
Abstract
High-intensity training (HIT) focused on stepping practice consistently improves clinical locomotor outcomes in individuals with neurologic injury. However, traditional HIT approaches typically do not target underlying impairments, and gains in non-locomotor tasks (ie, balance and transfers) or daily stepping are limited. One strategy to address these limitations involves providing HIT in variable contexts by progressively increasing locomotor demands across diverse environments while targeting specific biomechanical deficits (ie, limb-swing, propulsion, stance, and postural stability). This approach parallels the concept of “shaping” used successfully in constraint-induced movement therapy trials pioneered by Dr. Steven Wolf. The rapid progression of variable, difficult stepping tasks during HIT produces gains in multiple locomotor and non-locomotor outcomes, although, importantly, the accelerated progression of task demands and acceptance of movement variability represent key departures from conventional rehabilitation frameworks emphasizing gait quality. Together, this focus on progression and variability is likely responsible for the observed gains. In this issue honoring Dr. Steven Wolf, we delineate the shaping principles applied to locomotor rehabilitation following neurologic injury. We outline the rationale for HIT in variable contexts, explain how biomechanical targeting guides intervention progression, and present evidence detailing its observed efficacy in improving clinical and community mobility outcomes. We also describe how advanced robotic technology can further enhance locomotor outcomes by applying progressive resistance to target specific locomotor deficits. By integrating principles of biomechanics with long-standing theories in motor learning, we believe HIT in variable contexts can further harness the neural plasticity of the nervous system to maximize locomotor function following neurologic injury.
Keywords
Introduction
The incidence of acute-onset neurologic injury, including stroke, spinal cord injury (SCI), and traumatic brain injury (TBI), continues to increase, with concomitant increases in survival resulting in a growing population living with long-term neurologic impairments.1-3 In those with residual lower extremity function, recovery of ambulation is often a primary goal, yet many continue to experience deficits in walking independence, speed, and endurance. Long-standing data suggest strength and balance impairments are primary determinants of locomotor dysfunction,4-6 although interventions that directly target these deficits in isolation have produced inconsistent gains in walking function. 7 Rather, attempts to maximize task-specific (ie, walking) practice, particularly when delivered at higher cardiovascular intensities (high-intensity training, or HIT), have been shown to elicit relatively consistent gains in gait speed and endurance.7-16 Nonetheless, traditional HIT approaches that emphasize forward walking often demonstrate limited gains in non-locomotor outcomes (ie, balance and transfers)12-14 and minimal changes in daily stepping activity in the home and community, despite improvements in clinical measures of walking capacity. 17 These results reinforce principles of task specificity but also raise concern that focusing solely on forward walking may be insufficient to address broader functional limitations.
One strategy that may mitigate these limitations involves providing HIT in variable contexts, which entails practicing varied, challenging locomotor tasks (eg, multidirectional walking, stepping over uneven, compliant, or narrow surfaces, and stair climbing) in different environments (eg, overground and treadmill). Previous studies in individuals with acute-onset neurologic injury8,10,11,18 have described the utility of this strategy for improving locomotor and non-locomotor outcomes (ie, balance and transfers) to a greater extent than standard walking practice, supporting the concept of task transfer.
Training in variable contexts also focuses on progression of task difficulty to address specific biomechanical deficits (eg, limb swing, propulsion, stance control, and postural stability), 10 an approach that parallels the concept of “shaping” used in constraint-induced movement therapy (CIMT) trials pioneered by Dr. Steven Wolf, PT, PhD. 19 Shaping is defined as a method in which motor tasks are learned or relearned by progressively increasing task difficulty in accordance with the patient’s capabilities while maintaining a manageable level of success.19-21 However, an emphasis on progressively increasing task difficulty during HIT while targeting specific biomechanical deficits coupled with a de-emphasis on normalizing kinematics contrasts sharply with conventional strategies.22,23 Accumulating evidence suggests these features, rather than strictly focusing on gait quality, may be the primary contributors to the functional gains observed.8,24
In this manuscript for the issue dedicated to Dr. Wolf, we delineate how shaping principles can be applied to locomotor training following neurologic injury. We outline the rationale for HIT in variable contexts, describe how biomechanical targeting guides rapid progression of stepping tasks, and summarize evidence for its efficacy in improving both clinical and community mobility outcomes. We also discuss how advanced robotic technologies may further enhance locomotor outcomes by applying progressive, task-specific resistance to target particular biomechanical deficits. By integrating principles of exercise physiology and biomechanics with long-standing theories of motor learning and shaping, we propose that HIT in variable contexts, augmented when appropriate by robotic technologies, can more fully harness neural plasticity to maximize locomotor and non-locomotor recovery following neurologic injury.
