
Abstract
Background:
Spinal cord injury (SCI) leads to lifelong disability with highly variable neurological recovery, complicating prognostication and conceptualization of clinical trials. The American Spinal Injury Association Impairment Scale (AIS) is widely used to classify injury severity. Although AIS A injuries are considered sensorimotor complete, they show substantial heterogeneity in residual function and recovery. Data-driven approaches offer an opportunity to uncover latent subgroups beyond conventional classifications. We evaluate whether unsupervised, data-driven clustering can identify distinct subgroups within patients with traumatic SCI and characterize neurological patterns in sensorimotor complete SCI.
Methods:
We applied an unsupervised clustering model to International Standards of Neurological Classification of Spinal Cord Injury (ISNCSCI) examination scores from the European Multicenter Study about Spinal Cord Injury dataset (3165 patients), to derive neurological groupings independent of predefined ISNCSCI classifications. Clusters were derived from the full cohort, followed by focused analyses of individuals classified as AIS A at their first documented assessment. External reproducibility was evaluated using data from the Sygen clinical trial.
Results:
Six distinct clusters were identified. Patients graded as AIS A were represented in 5 clusters, which differed markedly in injury level (paraplegic vs tetraplegic) and indicators of recovery potential, including neurological sparing, upper and lower extremity motor scores, and AIS conversion rates. These patterns were consistently reproduced in the Sygen cohort.
Conclusions:
Proposed framework complements conventional AIS grading by revealing distinct neurological conditions related to the variability among patients with baseline sensorimotor complete injuries. Proposed data-driven framework enables more comprehensive prognostic assessments and improves patient stratification in clinical trials.
Keywords
Introduction
Spinal cord injury (SCI) is a rare but devastating neurological condition with lifelong consequences for affected individuals. Despite promising evidence from precisely defined preclinical models and numerous clinical trials over the past decades,1-9 translation into clinical benefit has been difficult. Demonstrating consistent and clinically meaningful effects of pharmacological interventions on tissue preservation or functional recovery after acute SCI remains challenging due to intrinsic heterogeneity in neurological status and recovery trajectories.10-14 Patients with seemingly similar injuries can experience vastly different sensory and motor outcomes: some recover extensively in the first weeks to months, while others improve minimally. This variability complicates prognostication, leaving patients with uncertainty about their future, and poses major challenges for clinical trials, where treatment effects must be measured against highly variable spontaneous recovery.
Patient stratification is key to reduce outcome variability and improve both prognostic accuracy and clinical trial design.10,15,16 By grouping patients according to baseline severity, expected recovery patterns, or likelihood of responding to interventions, stratification supports more accurate prognostication, guides individualized rehabilitation, and improves the design and interpretation of clinical studies.17-19 In current practice, the American Spinal Injury Association (ASIA) Impairment Scale (AIS; grades A-E, plus NT) 20 is used to classify the severity of neurological impairment and provides a standardized and clinically interpretable framework that is indispensable in SCI care and research. However, this categorical system may oversimplify complex neurological variation.
A particularly challenging category is represented by AIS grade A, commonly referred to as sensorimotor complete SCI, defined by the absence of sacral sparing (ie, no sensory and motor function in the lowest sacral segments, S4 and S5). 21 This grade was initially defined based on the preservation of sensorimotor functions in less than 4 segments below the neurological level of injury (NLI). However, it was found that fewer individuals with traumatic SCI convert between complete and incomplete status when the absence of sacral sparing was used instead of the length of the zone of partial preservation to define a complete injury (AIS A). 22 Because a complete injury is based solely on the absence of function in the lowest sacral segments, the AIS A category includes patients with substantial but unrecognized variability in residual sensorimotor function below the NLI, reflecting limitations in the granularity of current AIS-based clinical classification.10,21,23 The minority of individuals initially graded AIS A later transition to incomplete status due to recovery of sensorimotor functions in the lowest sacral segments, while the majority remains complete, sometimes despite substantial recovery of motor and/or sensory functions below the NLI.21,24-26 The timing, extent, and functional significance of these changes differ widely, indicating marked heterogeneity within the AIS A group.10,24,27,28
These challenges underscore the need to complement existing grading systems with additional insights into heterogeneity of individuals with SCI. Data-driven clustering models capable of modeling complex, nonlinear relationships and uncovering latent strata offer a potential solution. Such methods, applied to International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) assessments, 20 can identify groups of patients who share similar patterns across motor, sensory, and sacral functions—patterns that may not be visible within the broad categories of AIS grade or NLI. In this way, clustering can offer complementary insights beyond AIS grade into patient heterogeneity and support a more detailed characterization of neurological status and subsequent recovery.
Here, we apply a state-of-the-art deep probabilistic clustering model to ISNCSCI assessments from individuals with traumatic SCI. We hypothesize that distinct subgroups exist within the population of individuals with sensorimotor complete SCI (AIS A grade) and that these subgroups exhibit different neurological recovery potential. By revealing this hidden diversity, the proposed framework offers a new perspective on sensorimotor completeness and has the potential to improve prognostic modeling, support individualized clinical decision-making, and enhance stratification in future SCI trials.
Methods
Workflow
The proposed framework consists of 2 main steps: (1) unsupervised clustering of the full data set to identify groups with similar characteristics, and (2) analysis of the clusters based on predefined clinical criteria. The general workflow is shown in Figure 1. The clustering is performed once and can subsequently be reused for various analyses within the identified clusters. In the present study, the analysis focuses on individuals classified as AIS A at the first documented assessment, with the goal of uncovering distinct subgroups that may provide new insights for both clinical interpretation and trial design. Figure 1 summarizes the proposed approach.
