
Abstract
Background.
Persistent post-stroke ankle impairment hinders functional recovery. Brain-computer interface (BCI)-controlled ankle robot show rehabilitation potential, but their efficacy and underlying neuroplasticity remain unclear.
Objective.
To assess BCI-controlled ankle robot training on post-stroke lower-limb motor recovery and neuroplasticity using quantitative EEG (qEEG).
Methods.
Thirty-two stroke patients were randomized to BCI (n = 16, 40-minute BCI-robot training) or control (n = 16, 40-minute ankle-robot training) groups, receiving 5 sessions/week for 2 weeks. Outcomes included Fugl-Meyer Assessment-Lower Extremity (FMA-LE), Berg Balance Scale (BBS), Functional Ambulatory Category (FAC), Modified Ashworth Scale (MAS), active range of motion (AROM), and muscle strength. QEEG assessed the relative power of the delta (rδ), theta (rθ), alpha (rα), beta (rβ) bands, spectral power ratios, pairwise-derived Brain Symmetry Index (pdBSI), and functional connectivity.
Results.
Both groups showed significant within-group improvements in dorsiflexion AROM, dorsiflexor strength, FMA-LE, BBS, and FAC (P < .05). The BCI group demonstrated significantly greater FMA-LE improvement than controls (∆FMA-LE, P = .007) and reduced calf spasticity (MAS; P = .038). QEEG analysis in the BCI group revealed decreased rδ (P = .005), increased rα (P = .017), reduced DAR and DTABR (P < .05), reduced interhemispheric asymmetry (pdBSI-δ; P = .018), and enhanced Cz-parietal connectivity in α and β bands (P < .05).
Conclusion.
BCI-controlled ankle robot training significantly improved lower-limb motor function and reduced spasticity post-stroke. Associated neurophysiological changes, characterized by reduced slow-wave power and asymmetry, increased alpha power, and functional connectivity, indicated beneficial neuroplastic reorganization.
Keywords
Introduction
Stroke is a leading cause of global mortality and chronic disability, ranking as the second most common cause of death worldwide. 1 This neurological disorder frequently disrupts lower-limb motor control, impairing postural stability, ambulation, and the activities of daily living. Up to 80% of stroke survivors exhibit persistent gait deficits, with foot drop being one of the most predominant impairments due to compromised ankle dorsiflexion. As a critical determinant of gait biomechanics, the ankle governs dynamic balance and modulates proximal joint kinematics during locomotion, including hip and knee flexion. Impaired dorsiflexion exacerbates spatiotemporal asymmetry, provoking compensatory patterns such as circumduction gait. Despite conventional rehabilitation strategies, functional gains typically plateau within 6 to 8 months post-stroke.2,3 Assistive devices like ankle-foot orthoses provide transient improvements but fail to confer sustained recovery after discontinuation. Emerging neurotechnologies—such as robotic exoskeletons, functional electrical stimulation (FES), non-invasive brain stimulation, and brain-computer interfaces (BCIs)—now enable high-intensity, targeted motor training, even in severe impairment. 4 These interventions can engage cortico-muscular pathways, fostering neuroplastic remodeling to enhance functional restoration.5,6
Motor imagery-based BCIs (MI-BCIs) represent a promising neurorehabilitation tool, especially for patients with moderate-to-severe motor impairments where voluntary movement is limited. 7 These systems detect movement intention through electroencephalographic (EEG) signals and translate them into robotic-assisted passive movement of the affected limb, reinforcing the cortico-motor connection between intention and execution. Specific EEG feature patterns trigger external device activation, providing real-time feedback and creating a closed-loop rehabilitation paradigm. 8 Despite these advances, lower extremity (LE) rehabilitation using BCI technology remains underexplored compared to upper limb applications. The key challenges include difficulty in decoding LE kinematic and kinetic parameters from non-invasive recordings. 9 Existing studies on LE-BCI interventions for stroke rehabilitation are challenged by methodological limitations, including small sample sizes, wide confidence intervals, and variable study quality, which prevent definitive conclusions from being made.5,10 Our group previously developed an MI-BCI-controlled ankle robot system and demonstrated its feasibility for motor recovery. However, rigorous randomized controlled trials (RCTs) comparing its efficacy against conventional ankle-robot training are lacking. Thus, this study aimed to address this gap by conducting an RCT to evaluate whether BCI-controlled ankle robot training could achieve motor recovery superior to that of standard robotic training. We hypothesize that the BCI-integrated approach can yield significantly greater improvements in post-stroke lower limb function compared to standard robotic training.
Quantitative electroencephalography (qEEG) provides a clinically accessible method to evaluate cortical engagement during rehabilitation, with active participation shown to promote corticospinal plasticity and improve motor recovery outcomes. 11 Unlike other neuroimaging modalities, EEG offers the cost-effective monitoring of neural dynamics with millisecond temporal resolution, making it particularly valuable for investigating neurorehabilitation mechanisms. Emerging evidence suggests that pathological EEG patterns, including elevated slow-wave power and increased power ratio indices (PRI), correlate with poorer motor function and unfavorable prognosis post-stroke. Given the prevalence of interhemispheric dysregulation after stroke, asymmetry metrics, such as the Brain Symmetry Index (BSI), revised BSI, and pairwise-derived BSI (pdBSI), have demonstrated usefulness in predicting and tracking rehabilitation progress.12,13 Additionally, EEG-derived functional connectivity (FC) measurements, which quantify synchronization between cortical regions, are being increasingly recognized as biomarkers of functional recovery. 14 In this study, we used qEEG features to quantify the neuronal changes brought about by the ankle robot and BCI interventions. We hypothesize that BCI may enhance brain symmetry, and increase relative power values and functional neural connectivity, thereby facilitating efficient neural functional remodeling.
Methods
Study Design
This study was an assessor-blinded randomized controlled trial. It was conducted in accordance with the Declaration of Helsinki, Good Clinical Practice guidelines, and the Consolidated Standards of Reporting Trials (CONSORT). The research received approval from the local Ethics Committee at Beijing Tsinghua Chang Gung Hospital Medical Ethics (23329-0-02) and was registered as a clinical trial (ChiCTR2300074381).
Randomization
Randomization was carried out using a computer-generated sequence. A researcher, who was independent of participant recruitment and assessment, managed the randomization process. Each participant was given a unique identification number, and a random number generator was used to assign them (1:1) to either the BCI group or the ankle-robot group.