Rationale for HIT in Variable Contexts: The Concept of Task-Transfer
Although evidence supporting HIT focused on walking in individuals with neurologic injury continues to grow, much less attention has been given to incorporating variable stepping tasks within HIT. Early studies targeting higher aerobic intensities using only forward treadmill or overground walking revealed consistent gains in walking outcomes, but minimal effects on unpracticed tasks (ie, task transfer) such as balance or sit-to-stand performance.3,12-14 While these results reinforced a fundamental principle of task-specificity in motor learning, they also raised concern that this might shift focus toward more balance and sit-to-stand training, thereby reducing the amount of stepping practice.
An alternative approach involves integrating diverse stepping activities into HIT that are biomechanically similar to non-stepping tasks, thereby facilitating task-transfer. 25 Task-transfer occurs when unpracticed tasks share similar biomechanical demands and neural control strategies with practiced tasks. For example, stair climbing requires greater hip and knee extensor demands than overground walking, but is comparable to the neuromuscular requirements associated with sit-to-stand performance. Similarly, multidirectional stepping, or walking on compliant or uneven surfaces, challenges postural stability to a greater extent than forward treadmill walking, particularly when using a handrail. Practice of HIT in variable contexts can also simulate many of the mobility barriers encountered in the home and community, which may facilitate gains in daily stepping activity.
Identifying and Progressing Task Demands During Locomotor Training
Previous studies have detailed considerations associated with providing HIT in variable contexts, including identifying which tasks to practice and strategies to alter task difficulty. 10 While a shared strategy among therapists is to address the specific locomotor deficits that patients present with, various rehabilitation frameworks differ in which deficits are prioritized and how they should be addressed. For example, adherents of neurodevelopmental, or Bobath, treatment 22 emphasize preparatory gait strategies (ie, pre-gait) such as sitting with progression to quadruped or tall kneeling, and eventually standing, weight-shifting, and walking while maintaining “correct” kinematics. Although this strategy has been used for decades in individuals with neurologic injury, this gradual progression substantially limits the amount of stepping practice, which likely contributes to its limited efficacy in improving locomotor function. 26 Conversely, other strategies, such as body weight-supported treadmill training, skip preparatory gait exercises, and attempt to maximize stepping but reduce task demands by focusing on normalizing kinematics.23,27,28 Specific attention is directed towards limb loading and hip extension in stance and facilitating normal hip and knee swing-phase kinematics with appropriate spatiotemporal symmetry, all of which are thought trigger afferent signals that drive locomotor output. The focus on “good stepping” 27 also minimizes abnormal kinematic patterns, likely in an effort to avoid reinforcing compensatory strategies, with eventual progression to variable stepping tasks (ie, gait adaptability). Unfortunately, studies focusing on normalizing kinematic patterns do not consistently improve function or kinematics, particularly when compared with strategies that do not prioritize kinematics.23,29,30
An alternative approach focuses on targeting specific biomechanical deficits underlying locomotor dysfunction. Given the findings of previous studies focused on normalizing gait kinematics during locomotor training, attention in this paradigm is directed towards the muscle forces or joint powers necessary to accomplish upright locomotion. Previous work has identified 4 key biomechanical subcomponents of gait by their relative contributions to the mechanical and metabolic costs of locomotion.31-35 Primary subcomponents include those responsible for forward progression, such as propulsion, which is generated primarily by the plantarflexors in late stance and accounts for ~50% of the metabolic cost of walking, and limb swing, accomplished through hip flexor power generation (~10% of metabolic costs). Additional subcomponents are responsible for maintaining upright posture, including stance control, which involves maintaining hip and knee extensor activity to limit limb collapse (~25%) and lateral or postural stability, which relates to maintaining the center of mass over the actual or extrapolated base of support (~6%). While these proportions may not directly apply to neurologic populations presenting with heterogenous deficits, the use of these subcomponents provides a framework for identifying which deficits most limit an individual’s locomotor performance. Critically, this approach de-emphasizes normalizing the quality of movement during locomotor tasks (ie, kinematics) in favor of accomplishing the task (ie, function).
The subsequent challenge is identifying which deficits warrant attention, and determining how to progress interventions to address them. A conceptual framework to gauge task difficulty is shown in Figure 1(A) illustrating the relationship between the degree of recovery of locomotor deficits and the level of assistance or task difficulty. For example, individuals with severely limited function would require complete assistance (ie, guidance) to ensure continuous stepping (left side of curve). Such assistance for those with substantial loss of stance control (ie, complete limb collapse) would consist of considerable body-weight support, typically through a counterweight-harness system, simply to remain upright. Similarly, in those with minimal limb swing, physical guidance by therapists is needed to facilitate stepping.