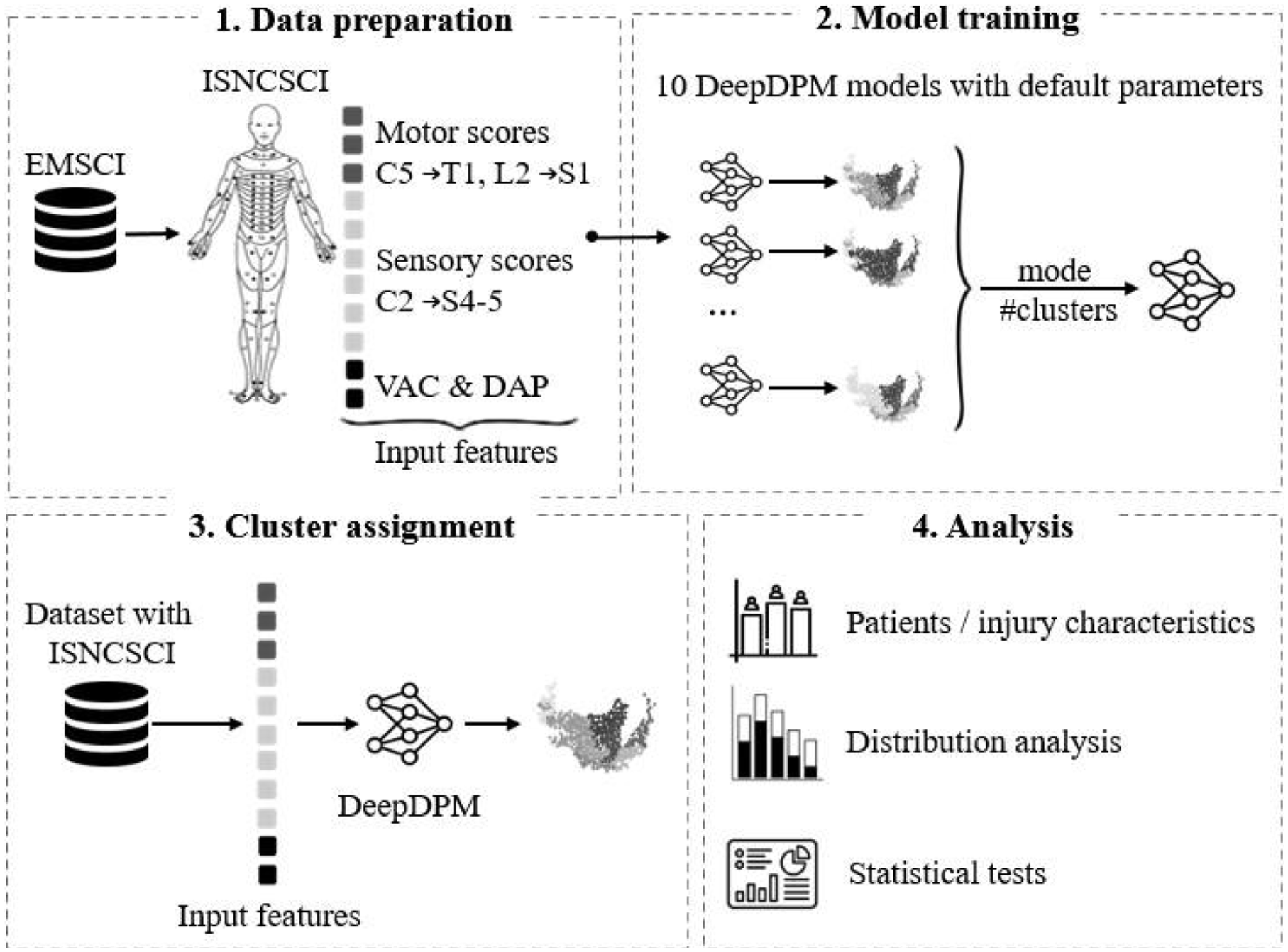
Workflow for unsupervised patient stratification using ISNCSCI features from the EMSCI dataset. 1. Data preparation: All documented ISNCSCI assessments, including motor (C5–T1 and L2–S1), sensory (C2–S4/S5), and sacral function (VAC and DAP) scores, were selected and standardized to form the feature set. 2. Model training: A probabilistic deep clustering approach (DeepDPM) was used to learn patient representations and identify cluster structure without predefined labels. Ten independent models were trained, and the mode number of clusters was selected to ensure stability. 3. Cluster assignment: The trained model was applied to EMSCI and Sygen ISNCSCI datasets to assign each assessment to a cluster. 4. Results analysis: cluster profiles were evaluated for clinical interpretability through comparisons of demographic, and neurological characteristics.
Patient Cohorts
The study is based on data from the European Multicenter Study about Spinal Cord Injury (EMSCI; ClinicalTrials.gov Identifier: NCT01571531), collected between 2002 and 2023 across 33 centers in accordance with the Declaration of Helsinki. From the full EMSCI database of 6607 patients with acute traumatic and ischemic SCI, only those with traumatic injuries were included here. Two cohorts were defined: a clustering cohort and an analysis cohort.
The clustering cohort included patients with documented AIS grade, NLI, and complete Spinal Cord Independence Measure (SCIM) III assessments. 29 Patients were excluded if they showed neurological deterioration (any motor score deterioration by 2 or more points between consecutive assessments), as individuals with traumatic SCI typically exhibit stable or improving neurological function over time, while marked deterioration is more likely related to complications. These are not captured in the EMSCI dataset and therefore their effects cannot be accounted for in the analysis. Patients were also excluded if they had a total motor score of 100 or an AIS E grade at the first assessment, or had injuries located caudal to S1 at the initial assessment. More details are provided in Figure S1 in Supplemental Materials.
The analysis cohort was drawn from the clustering cohort and included patients classified as AIS A at their first documented assessment with completed ISNCSCI evaluations during baseline (16-40 days post-injury [EMSCI acute I stage]) and follow-up (150-186 days post-injury [EMSCI acute III stage]) time points. More details are provided in Figure S1 in Supplemental Materials.
Clustering
Clustering was performed on the clustering cohort based on ISNCSCI examinations, consisting of segmental motor scores (MS, ordinal [0-5]), light touch sensory score (LTSS, ordinal [0-2]) and pin prick sensory score (PPSS, ordinal [0-2]), voluntary anal contraction (VAC, binary [Present/Absent]), and deep anal pressure (DAP, binary [Present/Absent]). No ISNCSCI classification variables, such as AIS grade or NLI, or functional scores (eg, SCIM III) were included, allowing analysis of how the data-driven clusters align with clinical classifications. Details on preprocessing and handling of missing data are provided in Section 1.2 in Supplemental Materials.
To identify subgroups without relying on prior assumptions about the number of subgroups or labels typical of supervised approaches, we applied an unsupervised Deep Dirichlet Process Mixture (DeepDPM) model. 30 This probabilistic deep clustering approach detects latent structure in the data without imposing predefined clinical labels. As a result, the model identifies potential subgroups based on similarities and differences in motor and sensory profiles across individual ISNCSCI assessments, including both differences between individuals and differences across assessments from the same individual. Importantly, all assessments are treated independently during clustering, such that recovery trajectories are not explicitly modeled. All technical details are provided in Section 1.3 in Supplemental Materials. After model training, the fitted DeepDPM model was applied to all ISNCSCI assessments to automatically assign each assessment to one of the identified clusters, providing a consistent basis for subsequent analyses.
Characterization
Two types of analyses were performed: (1) exploration of clusters (on the clustering cohort) and (2) targeted AIS A analysis (the analysis cohort).
For the visual presentation of the clustering manifold we employed the Uniform Manifold Approximation and Projection (UMAP) 31 technique. For exploratory cluster-wise analysis, categorical variables such as sex, AIS grade, and NLI were assessed using the Chi-square test. 32 Continuous and ordinal variables, including sum motor and sensory scores, which are not normally distributed, were compared using the Wilcoxon rank-sum test32,33 and the Kolmogorov–Smirnov test. 34
For the AIS A targeted analysis, we examined baseline (16-40 days post-injury) ISNCSCI assessments of individuals in each cluster, including AIS grade, NLI, motor (upper extremity motor scores [UEMS] and lower extremity motor scores [LEMS]) and sensory scores (PPSS and LTSS), and zones of partial preservation (ZPP). 20 The outcomes at follow-up (150-186 days post-injury) were also considered, including changes in motor and sensory scores, SCIM III subscores (total self-care [items 1-5], total respiration and sphincter management [items 6-9], total mobility [items 10-17]), AIS grade conversion, and transitions between clusters.
External Validation
External validation was conducted using the Sygen dataset. 1 While the Sygen study employed an earlier ISNCSCI version, the segmental motor and sensory scores used for clustering are consistently defined across versions. The Sygen inclusion cohort was defined using the same inclusion criteria as for the EMSCI clustering cohort, with the exception that SCIM III assessments were not available in the Sygen dataset (details provided in Figure S7 in Supplemental Materials). For the Sygen analysis cohort, we selected ISNCSCI assessments at the same baseline time window (16-40 days post-injury), while the follow-up was adapted to the Sygen assessment schedule and defined as 165 to 210 days post-injury, corresponding closest to the week 26 evaluation used in EMSCI.