Participants and Sample Size
Participants hospitalized in the Department of Rehabilitation Medicine at Tsinghua Changgung Hospital in Beijing were recruited for the study. The following inclusion criteria were applied: (1) first episode of stroke, with pure unilateral motor paresis after the stroke, a course of illness within 6 months, and stable vital signs; (2) sufficient cognition to follow simple instructions and understand the content and purpose of the study; (3) no significant cognitive impairment, no auditory comprehension disorders, able to cooperate with assessments and treatment, a Mini-Mental State Examination score of ≥21, and confirmed by the Kinesthetic and Visual Imagery Questionnaire 15 as being capable of independently performing motor imagery tasks; and (4) manual muscle testing scores of ankle dorsiflexion and plantarflexion between 0 and 4 and lower limb Modified Ashworth Scale scores between 0 and 3.
The exclusion criteria comprised: (1) patients with severe dysphasia with inadequate communication; (2) any additional medical or psychological condition affecting the ability to comply with the study protocol; and (3) a history of other neurological disease, psychiatric disorders, including epilepsy, alcoholism, or substance abuse. Written informed consent was obtained from each participant before the start of the experiments following a protocol approved by the local Institutional Review Board.
The Sample Size
The sample size was calculated using G*Power 3.1.9.7 software, with the change of FMA-LE after training (∆FMA-LE) as the primary outcome measure. 16 A 2-tailed t-test was used for statistical analysis, with a significance level of α = 0.05 and power of 1 − β = 0.85. The sample size ratio between the experimental group and the control group was set at 1:1, a total of 32 stroke patients were required. Considering a 20% dropout rate, 40 stroke patients were required, with 20 participants in each group.
Intervention
Both groups continued movement exercises for ankle mobility and strength for 2 weeks. Subjects in the experimental group had BCI-controlled ankle robot training 5 times a week for 2 weeks at 40 minutes/session, and the control group had ankle-robot training 5 times a week for 2 weeks at 40 minutes/session.
MI-BCI-Controlled Ankle Robot Training
EEG Acquisition
Scalp EEG signals were collected from a 64-channel gel-based electrode cap (according to 10-20 International System). The data were amplified and digitized at 24-bit resolution, with a sampling rate of 1000 Hz (Neuracle Medical Technology [Shanghai] Co., Ltd.). The ground electrode was positioned at AFz and the reference electrode at CPz. All electrode impedances were balanced below 20 kΩ with the participants seated motionlessly. EEG channels over sensorimotor regions (FC2, FC4, FC6, C2, C4, C6, CP2, CP4, CP6, FC5, FC3, FC1, C5, C3, C1, CP5, CP3, and CP1) were used for online analyses and real-time ankle-robot control.
MI-BCI Paradigms
The participants received standardized instructions to perform only motor imagery tasks while avoiding attempts to move the affected lower limbs. Prior to formal training, a trained therapist explained the protocol and precautions, and provided motor imagery skill training to the experimental group. The complete training consisted of 2 stages: the model training stage and the rehabilitation training stage. The BCI-controlled ankle robot training (W3, Neuracle Medical Technology [Shanghai] Co., Ltd.; FSM-C-AN, Beijing Litecare Medical Technology Co., Ltd.) is shown in Figure 1(A) and (B).
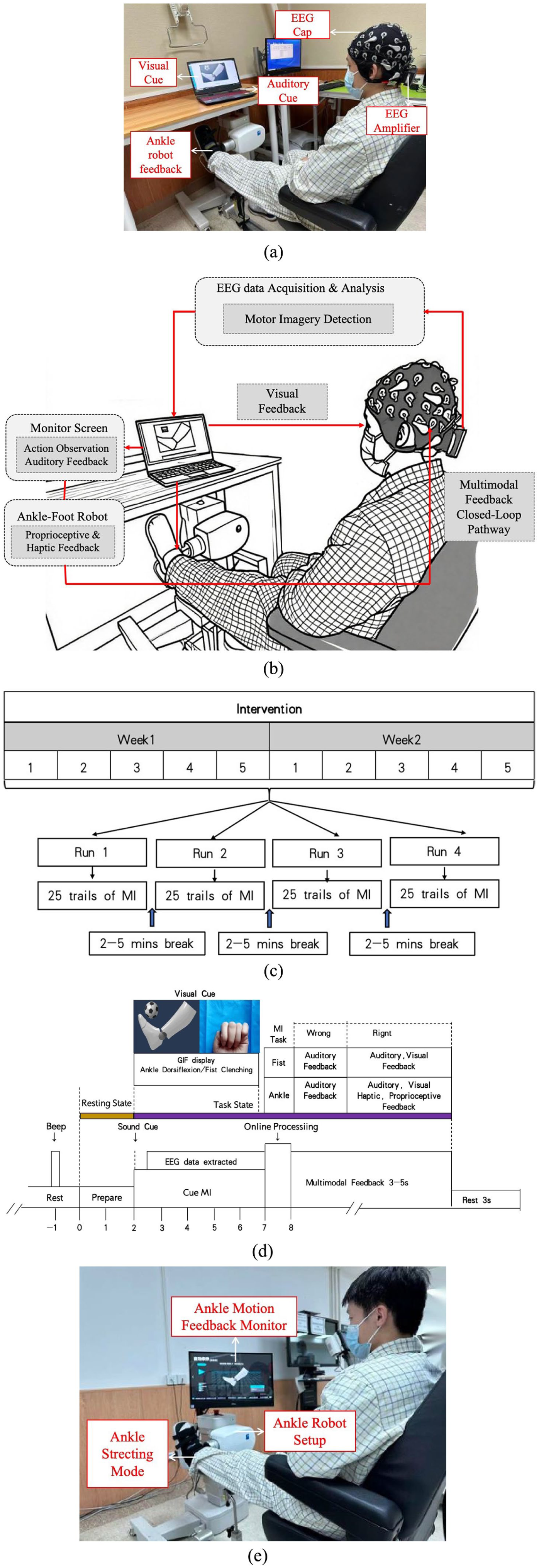
(A) BCI-controlled ankle robot setup for stroke rehabilitation, showing the EEG cap, EEG amplifier, monitor, and ankle robot. (B) System operation: Participants imagine ankle dorsiflexion or fist clenching. Upon detecting the correct neural pattern, the robot assists passive ankle dorsiflexion, providing real-time proprioceptive, visual, and auditory feedback. (C) Intervention progression. (D) Timing for kinesthetic motor imagery and robotic feedback. (E) Setup of ankle robot intervention.
