertebral artery demonstrated a “V”-shaped systolic notch resembling an early rabbit sign (Figure 2I and J), consistent with evolving subclavian steal physiology. These imaging findings correlated with the patient’s contemporary symptoms, including worsening fatigue, left arm numbness, and exertional upper extremity claudication, supporting the assessment of active disease in 2024.
Discussion
This case report presents a 2-time-point DUS comparison in a patient with TA, contextualized by an 8-year clinical disease course. While serial imaging was not performed at regular intervals, comparison of early and late DUS examinations provides valuable insight into the heterogeneous vascular evolution characteristic of TA under prolonged medical management. Such detailed integration of clinical history and vascular ultrasound findings remains relatively limited in the literature and contributes to a more nuanced understanding of disease behavior over time.
A key observation in this case is the dissociation between inflammatory biomarkers and clinical or imaging evidence of disease activity. Throughout the disease course, the patient experienced recurrent inflammatory and ischemic symptoms—most notably fatigue, headaches, upper extremity paresthesia, and exertional claudication—often coinciding with interruption or cessation of IL-6 receptor blockade. These episodes were accompanied by progression of physical examination findings, including diminished pulses and prominent bruits, and supported by interval DUS changes, despite repeatedly normal ESR and CRP values. Accordingly, disease activity in this patient was defined primarily by clinical presentation and imaging findings rather than laboratory markers alone, consistent with known limitations of inflammatory markers in patients receiving IL-6 inhibition.
Medical Management vs Surgical or Endovascular Intervention
Initial medical therapy for TA typically consists of systemic glucocorticoids combined with a non-glucocorticoid immunosuppressive agent. Methotrexate is commonly used as first-line adjunct therapy, while biologic agents are recommended for patients with refractory disease or glucocorticoid intolerance. In this case, treatment included tocilizumab, a humanized monoclonal antibody targeting IL-6, a cytokine highly expressed in inflamed arterial tissue. 1 The patient demonstrated repeated symptomatic improvement while receiving IL-6 receptor blockade, with recurrence of symptoms during periods of treatment interruption.
Surgical and endovascular treatment options for TA include percutaneous transluminal angioplasty, stent placement, stent grafting, and open bypass surgery. These interventions are generally reserved for patients with critical ischemia, aneurysmal disease, or severe aortic valve involvement and are relatively contraindicated during periods of active arterial inflammation, as procedural complication rates are higher and long-term patency is reduced when interventions are performed in the inflammatory phase.1,8 Current guidelines emphasize achieving inflammatory disease control with medical therapy before considering revascularization.
In this patient, multidisciplinary evaluation consistently favored continued medical management. Despite extensive large-vessel involvement, she demonstrated preserved intracranial perfusion on transcranial Doppler studies, the absence of completed stroke, and only intermittent ischemic symptoms. These factors, together with evidence of active or smoldering inflammatory disease at several time points, supported deferral of surgical or endovascular intervention in favor of immunosuppressive therapy and close imaging surveillance.
Interpretation of Duplex Ultrasound Findings
Comparison of early (2016) and late (2024) DUS examinations demonstrated heterogeneous vascular remodeling, with progression of stenosis in some arterial segments and partial restoration of flow in others. The appearance of central intraluminal color flow within the previously occluded right CCA at late follow-up was interpreted as consistent with recanalization or, less likely, neovascularization from the adventitial vasa vasorum. While this finding suggests hemodynamic improvement within a previously occluded segment, it does not imply complete reversibility of the underlying vasculitic process.
Conversely, progression of stenosis within the left common carotid, external carotid, and subclavian arteries, along with the development of heterogeneous plaque and abnormal monophasic waveforms, reflected chronic fibrotic remodeling. The identification of early subclavian steal physiology, manifested by characteristic vertebral artery waveform changes, further illustrates the ability of DUS to detect clinically relevant hemodynamic adaptation before the onset of critical ischemia. Together, these findings highlight the utility of DUS in characterizing not only anatomic stenosis but also flow direction, waveform morphology, and compensatory mechanisms in TA.
Differentiation of Vasculitis From Atherosclerotic Disease
Differentiating vasculitic lesions from atherosclerotic disease using DUS can be challenging, as both may present with arterial wall thickening and luminal narrowing.8,9
However, key distinguishing features can aid differentiation. 10 TA lesions typically occur in younger patients and demonstrate long, concentric, and homogeneous arterial wall thickening, often described as the “macaroni sign,” particularly within the common carotid arteries. 11 In contrast, atherosclerosis more commonly affects older individuals and is characterized by focal, eccentric, heterogeneous plaques that may be calcified and produce irregular vessel contours.12,13
In this case, the patient’s age at presentation, diffuse large-vessel involvement, and early imaging findings favored vasculitis as the primary pathology. The later development of heterogeneous plaque, particularly within the carotid bulbs (Figure 2F), likely reflects a combination of chronic inflammatory injury and secondary atherosclerotic change. Careful assessment of lesion morphology, distribution, and clinical context is therefore essential when interpreting ultrasound findings in long-standing TA.
Limitations
Interpretation of imaging findings may be subject to observer bias, and causality between medical therapy and imaging changes cannot be definitively established. Nonetheless, integration of detailed clinical data with objective DUS findings strengthens the interpretation and clinical relevance of this case. Larger studies with standardized longitudinal imaging are needed to further define ultrasound markers of disease activity and long-term vascular remodeling in TA. One limitation to ultrasound is its user-dependency; for example, accurate velocity measurement is largely reliant on proper angle correction.
Conclusions
This 2-time-point DUS comparison illustrates the complex and heterogeneous vascular evolution of TA under medical management, demonstrating both progressive stenosis and partial restoration of arterial flow across different vascular territories. Duplex ultrasound proved valuable in documenting arterial wall morphology, flow direction, and hemodynamic adaptation, providing clinically meaningful information beyond laboratory markers alone.
Ongoing ultrasound surveillance supports longitudinal clinical assessment by identifying chronic vascular remodeling, collateralization, and evolving stenosis, thereby reinforcing its role in the long-term management of TA. Larger studies incorporating standardized imaging intervals and extended follow-up are needed to further define ultrasound correlates of disease activity and treatment response.
Supplemental Material
sj-docx-1-jvu-10.1177_15443167261460998 – Supplemental material for Early vs Late Arterial Wall Changes in Takayasu Arteritis Assessed by Duplex Ultrasound
Supplemental material, sj-docx-1-jvu-10.1177_15443167261460998 for Early vs Late Arterial Wall Changes in Takayasu Arteritis Assessed by Duplex Ultrasound by Hana Dakhlaoui, Adam Bardoczi, Melinda Majsai, Steven To and Zsolt Garami in Journal for Vascular Ultrasound
Footnotes
Acknowledgements
The authors thank Michelle Swick for her thorough review and edits of the manuscript and Steven To for his thorough review of the ultrasound images.
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series. The images displayed in the figures contain no patient identifiers.
Consent to Participate
Consent was obtained from the patient as part of our institution’s general consenting process.
Consent for Publication
Consent was obtained from the patient as part of our institution’s general consenting process, which includes case publications.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.