All assessments from the Sygen inclusion cohort were inferred through the previously trained clustering model, developed on the EMSCI data. No retraining or fine-tuning was performed, ensuring an independent validation of the model’s generalizability. Subsequently, the targeted AIS A analysis was repeated in the Sygen analysis cohort following the same analytical pipeline as used for the EMSCI data. This allowed a direct comparison of subgroup characteristics and outcome trends across independent datasets.
Results
Clustering Cohort
The full ISNCSCI assessment manifold shown in Figure 2(A) illustrates the distribution of all observed neurological assessment states in the EMSCI clustering cohort, with each point representing a single assessment independent of patient identity or assessment time. By focusing on assessment states rather than individual patient trajectories, this representation highlights recurring neurological profiles that may occur across different patients and at different stages post-injury, enabling the identification of common neurological patterns within the cohort. The continuous structure of the manifold reflects the range of neurological profiles captured by motor, sensory, and sacral function measures and provides a global view of the assessment space on which subsequent cluster assignments are defined. Figure 2(B) illustrates the distribution of AIS grades (A-D) across the clustering cohort.
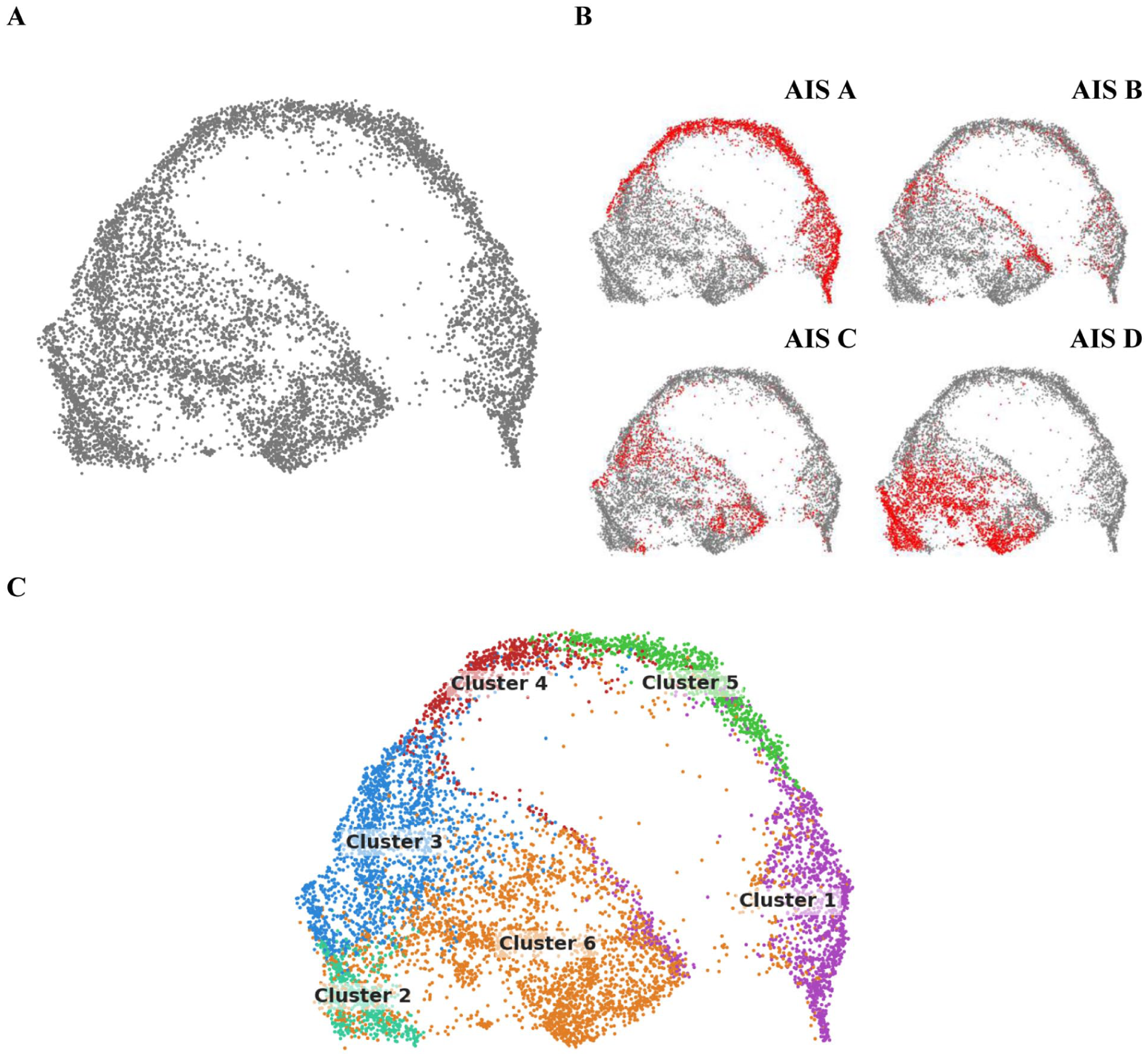
(A) Two-dimensional UMAP of all observed ISNCSCI assessments in the EMSCI clustering cohort. The visualization represents the space of observed neurological assessment states, independent of patient identity or assessment time, emphasizing that similar neurological profiles may occur in different patients and at different stages post-injury, and allowing the identification of common neurological patterns shared across patients rather than individual recovery trajectories. (B) Distribution of AIS grade assessments across the assessment manifold. In each panel, assessments corresponding to the indicated AIS grade (A-D) are highlighted in red, while all remaining assessments are shown in grey, illustrating how different AIS grades occupy overlapping but distinct regions of the neurological assessment space. (C) Cluster assignments across the ISNCSCI assessment manifold. Each point represents a single ISNCSCI assessment and is colored according to its assigned cluster, illustrating the spatial organization and overlap of data-driven neurological patterns. The distribution of motor and sensory scores across the EMSCI clustering manifold is shown in Figure S3 in the Supplemental Results.
The DeepDPM unsupervised clustering identified 6 distinct clusters, labeled 1 through 6, as visualized in the 2-dimensional UMAP space in Figure 2(C). The clusters represent data-driven partitions of the ISNCSCI assessment space, without implying predefined or clinically established categories. Most (88%) AIS A assessments are concentrated in the adjacent clusters 5, 1, and 4, with additional cases distributed across cluster 3 and a small number in cluster 6 (see Supplemental Table S1. Cluster 2 contains no AIS A cases. Notably, clusters 1, 4, and 5 also include a proportion of non-AIS A assessments (shown in gray in Figure 2(B)), indicating that these clusters encompass a mix of AIS grade representations. A detailed summary of cluster characteristics, including sample composition and key clinical features, is provided in Table S1 of the Supplemental Results.
Differences in the distribution of AIS grades and NLI across clusters of the EMSCI clustering cohort are shown in Supplemental Figures S4.AIS and S4.NLI. Patients in clusters 1, 2, and 6 have predominantly cervical NLIs but differ in severity, with cluster 1 enriched with patients with AIS grades A or B, cluster 2 largely composed of AIS D, and cluster 6 showing a mixed AIS C or D profile. Patients assigned to cluster 5 have almost exclusively thoracic NLIs with predominantly AIS A grade. Clusters 3 and 4 show a caudal shift toward lower thoracic–upper lumbar NLIs, with all AIS grades present in cluster 3 and mainly AIS grades A or B in cluster 4.