Prior to each session, an individualized passive stretch assessment established 2 thresholds: (i) the comfortable dorsiflexion angle (maximum angle with NRS pain score ≤2/10), and (ii) the maximum tolerable torque (just below muscle guarding or spastic catch). The target angle for haptic-proprioceptive feedback was set to ≥15° where possible. If the comfortable angle was below 15°, movement amplitude was limited to that threshold to prevent overstretching. Plantarflexion beyond 0° was prohibited to avoid spastic co-activation. Following successful BCI classification, the robot executed a single passive dorsiflexion movement from 0° to the target angle at 20°/s, returning immediately to neutral without holding. Cycle duration was (2 × target angle)/20°/s. Real-time torque monitoring enforced a pre-set session threshold (typically 8-12 Nm), with automatic termination if exceeded. This amplitude- and torque-adaptive approach ensures adequate proprioceptive stimulation—targeting a functional range (10-15°) when tolerable—while minimizing discomfort and involuntary activation in subacute patients with limited ankle mobility.
(1)
We implemented the Filter Bank Common Spatial Pattern (FBCSP) algorithm to discriminate between ankle dorsiflexion and fist-clenching motor imagery tasks. EEG signals were down-sampled from 1000 Hz to 250 Hz, then bandpass-filtered (8-30 Hz) using a Chebyshev type II filter and decomposed into 10 overlapping (50%) 4-Hz sub-bands. From each sub-band, we extracted 4 common spatial pattern features and performed feature selection using information entropy criteria. A linear support vector machine classifier was trained on the resulting feature set for task discrimination.
(2)
Ankle-Robot Training
The ankle robot (Beijing LTK Science and Technology Co., Ltd.) was secured to a stationary chair to prevent device displacement during operation. The participants were seated with the affected limb positioned at 30° knee flexion and neutral ankle alignment (0° dorsiflexion). The foot was firmly affixed to the motor-driven footplate using adjustable dorsal and heel straps, ensuring proper alignment of the ankle axis with the motor shaft. An integrated torque sensor recorded real-time ankle joint kinetics during the training sessions (Figure 1(E)). For the control group, robotic-based rehabilitation is passive and the ankle robot is driven by a servo motor controlled by a digital signal processor, as described in a previous study. 17
Outcome Measures
Biomechanical Evaluations
Evaluations included active dorsiflexion range of motion (DF-AROM) and dorsiflexor muscle strength (MS), quantified using a Hoggan MicroFET3 digital dynamometer (Hoggan Health Industries, Inc. Salt Lake City, UT, USA) 17 Spasticity of the triceps surae was evaluated using the Modified Ashworth Scale (MAS). 18 MAS scores range from 0 to 5 points, with higher scores indicating worse spasticity. Level 0 was set as 0, level I was set as 1, level I+ as 2, level II as 3, level III as 4, and level IV as 5.
Clinical Evaluations
Participants underwent comprehensive functional evaluations including: The Fugl-Meyer Assessment for Lower Extremity (FMA-LE; 0-34 points) to quantify sensorimotor impairment 19 ;Berg Balance Scale (BBS; 0-56 points) to evaluate postural control, 20 and Functional Ambulatory Categories (FAC; Holden0-Holden5) to characterize walking independence. 21
Electrophysiological Assessment
Five minutes of eyes-closed resting-state EEG data were recorded using a 64-channel system. Offline preprocessing was performed using the EEGLAB toolbox (version 2019.0) and MATLAB (R2022b) was conducted with custom functions. 22 The workflow comprised 5 steps. (1) Applying s zero-phase finite impulse response bandpass filter (1-45 Hz). (2) Down-sampling the data to 250 Hz. (3) Semi-automatically identifying and discarding bad channels and interpolating their signals using spherical interpolation. (4) Re-referencing the EEG data to the average across all channels and restoring the original reference channel (CPz) values. (5) Removing artifacts through independent component analysis.
Power spectral density (PSD) was computed using Welch’s method (2-second epochs, 50% overlap, Hamming window). For each channel, absolute band power was calculated through spectral integration within standard frequency bands (δ: 1-4 Hz, θ: 4-8 Hz, α: 8-13 Hz, β: 13-30 Hz). Relative power was derived by normalizing each bands’ power against the total integrated power (1-30 Hz). Global power metrics were obtained by averaging across all channels, yielding relative power of delta (rδ), theta (rθ), alpha (rα), and beta (rβ) bands.
These global measures were further utilized to compute 5 ratio-based features:





Then, the absolute PSD was employed to compute frequency-specific pairwise-derived Brain Symmetry Index (pdBSI) across 4 frequency band. For each frequency band, the pdBSI was calculated using the formula:

Here,
FC was assessed using the weighted phase-lag index (wPLI) with the sliding-window approach (window length of 2 seconds and 50% overlap). Preprocessed data were first transformed via scalp Laplacian filtering to mitigate volume conduction effects. Analytic signals were derived using complex Morlet wavelets (logarithmically spaced central frequencies: 2 to 30 Hz in 20 steps; cycles: 4-8). Connectivity strength between channels x and y for each window and each frequency was computed as:
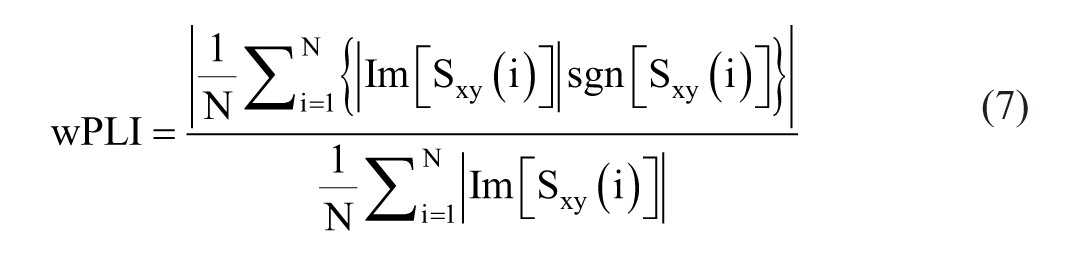
where
Statistical Analysis
Data normality was verified using the Shapiro-Wilk test. Between-group baseline comparisons employed independent t-tests (normal data) or Mann-Whitney U tests (non-normal data) for continuous variables, and Fisher’s exact tests for categorical variables. Within-group training effects were assessed using paired t-tests or Wilcoxon signed-rank tests for biomechanical (ROM, MS, and MAS) and clinical (FMA-LE, BBS, and FAC) outcomes. Effects were considered significant at P-values <.05. Between-group differences in intervention effects were evaluated using Mann-Whitney U tests, with a Bonferroni correction applied for multiple comparisons (P=.0083). The statistical analyses were performed using SPSS version 21.0 (IBM Corporation, Armonk, NY, USA). All EEG statistical analyses were performed using custom MATLAB scripts with the statistical significance threshold set at 0.05. Baseline variability was accounted for by implementing ANCOVA models with T1 outcomes as dependent variables, treatment group as the fixed factor, and T0 measurements as covariates. Between-group differences at T1 were evaluated using the 2-sample t-test.