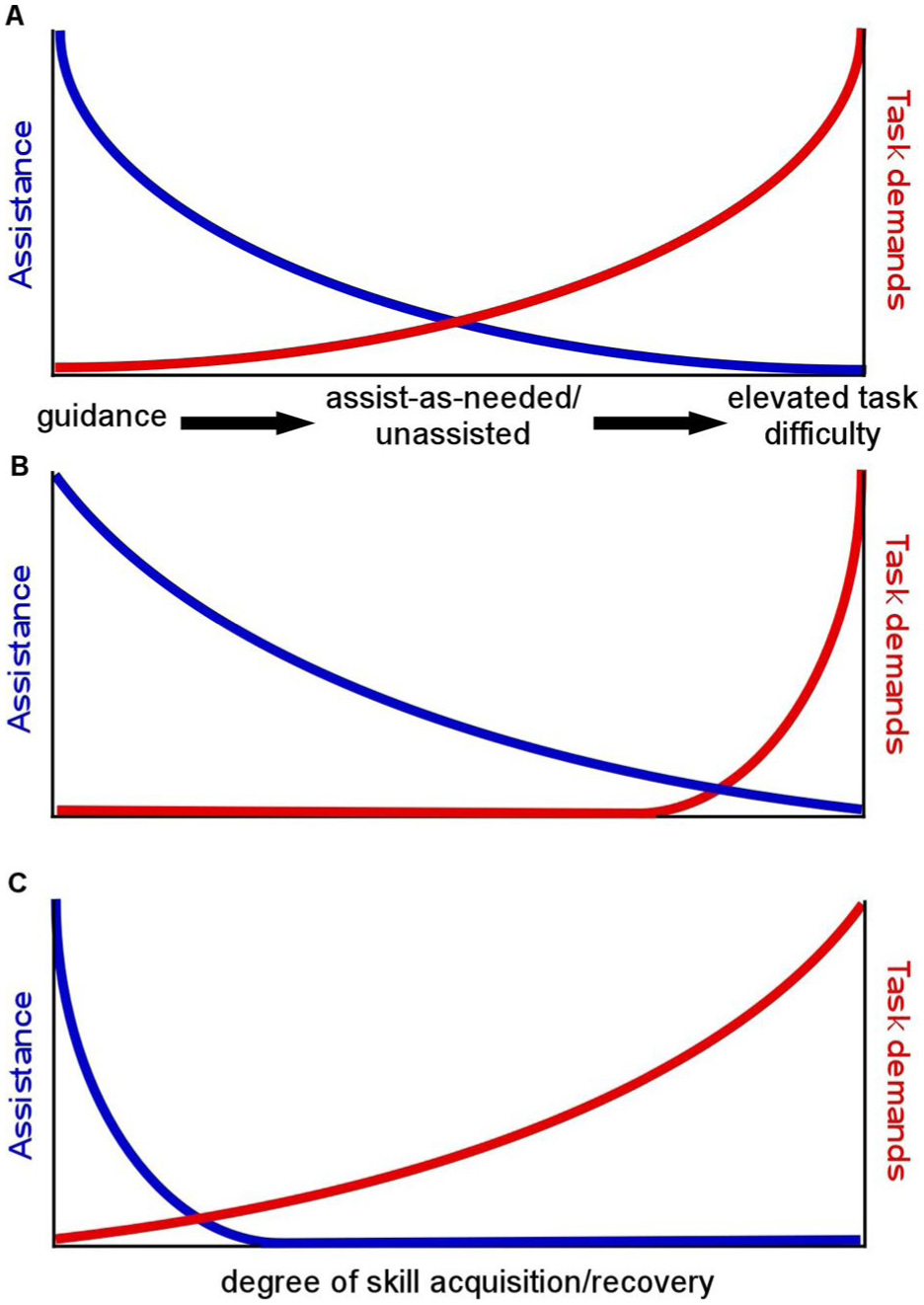
(A) Schematic of relationship between locomotor recovery and use of assistance or increases in task demands to continue to progress gains in function. (B) Alterations in schematic with strategies ensuring kinematic quality, with protracted assistance, and limited task variability. (C) Shift in schematic with focus on biomechanical deficits with reduced assistance and increased task difficulty early during recovery.