Clusters 2 and 6 include older individuals (mean age: ~53-55 years) compared with the remaining clusters (mean age: ~41-43 years), in line with previously reported associations between age and injury characteristics. 35 Motor scores further distinguish clusters: clusters 1, 4, and 5 show near-zero LEMS, cluster 2 shows higher LEMS (35-50), and clusters 3 and 6 span a broad LEMS range (0-50). UEMS analysis confirms the results of the NLI analysis of the presence of paraplegia in clusters 3 to 5 (UEMS = 50), heterogeneous impairment in clusters 1 and 6, and mostly preserved upper extremity function in cluster 2.
Taken together, these results indicate that individual clusters are characterized by distinct patterns of motor, sensory, and injury-level features, while partially overlapping in their distributions of AIS grade and NLI. Additional results from the exploratory cluster-wise analyses, are provided in detail in Figures S3 to S6 in Supplemental Results.
Analysis Cohort
The characteristics of the analysis cohort, along with the corresponding cluster assignments at baseline (16-40 days post-injury) are summarized in Table 1. Cluster 2 was excluded from further analyses, as no individuals from the analysis cohort were assigned to this cluster.
Characteristics of the EMSCI Analysis Cohort and the Derived Clusters at Baseline After Injury (16-40 Days Post-Injury).
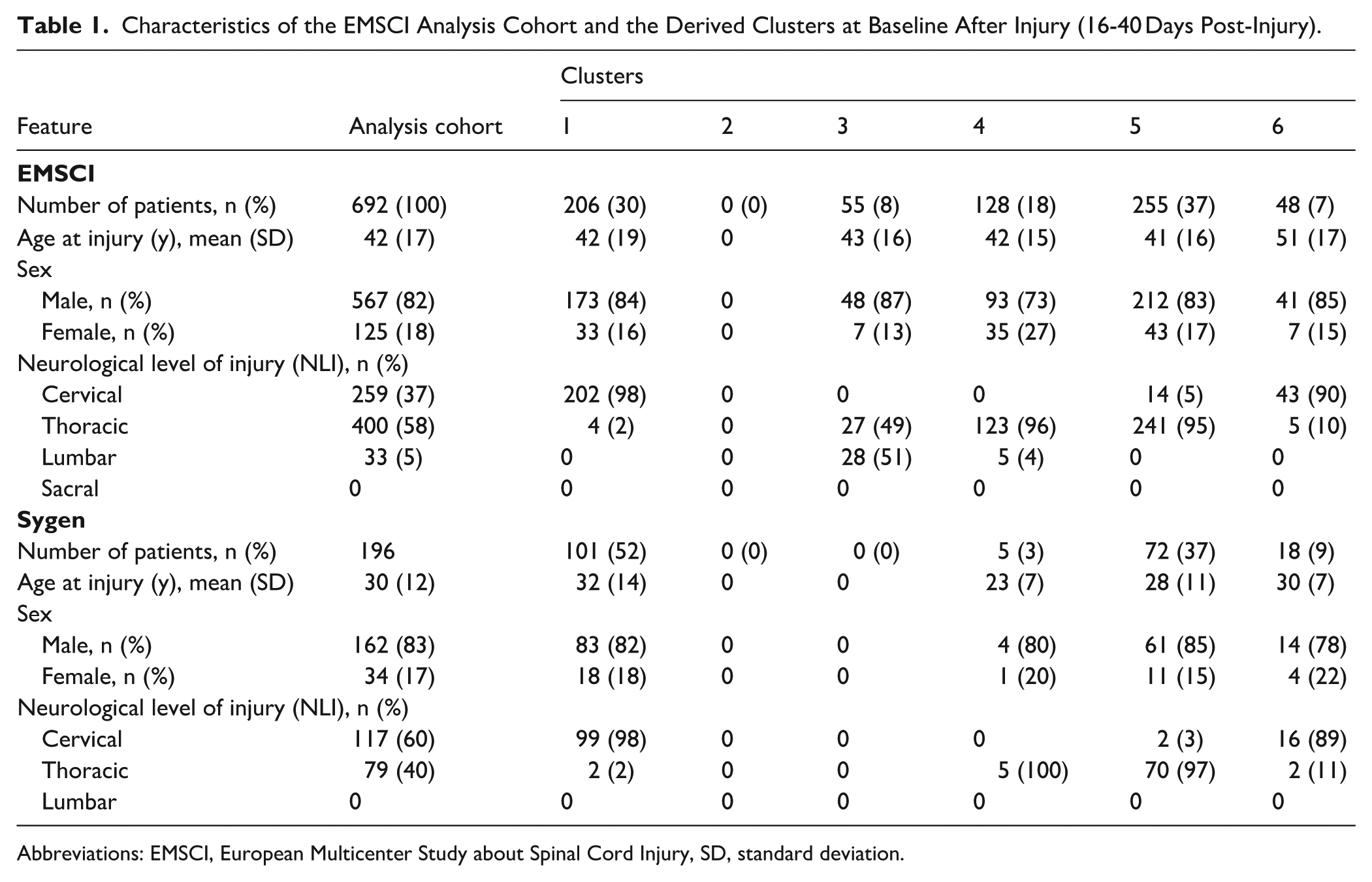
Abbreviations: EMSCI, European Multicenter Study about Spinal Cord Injury, SD, standard deviation.
The baseline distribution of AIS grades and NLI across the clusters of interest (1, 3, 4, 5, and 6) is summarized in Figures 3(A) and (B). AIS patterns suggest that clusters 3 and 6 include individuals who were classified as AIS A at a very early time (0-15 days ) post-injury but had converted to AIS B, C, or D by the baseline assessment (16-40 days post-injury). However, very early ISNCSCI assessments in EMSCI may include individuals without severe polytrauma, introducing potential selection bias. Distinct cluster-specific NLI characteristics are also evident: clusters 1 and 6 are dominated by cervical injuries, cluster 5 shifts toward thoracic levels, and clusters 3 and 4 are centered on lower thoracic to upper lumbar levels (T8–L1).