Results
The Flow of the Trial and Baseline Characteristics of Subjects
Between August 2023 and October 2024, we screened consecutive inpatients from the rehabilitation department (n = 82) for eligibility. After excluding 31 patients who did not meet inclusion criteria and 11 who declined participation (Figure 2), we randomized 40 participants (1:1 allocation) to either the BCI group (n = 20) or ankle-robot group (n = 20) groups. Both groups experienced 4 dropouts, with no adverse events reported. Baseline demographic and clinical characteristics showed no significant intergroup differences (Table 1).
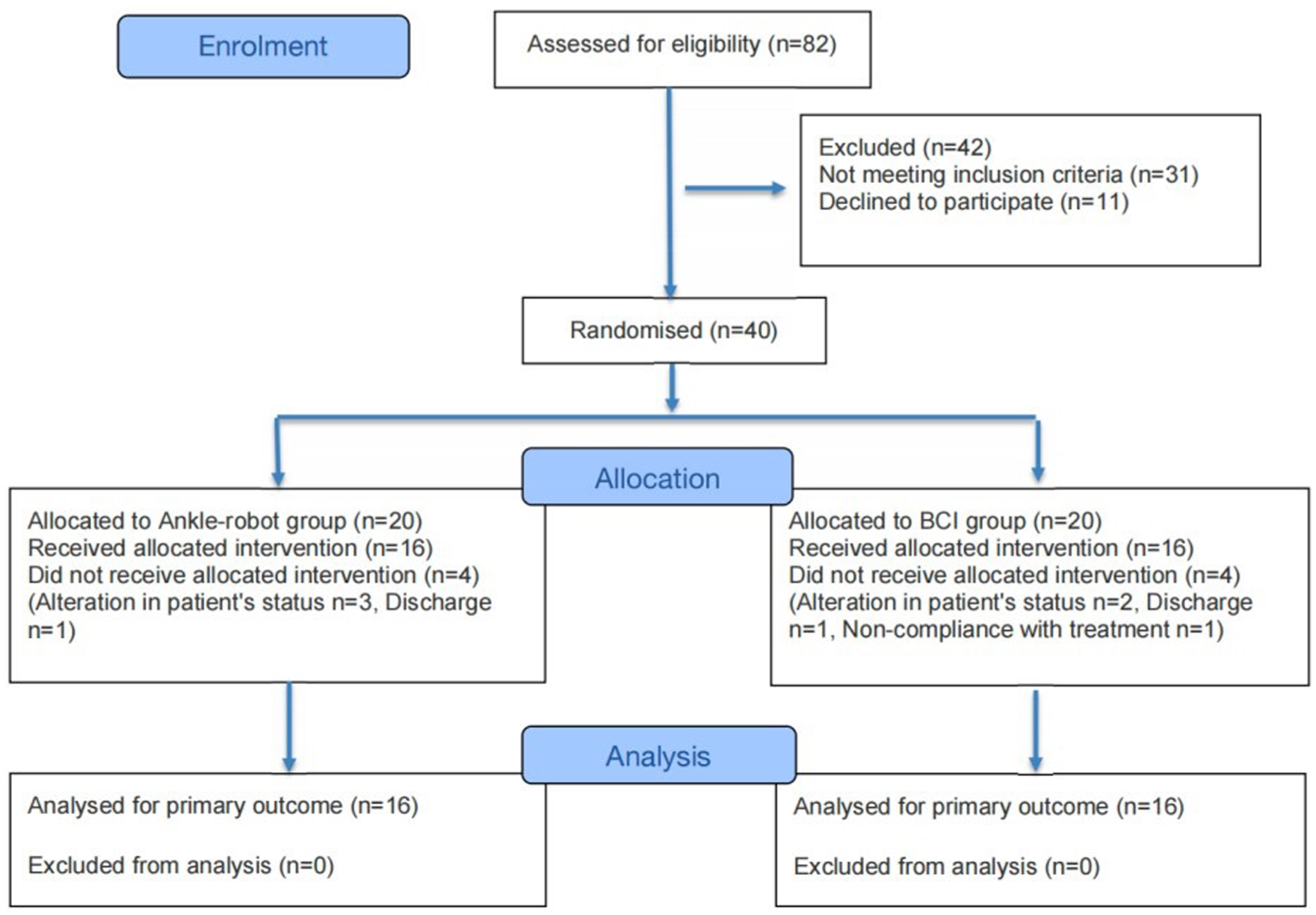
CONSORT patient flow throughout the study.
Baseline Characteristics of the Subjects.
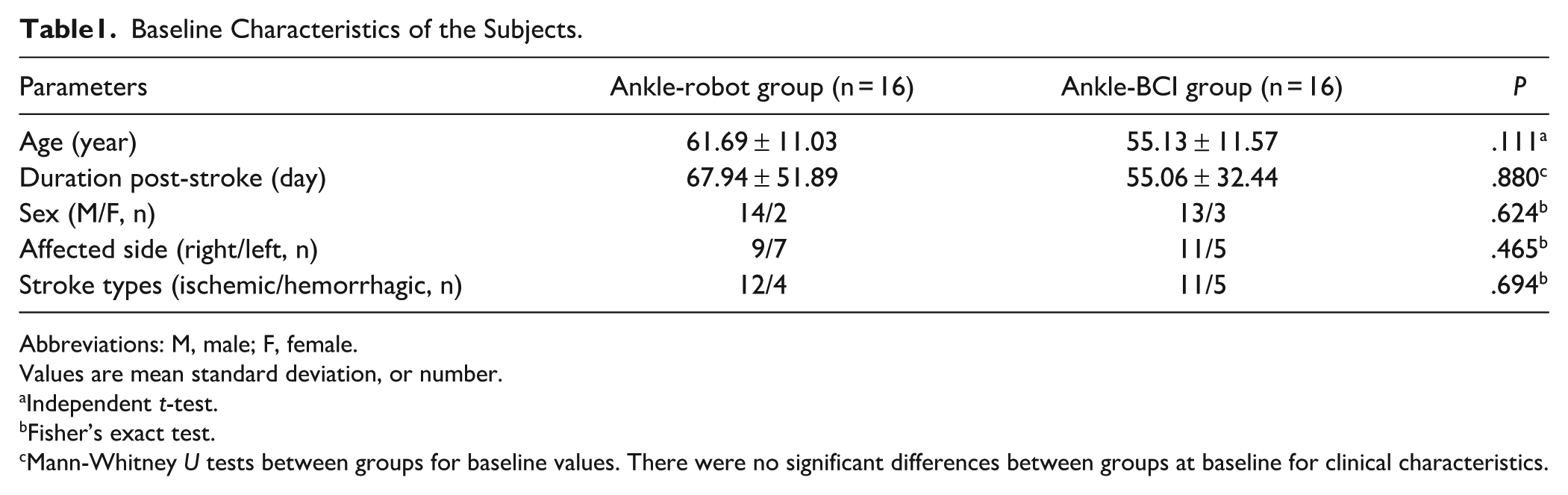
Abbreviations: M, male; F, female.