As locomotor function improves, reducing the level of assistance is warranted to progress task demands and maximize volitional effort. Progression strategies often include reducing weight support for stance or minimizing limb swing assistance, although modulating such assistance may be necessary with short-term fluctuations in motor function (eg, fatigue). Unlike other gait training strategies, however, minimal attention is directed towards normalizing kinematics8,10,11 except for corrective bracing to prevent injury (ie, knee hyperextension or ankle inversion). Rather, the primary focus remains on encouraging maximal volitional engagement. Even though patients may generate inconsistent stepping patterns, such movement variability may elicit implicit mechanisms of motor learning that enhance motor performance. 36 With further recovery, task demands increase rapidly. Strategies targeting limb swing often include stepping over obstacles or using leg weights, even when individuals can only minimally generate a positive step length, whereas stance-phase challenges can involve ascending stairs or using a weighted vest. Simultaneous increases in propulsive demands may include walking faster, on inclines, or with propulsive resistance (posterior elastic restraint), with additional challenges to postural stability such as walking on compliant and uneven surfaces, and performing multidirectional stepping.
Applying “Shaping” to Locomotor Training
The concepts of reducing assistance and progressing task difficulty during physical rehabilitation are not novel; rehabilitation professionals have long understood the need to progressively increase task demands to continually elicit gains in performance. In the field of motor control, these ideas are consistent with the guidance hypothesis 37 and the challenge point framework, 38 in which gradually reducing physical, visual, or verbal assistance is accompanied by subsequent increases in task demands with improved performance. These frameworks parallel the concept of “shaping” that was integral to the CIMT protocols Dr. Wolf helped translate from primate studies. 19 In CIMT, shaping involves adaptive task practice in which upper extremity task demands are progressively adjusted according to the patient’s capabilities, and usually targeting a 60% to 80% success rate, similar to the challenge-point hypothesis, which produced significant gains in paretic arm function post-stroke. 19
When applying the concept of “shaping” during locomotor training, rehabilitation strategies as depicted in Figure 1(A) differ as to how “success” is defined, and the relative difficulty of task demands applied. When using neurodevelopmental strategies or weight-supported treadmill training, for example, ensuring normal kinematics with physical assistance is a primary goal, and progression is based on achieving certain kinematic milestones even if practiced tasks are very different. Accordingly, progression of task demands would not receive equivalent attention, with protracted assistance to ensure normal kinematics and more gradual or limited increases in task difficulty as depicted in Figure 1(B). Conversely, with HIT in variable contexts, physical assistance is reduced as rapidly as possible in large part because normalizing gait kinematics is not a primary focus. Rather, “success” is simply the completion of the stepping task as defined for each biomechanical subcomponent, including positive step lengths (ie, swing phase and propulsion), limited limb collapse (stance), or loss of balance (postural stability), with progression in a specific direction (propulsion). For this strategy, there is no percentage threshold for success, although the inability to complete stepping tasks for 3 to 5 consecutive steps warrants reduction of task difficulty. 10 Accordingly, “success” may therefore not nearly reach the 60% to 80% threshold utilized in other motor control frameworks,19,38 as long as participants can tolerate multiple mistakes. The rapid reduction in assistance as needed and acceleration of task demands would therefore occur earlier in the recovery process as depicted in Figure 1(C).
During application of HIT in variable contexts, use of the strategies delineated above is associated with considerably fewer steps achieved per training session (~3000) than providing forward treadmill stepping alone (~4000).10,11,18 Nonetheless, gains in both locomotor and non-locomotor outcomes were still substantial. For example, in the Variable Intensive Early Walking post-Stroke trial in individuals <6 months post-stroke, improvements in locomotor function were ~3-fold greater than conventional interventions providing a similar number of training sessions targeting lower intensities (40%-50% heart rate reserve). 11 Additional findings included significant gains in balance and sit-to-stand transfers from baseline assessments in both HIT and conventional therapies that were not significantly different between training groups. More directly, those assigned to conventional training practiced both standing balance and sit-to-stand tasks, while participants receiving HIT in variable contexts practiced only stepping. These data are consistent with the concept of “reverse transfer” 18 or the “leap-frog” hypothesis, 39 in which practicing more dynamic, difficult tasks would facilitate gains in less challenging tasks such that their practice was unnecessary.