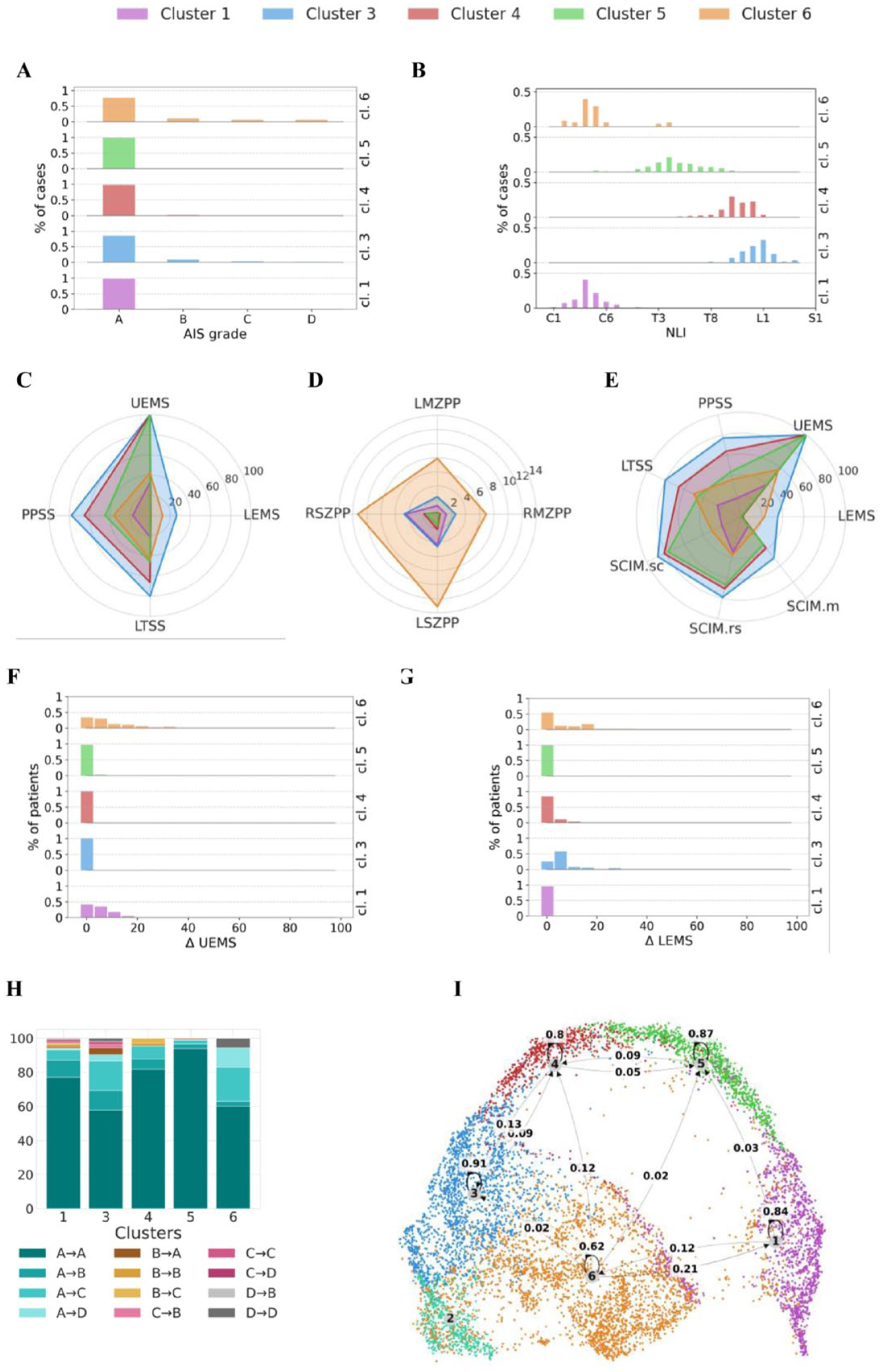
Cluster characteristics of EMSCI analysis cohort: Cluster 2 was omitted as it did not contain any AIS A patients. (A) baseline AIS grade distribution across clusters, where non-AIS A cases represent patients who converted between their first documented assessment and the analysed baseline (16-40 days post-injury); (B) baseline NLI distribution; (C) baseline motor scores (UEMS and LEMS) and sensory scores (PPSS and LTSS); (D) baseline ZPP, including right and left motor (RMZPP, LMZPP) and right and left sensory (RSZPP, LSZPP) components; (E) follow-up motor and sensory scores, and SCIM scores (SCIM.sc—self-care; SCIM.rs—respiration and sphincter management; SCIM.m—mobility); (F and G) delta improvement in upper extremity motor score (ΔUEMS, F) and lower extremity motor score (ΔLEMS, G); (H) AIS grade conversion between the assessments at defined baseline (16-40 days post-injury) and follow-up (150-186 days post-injury); (I) transition probabilities between dataset clusters calculated across all assessments within the baseline and follow-up time intervals. Each row shows the likelihood of moving from 1 cluster at baseline to another cluster at follow-up. Rows with probabilities <.02 were omitted. To facilitate direct comparison, all measures in panels (C-E) are linearly rescaled to a 0 to 100 range, where 0 and 100 correspond to the minimum and maximum values within each assessment, respectively.
Baseline motor (upper extremity motor score, UEMS; LEMS) and sensory (total PPSS); total light touch sensory score, LTSS) function is summarized in Figure 3(C). LEMS values are near zero in clusters 1, 4, and 5, reflecting severe lower extremity impairment, while upper extremity motor function remains largely preserved in clusters 3, 4, and 5, aligned with their thoracic/lumbarNLIs. Sensory function is impaired across all clusters, with the greatest loss observed in cluster 1 and comparatively higher preservation in cluster 3. Patterns of ZPP are further illustrated in Figure 3(D), where cluster 6 shows larger motor and sensory ZPP length, corresponding to a larger degree of residual neurological functions. In contrast, clusters 4 and 5 are characterized predominantly by sensory preservation, and a smaller length of ZPP than observed in cluster 1, suggesting a higher amount of neurological impairment. Follow-up outcomes for LEMS, UEMS, PPSS, LTSS, and SCIM III are presented in Figure 3(E), with corresponding motor improvements (ΔUEMS and ΔLEMS) shown in Figure 3(F) and (G). Consistent with the NLIs, clusters 3, 4, and 5 show no UEMS change. Cluster 1 demonstrates moderate UEMS improvement, while cluster 6 shows a bit larger gains. For LEMS, meaningful improvements are evident in clusters 3 and 6, whereas clusters 1 and 5 show minimal recovery. Cluster 4 shows some LEMS improvement. SCIM III outcomes indicate greater functional independence in clusters 3, 4, and 5, consistent with their thoracic/lumbar NLIs. Notably, cluster 6 displays larger LEMS gains than cluster 1 despite a similar NLI, highlighting clinically relevant differences in recovery potential of the patients graded as AIS A at baseline.
AIS conversion between baseline (16-40 days post-injury) and follow-up (150-186 days post-injury) assessment time points is summarized in Figure 3(H). Clusters 3 and 6 show the highest conversion rates from AIS A to higher grades, with cluster 3 showing 28% conversion to AIS B or C and 4% to D, and cluster 6 showing 23% to AIS B/C and 10% to AIS D. Cluster 5 showed the least improvement, with 94% of individuals remaining AIS A, while clusters 1 and 4 exhibited intermediate conversion rates (cluster 1: 16% from A to B/C and 1% to D; cluster 4: 14% from A to B/C). Detailed information is provided in Table S2 in the Supplemental Results.
Transition probabilities between clusters from baseline (16-40 days post-injury) to follow-up (150-186 days post-injury) assessment time points are depicted in Figure 3(I). Most individuals remained in their baseline cluster at follow-up. Stability was high in clusters 1, 3, 4, and 5 (80%-90%). Cluster 6 was less stable (~62%), with transitions primarily to clusters 1 (~20%) and 4 (~10%). It is important to note that cluster 6 accounts for only about 6% of all AIS A assessments (Table S1 in the Supplemental Results), which may limit the interpretability of these transitions.
External Validation: Sygen Dataset
Inclusion Cohort
The 2-dimensional UMAP representation of the ISNCSCI assessment manifold for the Sygen dataset is shown in Figure 4(A). When EMSCI and Sygen assessments are visualized in a common UMAP space (Figure 4(B)), the 2 cohorts show a natural overlap of ISNCSCI assessment manifolds despite differences in study design, time of data collection, and cohort composition. Although EMSCI covers a broader range of observed assessment patterns, Sygen assessments occupy overlapping regions of the assessment space. This overlap supports the hypothesis that clustering structures learned from EMSCI data are applicable to corresponding regions of the Sygen assessment manifold, such that clusters observed in Sygen are expected to exhibit neurological characteristics similar to those identified in EMSCI. At the same time, some clusters may be underrepresented in the Sygen cohort due to sparser coverage of the ISNCSCI assessment manifold.