Values are mean standard deviation, or number.
Independent t-test.
Fisher’s exact test.
Mann-Whitney U tests between groups for baseline values. There were no significant differences between groups at baseline for clinical characteristics.
Biomechanical and Clinical Evaluations
No significant differences in baseline DF AROM, dorsiflexor muscle strength, MAS of the calf muscle, FMA-LE, BBS, or FAC were found between the 2 groups. Following the 2-week intervention, both groups demonstrated significant improvements in dorsiflexor strength (control: P = .003; BCI: P = .001), DF-AROM (control: P = .005; BCI: P = .003), FMA-LE (both P < .001), BBS (both P < .001), and FAC (control: P = .008; BCI: P = .003). Notably, only the experimental group exhibited reduced calf muscle spasticity (MAS: P = .038 vs. control P = 0.317). Between-group comparisons revealed superior FMA-LE gains in the experimental group (∆FMA-LE, P = .007) (Table 2).
Biomechanical and Clinical Evaluations at Pre- and Post-Training Between 2 Groups.
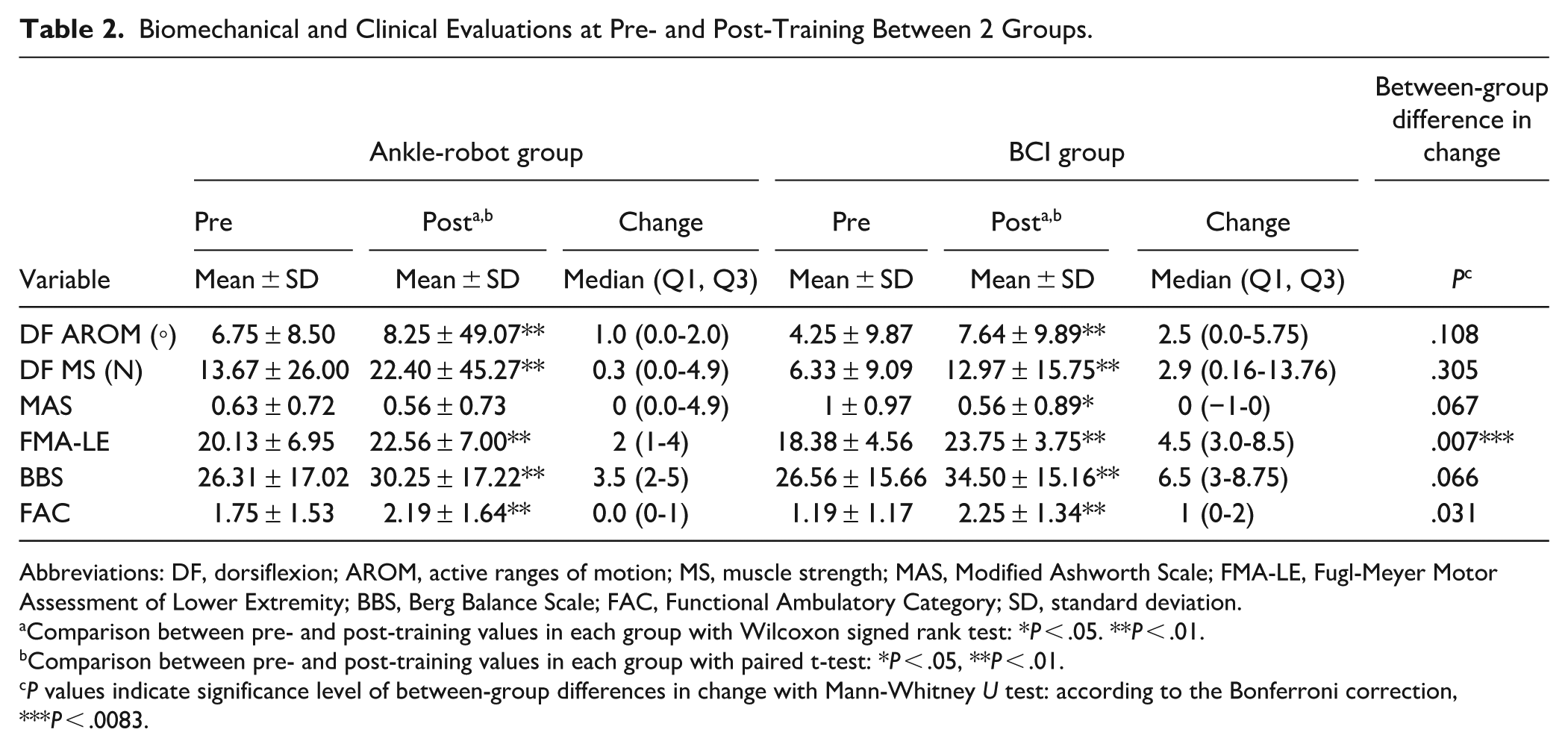
Abbreviations: DF, dorsiflexion; AROM, active ranges of motion; MS, muscle strength; MAS, Modified Ashworth Scale; FMA-LE, Fugl-Meyer Motor Assessment of Lower Extremity; BBS, Berg Balance Scale; FAC, Functional Ambulatory Category; SD, standard deviation.
Comparison between pre- and post-training values in each group with Wilcoxon signed rank test: *P < .05. **P < .01.
Comparison between pre- and post-training values in each group with paired t-test: *P < .05, **P < .01.