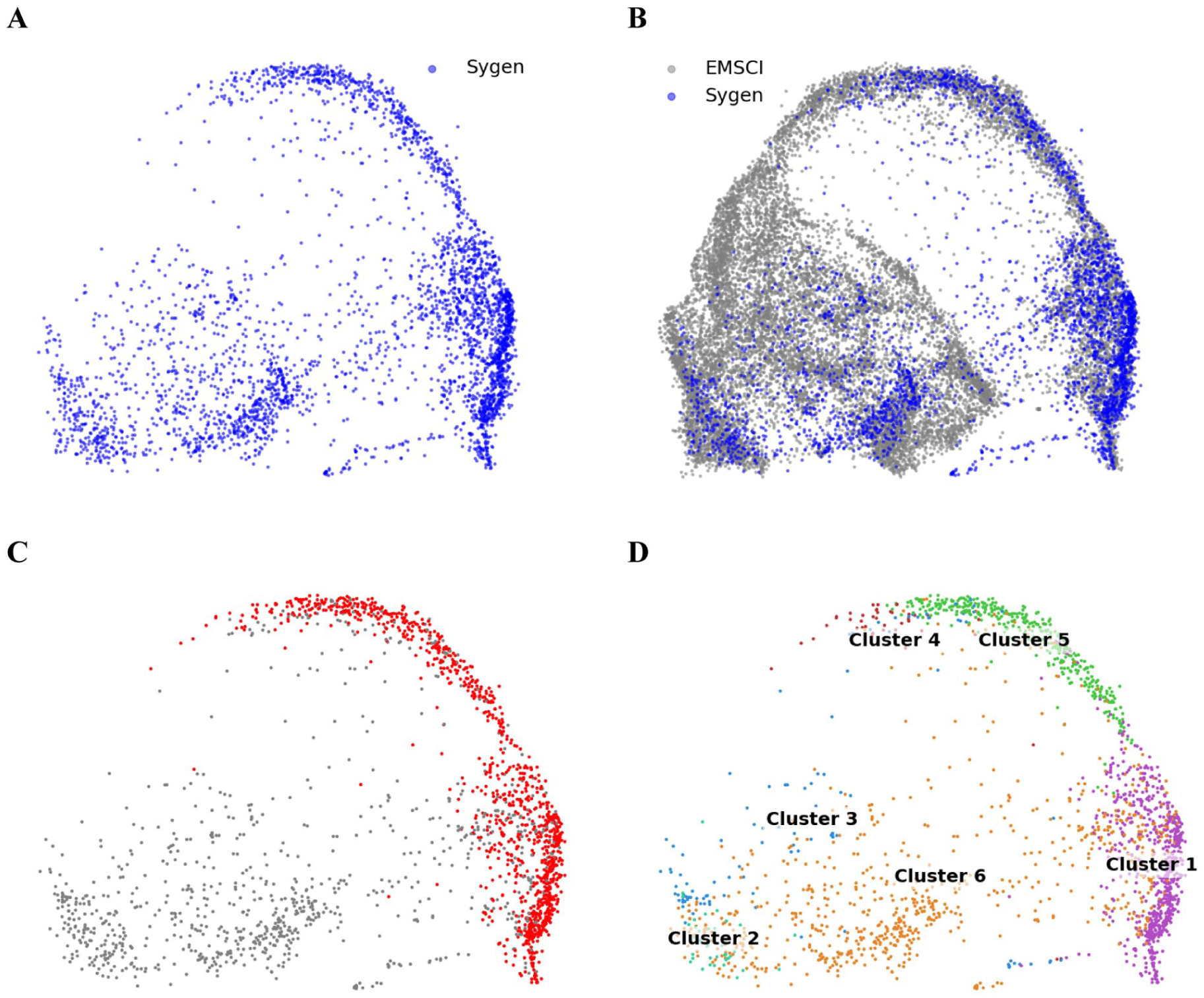
(A) Two-dimensional UMAP representation of the ISNCSCI assessment manifold in Sygen dataset; (B) EMSCI and Sygen ISNCSCI assessments visualized in a common UMAP space, resulting in natural overlap between cohorts; (C) Spatial distribution of AIS A assessments across the ISNCSCI assessment manifold in the Sygen dataset; (D) Cluster assignments within the Sygen ISNCSCI assessment manifold obtained using the DeepDPM model trained on EMSCI dataset.
The spatial distribution of AIS A assessments within the Sygen cohort is shown in Figure 4(C), illustrating their dispersion across the assessment manifold. Cluster assignments inferred using the DeepDPM model trained on EMSCI data are presented in Figure 4(D). Most individuals fall into clusters 1, 5, and 6, whereas clusters 2 to 4 contain relatively few cases. The low representation of clusters 3 and 4 reflects the predominance of lower thoracic neurological levels in these clusters, which are underrepresented in the Sygen cohort. Cluster 2, characterized mainly by cervical injuries with AIS D and relatively preserved sensory function, is also sparsely represented, whereas comparable cervical AIS D cases in Sygen are more frequently assigned to cluster 6, which exhibits greater sensory impairment. A summary of cluster distribution is provided in Table S3 in the Supplemental Results.
Analysis Cohort
Baseline (16-40 days) post-injury characteristics of the Sygen analysis cohort and the corresponding cluster composition are listed in Table 1. Because clusters 2 to 4 do not contain a sufficient number of patients (no patients in clusters 2 and 3 and only 5 in cluster 4), they were not included in subsequent analyses. The distributions of AIS grades and NLI at baseline (16-40 days post-injury) assessments, shown in Figures 5(A) and (B), closely mirror the patterns observed in the EMSCI dataset. Clusters 1 and 5 consist almost entirely of AIS A cases (99% and 100%, respectively), while cluster 6 includes a mix of complete and incomplete injuries (AIS B/C, 44%).
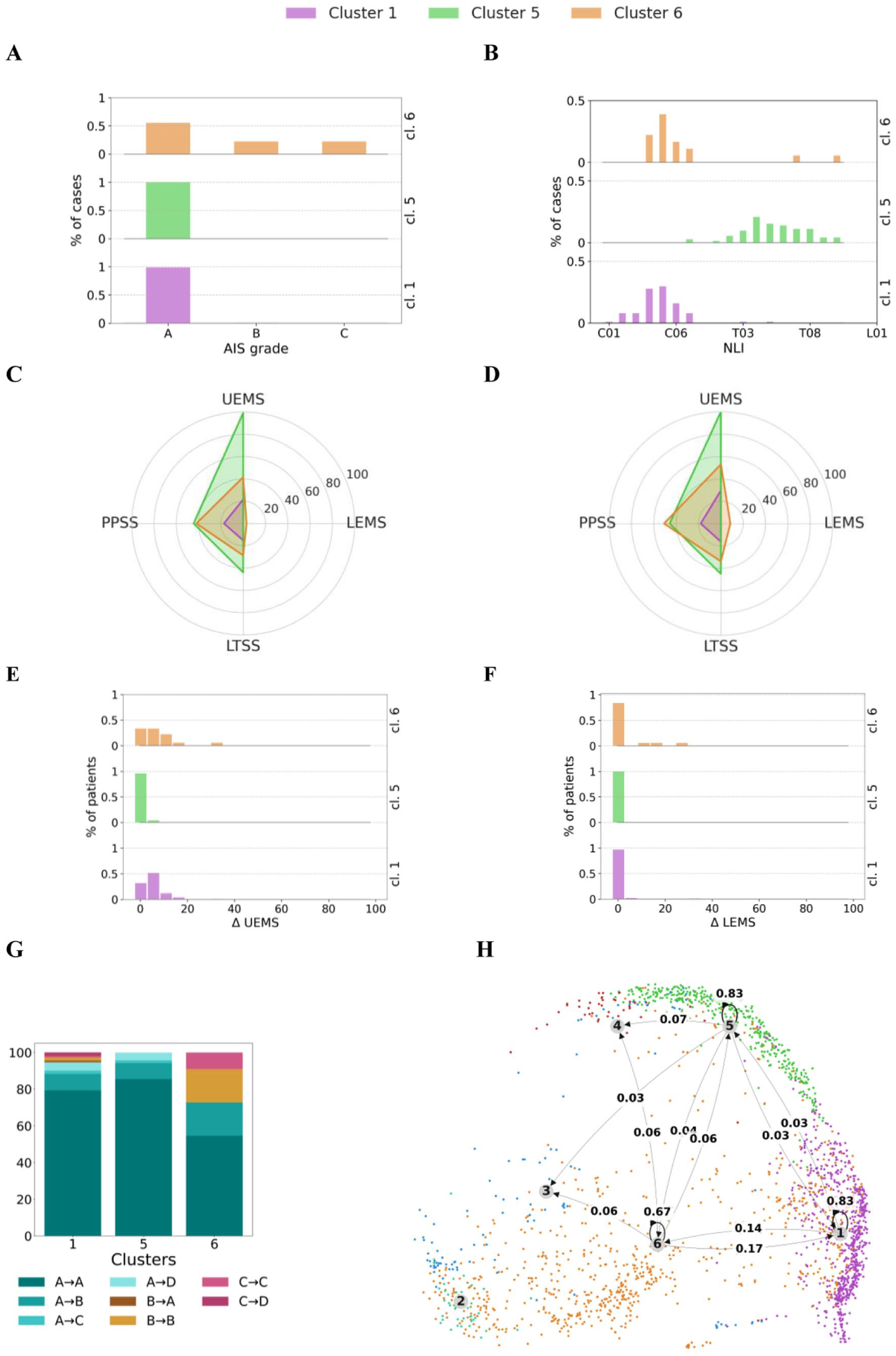
Sygen dataset: (A and B) AIS grade and NLI distributions for the selected clusters; (C and D) total motor and sensory scores at baseline (C) and follow-up (D); (E and F) changes in upper extremity motor score (ΔUEMS, E) and lower extremity motor score (ΔLEMS, F) from baseline to follow-up; (G) AIS grade conversion within each cluster between baseline and follow-up; (H) transition probabilities between dataset clusters calculated across all assessments within the baseline and follow-up time intervals. Each row shows the likelihood of moving from 1 cluster at baseline to another cluster at follow-up. Rows with probabilities <.02 were omitted. Results for clusters 2 to 4 are excluded due to insufficient data. To facilitate direct comparison, all measures in panels (C-D) are linearly rescaled to a 0 to 100 range, where 0 and 100 correspond to the minimum and maximum values within each assessment, respectively.
Motor and sensory outcomes at baseline (16-40 days post-injury) and follow-up (165-210 days post-injury), along with changes in UEMS and LEMS (ΔUEMS and ΔLEMS), are presented in Figures 5(C) to (F). The overall levels of impairment and the magnitude of improvement align with EMSCI findings across neurological levels covered by EMSCI and represented in the Sygen cohort, supporting the generalizability of the clustering structure within this shared NLI range to an independent cohort.
AIS grade changes between baseline and follow-up are summarized in Figure 5(G). Clusters 1 and 5 remain largely composed of AIS A cases at follow-up (80% and 86%, respectively), with approximately 15% converting to less severe grades (AIS B-D). Compared with EMSCI, conversion rates in cluster 1 are similar across cohorts, whereas cluster 5 shows a higher conversion rate in Sygen (~14%) than in EMSCI (~6%). In cluster 6, around 18% of individuals convert from AIS A to B, while the remainder maintain their baseline AIS classification, whereas in EMSCI about 34% convert from AIS A to a higher grade. Detailed information is provided in Table S4 in the Supplemental Results.
Transitions between clusters from baseline (16-40 days post-injury) to follow-up (165-210 days post-injury) are shown in Figure 5(H). As in the EMSCI cohort, cluster stability is high: about 83% of individuals in clusters 1 and 5 remain in the same cluster at follow-up. Cluster 6 exhibits lower stability (~67%), with movement primarily with cluster 1. Approximately 17% of cluster 6 individuals transition to cluster 1, while 14% of those initially in cluster 1 move to cluster 6, closely reflecting the transition patterns observed in EMSCI.
Discussion
In this study, we introduce a fully data-driven framework for SCI severity stratification based exclusively on ISNCSCI examination features to complement current AIS grading. Using a probabilistic deep clustering model, we identified 6 clusters representing distinct patterns of neurological impairment and sparing. This stratification emerges solely from ISNCSCI motor, sensory, VAC, and DAP features, enabling an unbiased comparison with conventional classifications, including AIS grade, NLI, and recovery profiles. This approach uncovers substantial heterogeneity within individuals classified as AIS A, emphasizing differing levels of neurological sparing and recovery potential amongst these injuries. The evaluation in the independent Sygen dataset supports the robustness of the proposed stratification at the level of neurological patterns, despite differences in cohort definition and assessment timing. While the exact cluster structure differs between datasets, consistent associations between cluster membership, preserved neurological function, and recovery were observed. These findings suggest that the data-driven stratification captures meaningful variation, and may complement existing measures such as AIS grade by providing a more granular description of neurological status and recovery potential.
The need for improved stratification methods in SCI has been emphasized for more than a decade. Several studies have shown that AIS grade and NLI only partially capture the biological extent of injury and cannot resolve the variability in spontaneous recovery within nominally homogeneous groups (eg, AIS A cervical injuries).27,36-40 As a result, current clinical trials often enroll highly heterogeneous cohorts, which complicates statistical evaluation by increasing noise and thereby may obscure treatment effects.18,19,27 Previous approaches such as Unbiased Recursive Partitioning with Conditional Inference Trees (URP-CTREE) have improved stratification by identifying more homogeneous clusters at follow-up in respect to a predefined study endpoint based on for example early upper extremity motor scores or other baseline predictors.16,41 As in the present work, these approaches require baseline assessments and follow-up endpoints. However, in URP-CTREE the definition of subgroups is explicitly optimized for associations with a selected future outcome, making the resulting stratification sensitive to the timing and characteristics of the baseline assessment and to the choice of endpoint. In contrast, the proposed approach uses ISNCSCI data to derive outcome-agnostic clusters, while baseline and follow-up assessments are used solely to evaluate recovery trajectories and clinical relevance. By leveraging ISNCSCI assessments across different clinical phases, the proposed approach reduces reliance on a single predefined baseline examination, a known limitation of outcome-driven stratification models.16,41,42 Moreover, AIS grade and NLI are not used as model inputs, ensuring that discovered clusters provide a perspective on injury severity independent from those widely used ISNCSCI classification variables. Finally, unlike URP-CTREE, DeepDPM does not rely on recursive splitting of predefined clinical variables, but instead infers cluster structure directly from the joint distribution of ISNCSCI features without enforcing decision tree-based partitions.