P values indicate significance level of between-group differences in change with Mann-Whitney U test: according to the Bonferroni correction, ***P < .0083.
EEG Analysis
Analysis of covariance (ANCOVA), controlling for baseline (T0) values, revealed distinct between-group differences in neural features at T1. The BCI group exhibited 4 electrophysiological phenomena compared to the ankle-robot group: (1) significantly reduced delta power (rδ: t = −3.038, P = .005) and enhanced alpha power (rα: t = 2.532, P = .017); (2) lower spectral power ratios across all indices, with significant reductions observed in DAR (t = −2.669, P = .012) and DTABR (t = −2.381, P = .024); (3) reduced δ-band interhemispheric asymmetry (pdBSIδ: t = −2.503, P = .018); and (4) preferential enhancement of Cz-parietal connections in the BCI group in wPLI-based connectivity analysis (Table 3, Figures 3).
Analysis of EEG Spectral Features.
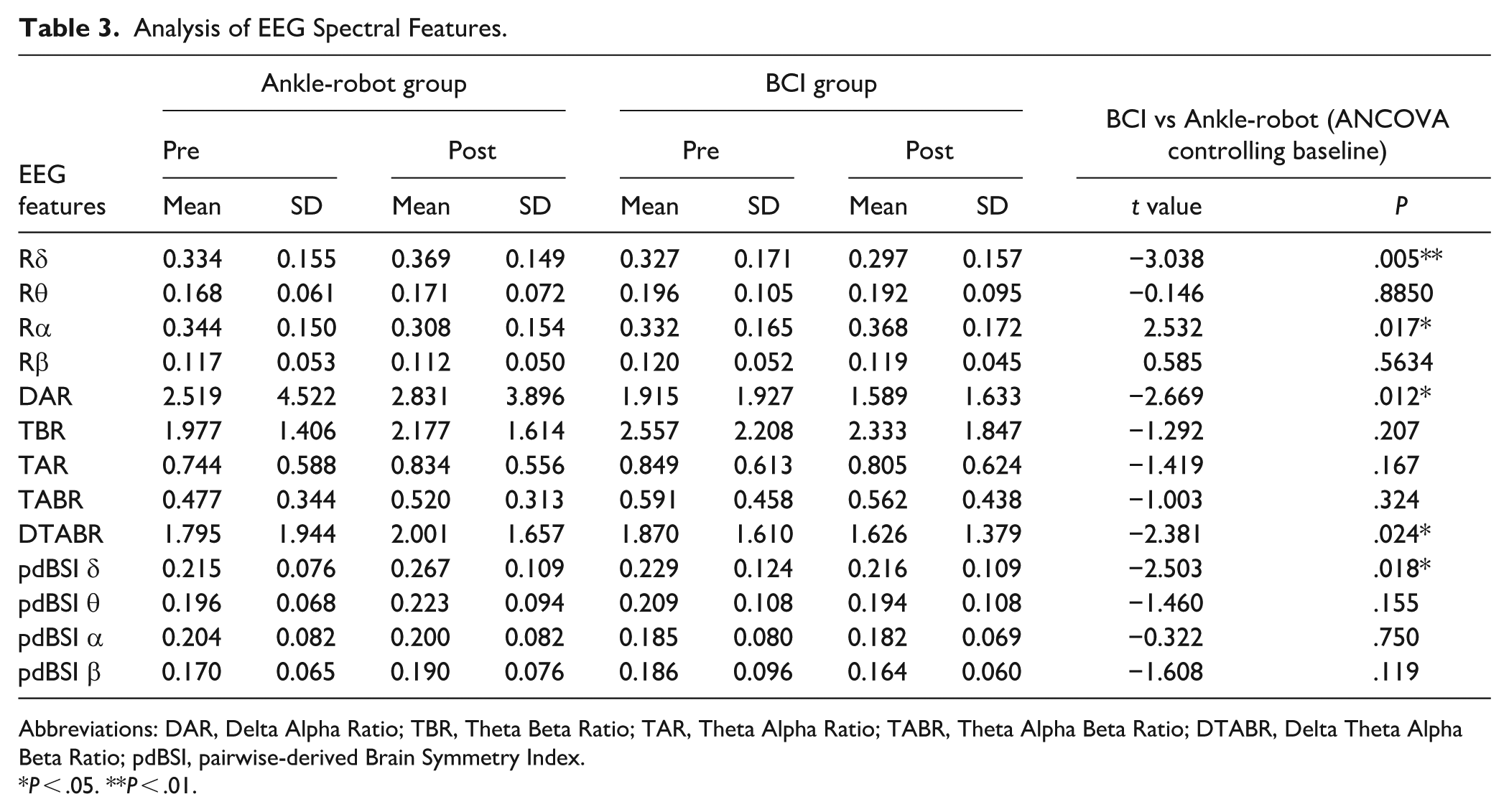
Abbreviations: DAR, Delta Alpha Ratio; TBR, Theta Beta Ratio; TAR, Theta Alpha Ratio; TABR, Theta Alpha Beta Ratio; DTABR, Delta Theta Alpha Beta Ratio; pdBSI, pairwise-derived Brain Symmetry Index.
P < .05. **P < .01.