Within this landscape, we observed that patients classified as AIS A contribute to a variety of subpopulations with substantial differences in the associated functional ability and recovery potential while simultaneously aligning well with known clinical patterns. Clusters 1, 4, and 5 capture the majority of AIS A cases, with clear differences between cervical and thoracic injuries and between patients with high levels of preserved function and those with minimal preserved function after injury. Clusters 3 and 6 identify groups with early signs of preserved function, either through larger ZPP lengths or higher below-NLI motor and/or sensory scores. These groups show substantially higher AIS conversion rates and greater LEMS gains despite originating from identical classification as AIS A. These findings are consistent with prior observations that patients with similar baseline classifications can follow different recovery trajectories and achieve different outcomes.17,27,43,44 Importantly, our clustering results demonstrate that individuals classified as AIS A exhibit meaningful variation in preserved neurological function, supporting prior evidence of substantial heterogeneity across cervical and thoracic spinal cord injuries, as reported using both clinical and imaging-based assessments.37,38,45,46 In summary, we hence offer a more refined subgrouping within the AIS A category that accounts for detailed and holistic patterns of retained sensory-motor function.
The external validation using the Sygen dataset further supports the robustness and generalizability of the clustering solution. Despite substantial differences between EMSCI and Sygen in data collection practices and demographics, the cluster-specific neurological profiles, AIS distributions, patients’ recovery potential, and conversion rates were highly consistent. This cross-cohort reproducibility indicates that the identified clusters reflect underlying neurological patterns rather than dataset-specific properties. Importantly, this demonstrates that clinically acquired ISNCSCI examinations contain sufficient information to support reproducible, data-driven stratification across independent cohorts.
Beyond characterizing heterogeneity, our findings have direct implications for clinical trial design. Enriched enrollment strategies increasingly rely on stratification methods that can identify participants with comparable neurological severity and recovery potential. 47 The clusters presented here offer a reproducible and outcome-agnostic basis for selecting more homogeneous cohorts or performing stratified randomization. For example, the distinction between “severe cervical with minimal sparing” (cluster 1) and “cervical with early residual function” (cluster 6) could aid in reducing within-group variability and improving power to detect treatment effects. Similarly, thoracic clusters (clusters 4 and 5) differ in recovery potential despite both being dominated by paraplegic AIS A injuries, suggesting that additional granularity beyond conventional AIS-based classifications may help refine cohort definition in future clinical trials.
Beyond clinical trial design, an important question is how such data-driven stratification could be translated into clinical practice. The proposed framework could be extended to a decision-support setting in which an individual patient’s ISNCSCI assessment is mapped to the closest cluster, thereby providing a more refined characterization of the neurological impairment within the AIS A. This cluster assignment could then be linked to observed recovery profiles (eg, expected ranges of motor recovery or likelihood of AIS conversion), offering a complementary, data-driven perspective to current prognostic approaches such as AIS conversion.
Limitations
A key limitation of our analysis is that the current ISNCSCI-derived clustering primarily captures neurological function rather than providing a comprehensive, multimodal representation of injury severity and recovery potential. Important clinical domains, such as autonomic function, pain, spasticity, and biomarkers, including liquid (eg, serum or CSF) or MRI-derived measures, are not incorporated due to their absence in the studied cohort. Integrating such complementary information may provide a more nuanced understanding of recovery mechanisms and help clarify why certain subgroups show differential outcomes.38,42,44 For instance, multimodal data might help disentangle the relative contributions of lesion characteristics, neuroplasticity, and rehabilitation intensity to observed functional gains.
The heterogeneity of rehabilitation and clinical interventions across patients should also be noted. Neither EMSCI nor Sygen systematically captures differences in therapy intensity and duration, or treatments for secondary complications or other medical conditions, which may influence neurological recovery after SCI. Consequently, some observed differences between clusters may reflect variation in rehabilitation exposure rather than purely intrinsic neurological potential.
A further limitation relates to non-uniform availability of ISNCSCI assessments at very acute time points (0-15 days post-injury). Very early examinations are frequently missing in patients with severe injuries due to medical instability. As a result, individuals whose first documented assessment occurred later (eg, 16-40 days post-injury) and were classified as AIS A were assumed to have been AIS A at earlier stages, with the missing assessments reflecting severity-related unavailability rather than neurological deterioration. While deterioration to AIS A at selected baseline (16-40 days post-injury) is considered unlikely, this assumption may nonetheless introduce selection bias that should be considered when interpreting the composition of AIS A clusters.
Supplemental Material
sj-docx-1-nnr-10.1177_15459683261454947 – Supplemental material for Unsupervised Data Driven Clustering of the Neurological Assessments of People With Traumatic SCI Focusing on Sensorimotor Complete Injuries
Supplemental material, sj-docx-1-nnr-10.1177_15459683261454947 for Unsupervised Data Driven Clustering of the Neurological Assessments of People With Traumatic SCI Focusing on Sensorimotor Complete Injuries by Olga Taran, Rüdiger Rupp, Louis P. Lukas, Adrian Kaufmann, Norbert Weidner, Martin Schubert, Björn Zörner, Frank Röhrich, Josina Waldmann, Yorck B. Kalke, Rainer Abel, Doris Maier, Fred H. Geisler, Armin Curt, Catherine R. Jutzeler and Sarah C. Brüningk in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgements
We acknowledge the use of AI tools in this work to improve language. All text was originally written by the authors, partially enhanced with the assistance of ChatGPT, and the final version reviewed and approved by the authors.
List of Abbreviations/Glossary
AIS American Spinal Injury Association Impairment Scale
DAP Deep anal pressure
DeepDPM Deep Dirichlet Process Mixture
EMSCI European Multicenter Study about Spinal Cord Injury
ISNCSCI International Standards for Neurological Classification of SCI
LEMS Lower extremity motor score
LTSS Light touch sensory score
MS Motor score
NLI Neurological level of injury
PPSS Pin prick sensory score
SCI spinal cord injury
SCIM Spinal Cord Independence Measure
SS Total sensory score
TMS Total motor score
UEMS Upper extremity motor score
UMAP Uniform Manifold Approximation and Projection
VAC Voluntary anal contraction
ZPP Zone of partial preservation
Author Contributions
Olga Taran: Conceptualization; Formal analysis; Investigation; Methodology; Software; Validation; Visualization; Writing—original draft; and Writing—review & editing. Rüdiger Rupp: Conceptualization; Methodology; and Writing—review & editing. Louis P. Lukas: Conceptualization and Writing—review & editing. Adrian Kaufmann: Conceptualization and Writing—review & editing. Norbert Weidner: Conceptualization; Methodology; and Writing—review & editing. Martin Schubert: Conceptualization; Methodology; and Writing—review & editing. Björn Zörner: Investigation and Writing—review & editing. Frank Röhrich: Investigation and Writing—review & editing. Josina Waldmann: Investigation and Writing—review & editing. Yorck B. Kalke: Investigation and Writing—review & editing. Rainer Abel: Investigation and Writing—review & editing. Doris Maier: Investigation and Writing—review & editing. Fred H. Geisler: Investigation and Writing—review & editing. Armin Curt: Conceptualization; Methodology; and Writing—review & editing. Catherine R. Jutzeler: Conceptualization; Funding acquisition; Methodology; Supervision; and Writing—review & editing. Sarah C. Brüningk: Conceptualization; Funding acquisition; Methodology; Supervision; and Writing—review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project and O. Taran were supported by the Wings for Life Foundation (grant #2024_301). O. Taran was additionally supported by the International Foundation for Research in Paraplegia (IRP #P207). S. Brüningk was funded by the Swiss National Science Foundation under TMSGI3_225913.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplementary Material
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.