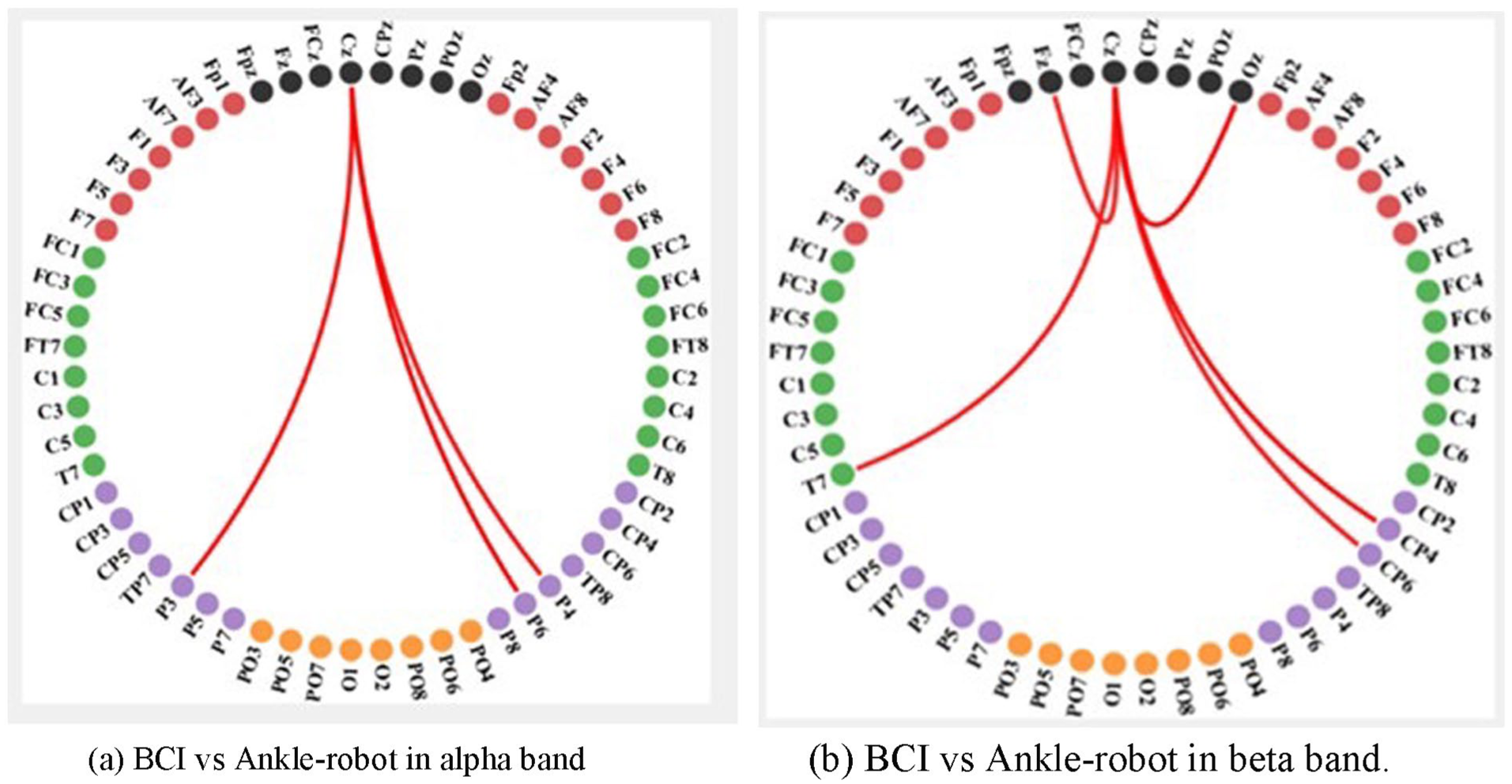
Group differences in functional connectivity (FC). For X versus Y, the blue color indicates X < Y; the red color indicates X > Y. (A) BCI versus Ankle-robot in alpha band. (B) BCI versus Ankle-robot in beta band.
Discussion
The RCT showed significant within-group improvements in lower limb motor function, balance function, and walking ability after 10-session training in both groups. However, the BCI group showed additional improvements in MAS. Between-group comparisons showed significant differences in ∆FMA-LE. These results demonstrated that BCI training exhibited superior efficacy in enhancing lower limb motor function compared to ankle-robot training and alleviating lower limb spasticity. The qEEG results showed that the BCI group exhibited reduced low-frequency power, elevated high-frequency power, reduced inter-hemispheric brain asymmetry, and restored connectivity compared with the ankle-robot group, similar to EEG profiles observed in healthy individuals.22 -24 This indicates that BCI intervention drives EEG features toward normative profiles observed in healthy individuals, surpassing the limited neuromodulatory effects of ankle-robot training. Motor imagery-based BCI ankle robot training establishes a closed-loop system that utilizes real-time neural signals to provide active robotic assistance. Unlike conventional repetitive passive movement training, which primarily enhances motor function through mechanical stretching, this intent-driven approach promotes neural recovery and functional improvement beyond the effects of passive robot-assisted therapy.
Motor imagery has emerged as a promising neurorehabilitation approach, leveraging shared neural substrates between imagined and executed movements to promote post-stroke recovery. 25 While conventional motor imagery training has shown limited clinical efficacy in some trials, likely due to interindividual variability in corticomotor activation, 26 BCI-mediated motor imagery paradigms address this limitation through closed-loop systems that: (1) detect movement intention via EEG signatures (event-related desynchronization/event-related synchronization and movement-related cortical potentials), 27 (2) provide real-time sensory feedback, and (3) trigger assistive devices. This approach is particularly relevant for severely impaired patients who retain preserved motor imagery capacity despite minimal voluntary movement. 28
Common BCI strategies, including Functional Electric Stimulation (FES) and robotic assistance, have been applied to stroke neurorehabilitation systems. The 2 therapies differ in rehabilitation mechanisms: BCI-FES affects the brain by “stimulating” muscle movement, while BCI-robot training does so by “assisting” movement. Yet both ultimately promote neuroplasticity through bidirectional interaction.6,29,30 Users control BCI-FES via brainwaves to generate intended movements while enhancing neural plasticity. Mrachacz-Kersting et al 5 demonstrated that MRCP-triggered electrical muscle stimulation could effectively bridge the disrupted sensorimotor loop in stroke patients. Subsequently, studies by Do et al 31 established the safety and feasibility of foot-drop targeted BCI-FES systems, while Chung et al 10 reported superior gait and balance outcomes compared to conventional FES. These clinical benefits may arise from Hebbian plasticity mechanisms 32 and enhanced afferent feedback during combined BCI-FES therapy. BCI-FES directly reconstructs motor pathways through electrical stimulation but is limited to patients with mild-to-moderate impairment, as it cannot restore movement in complete paralysis. Its efficacy is further constrained by imprecise parameter control and the superficial nature of surface-electrode FES. 33 Conversely, BCI-Robotics systems use robotic hardware to assist intended movements, enhancing motor learning. A key advantage is their applicability even in cases of no residual motor function, enabling movement of paralyzed limbs. 34 While these systems show promise in stroke rehabilitation, research has predominantly focused on the upper limb, with lower-limb applications remaining less explored. Notably, Xu et al 35 showed that MRCP-triggered ankle orthoses with multimodal feedback significantly improved lower limb function in subacute stroke patients compared to those who received conventional training. In our study, during ankle motor imagery-based BCI training, patients imagine performing ankle dorsiflexion as if kicking a ball. The system performs real-time analysis of EEG signals and, upon reaching a predefined threshold, triggers an ankle-stretching robot to execute the movement. Concurrent visual, auditory, and proprioceptive feedback is provided, closing a “sensory-motor loop” that facilitates functional reorganization of impaired central neural circuits and peripheral effectors.11,36 This study demonstrates that BCI ankle robot training leads to greater improvement in active lower limb motor function in hemiplegic patients compared to robotic ankle stretching alone, likely due to its enhanced efficacy in promoting neural functional remodeling. However, a key challenge in BCI-based robotic systems lies in achieving real-time and high-precision control of robotic movements, which necessitates ongoing refinement in future research.
Post-stroke recovery fundamentally relies on neuroplastic reorganization, 36 with Hebbian plasticity representing a key mechanism. 5 BCI systems capitalize on this principle by closing the disrupted sensorimotor loop through multimodal feedback (robotic/haptic/proprioceptive) contingent on successful motor imagery detection.36,37 While visual feedback remains prevalent in MI-BCI paradigms, 38 emerging evidence suggests that haptic stimulation may enhance engagement and task performance, 39 although without eliciting distinct neurophysiological patterns. Crucially, proprioceptive feedback, whether through peripheral nerve stimulation 40 or robotic limb movement, appears particularly effective by providing naturalistic somatic input that reinforces motor representations.41,42 Therefore, our protocol integrated multiple feedback modalities (visual, auditory, haptic, and proprioceptive) to optimally engage these plasticity mechanisms, building on established correlations between feedback accuracy and functional outcomes6,43 -45 while addressing ongoing questions regarding optimal feedback design. 36 Thus, this study adopted multiple feedback modalities, such as vision, hearing, haptic stimulation, and somatosensory.
Resting-state EEG spectral features, particularly the delta/alpha ratio (DAR) and pdBSI have emerged as robust biomarkers for monitoring stroke progression and predicting motor outcomes.46,47 Elevated DAR values, reflecting increased delta/theta and diminished alpha power, indicate cerebral dysfunction, while pdBSI quantified interhemispheric spectral power asymmetries that correlated with motor impairment severity (r = −0.62, P = .044). 48 Notably, lower baseline pdBSI values predict better functional recovery across subacute and chronic stages,12,23,49 a finding corroborated by our results showing BCI-induced pdBSI-δ reductions superior to those of robotic training alone. FC patterns further enhanced prognostic capability. Increased μ/β-band intrahemispheric FC within ipsilesional motor areas50,51 and enhanced interhemispheric FC during movement 52 were found to correlate with subsequent motor improvement. Specifically, FC measured at 4 weeks post-intervention significantly predicts 8-week lower limb functional recovery (FMA-LE), 52 suggesting that these neurophysiological markers may guide rehabilitation strategies. Post-intervention connectivity analyses revealed distinct frequency-dependent reorganization patterns between interventions. In our study, the BCI group exhibited significantly enhanced α-band connectivity in Cz-P3/P4/CP6 pathways (P < .05), suggesting improved sensorimotor integration and interference suppression. More notably, BCI training-induced widespread β-band network engagement (Cz-Fz/Oz/T3/CP4/CP6; P < .01), reflecting the superior integration of motor execution with cognitive-visual processing compared to the localized connectivity changes observed following robotic training. These differential neuroplastic changes demonstrate the unique capacity of BCI to promote functionally relevant, distributed cortical reorganization through active neuromodulation, providing a neurophysiological rationale for its superior therapeutic effects in stroke rehabilitation. This study suggests that BCI training provides a neurophysiological basis for stroke rehabilitation by reducing slow-wave power and asymmetry, increasing alpha power, and promoting widespread reorganization of α- and β-band networks in the brain. However, the current findings have limitations and do not fully explain the neural mechanisms of ankle BCI rehabilitation. Future research should integrate higher-resolution imaging, kinematic, and electrophysiological data to precisely pinpoint the specific neural pathways activated by BCI, and conduct long-term follow-up to investigate the durability of these neuroplastic changes and their actual impact on ankle function.
Limitations
This study has several limitations. First, the modest sample size reduced statistical power for between-group comparisons beyond the primary outcome (FMA-LE), potentially obscuring subtler effects detectable in larger cohorts. Future studies involving more subjects may reveal additional group differences and enhance the study’s power. Second, the brief 2-week intervention period and absence of long-term follow-up preclude conclusions regarding the sustainability of functional gains or neuroplastic reorganization; extended treatment and longitudinal assessments are needed to evaluate durability. Third, reliance on the Modified Ashworth Scale introduces rater-dependent subjectivity for spasticity; future work should integrate objective neurophysiological measures (e.g., H-reflex modulation via surface EMG). Fourth, a key limitation is the lack of an active control group, since robot training alone did not match the BCI group’s cognitive load; future work should use an active control with sham BCI feedback to account for placebo effects and cognitive engagement differences. Fifth, a significant limitation of this study is the gender bias in the sample, which may restrict the generalizability of the findings. Although this is partly due to the higher incidence of stroke in males, future studies should enroll gender-balanced samples and conduct subgroup analyses to investigate the impact of gender differences on rehabilitation outcomes. Furthermore, while the Functional Ambulatory Category efficiently classifies walking independence, its insensitivity to kinematic gait parameters limits mechanistic insight; instrumented motion analysis is warranted to elucidate recovery patterns. Additionally, despite resting-state qEEG’s millisecond temporal resolution, susceptibility to volume conduction constrains spatial precision; multimodal imaging (e.g., fMRI) is required to anatomically localize connectivity alterations. Finally, generalizability may be constrained by single-center recruitment and device-specific implementation, necessitating validation through multisite trials with diverse populations.
Conclusions
This RCT provides evidence that BCI-controlled ankle robot training confers superior therapeutic post-stroke motor recovery benefits relative to conventional ankle-robot training. The intervention yielded significant improvements in lower-extremity function (FMA-LE) and spasticity reduction (MAS), supported by neurophysiological evidence of reduced slow-wave power and asymmetry, increased α-band brain activity and corticomotor functional connectivity. The findings demonstrate that closed-loop BCI systems promote functionally relevant neuroplasticity, establishing their clinical value as a targeted rehabilitation strategy for stroke-related motor impairment.
Footnotes
Acknowledgements
The authors express their sincere appreciation to the participating therapist and participants for their cooperation.
Author Contributions
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Key R&D Program of China (grant No. 2022YFC3601105), Young Investigator Grant of Beijing Tsinghua Chang Gung Hospital (23329-0-02), Open Research Project Program of Beijing Municipal Key Laboratory of Opto-Mechatronic Equipment Technology (BIPT-OMET-2022-02). No additional external funding was received for this study. The funders had no role in study design, data collection, and analysis, decision to publish, or preparation of the manuscript.