A subsequent larger study in ambulatory individuals with chronic stroke revealed similar changes, but also further clarified the unique contributions of HIT in variable contexts as compared to HIT providing only forward walking. In the Very Intensive Variable Repeated AmbulatioN Trial (VIVRANT), 8 90 ambulatory individuals received either HIT in variable contexts, HIT performing only forward walking on a treadmill and overground (both targeting >70% heart rate reserve) or low-intensity variable training (<40% heart rate reserve). Outcomes following training also revealed 2- to 4-fold greater gains in gait speed and endurance (Figure 2(A) and (B)) following either HIT intervention as compared to low-intensity training, emphasizing the utility of targeting higher intensities. HIT in variable contexts also resulted in greater gains in dynamic postural stability using the Functional Gait Assessment (P = .03 intent-to-treat vs P = .06 on-protocol analyses; Figure 2(C)) and selective gains in the balance confidence (Activities-specific Balance Confidence scale), with minimal changes in the other 2 groups. Notably, daily stepping in the home and community also improved significantly from baseline only in those who received HIT in variable contexts (Figure 2(D)). 40 It was hypothesized that the collective gains in clinical measures of locomotion, balance, and balance confidence may have contributed to improvements in daily stepping.
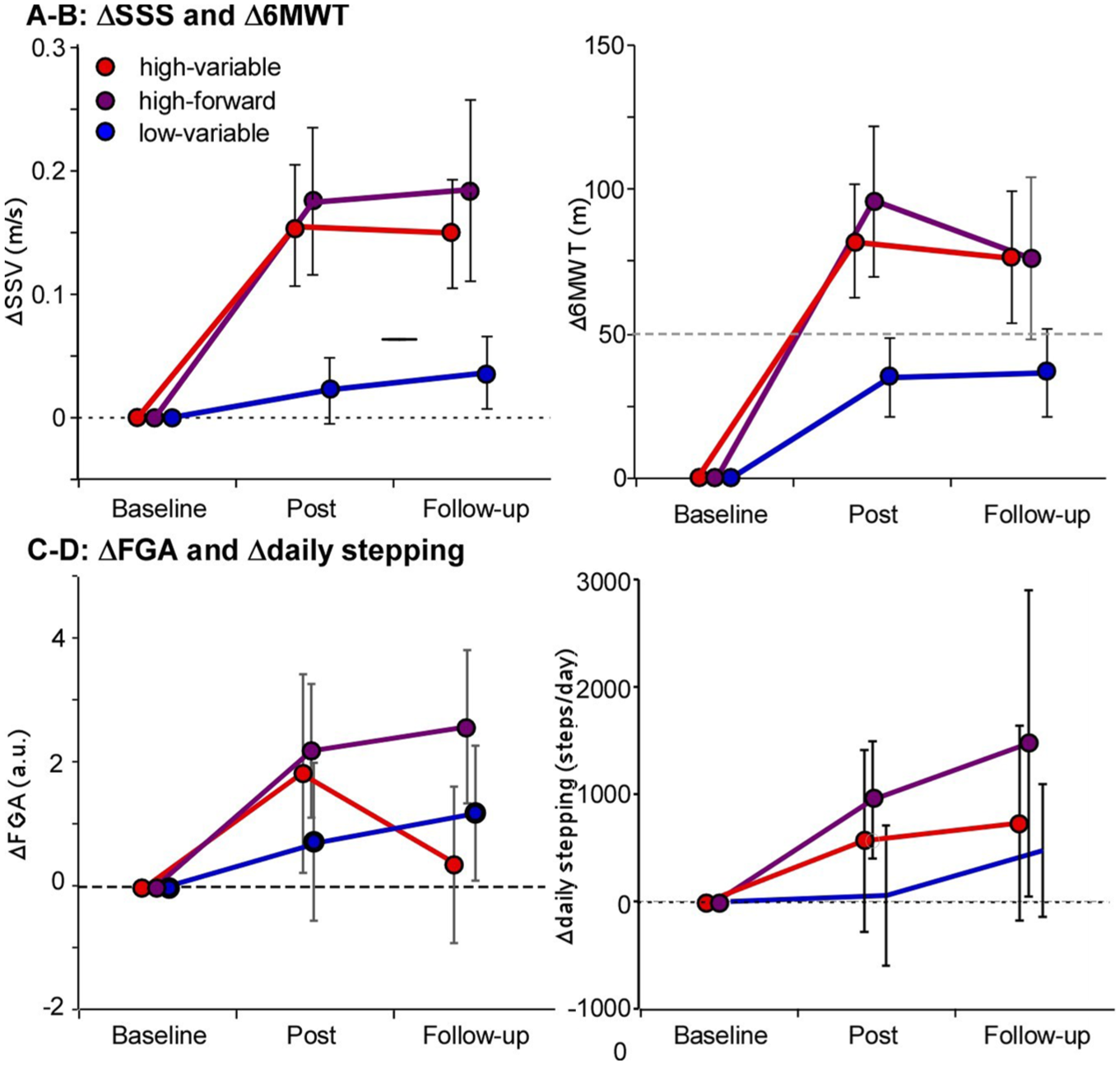
(A and B) Changes in self-selected speeds and 6-min walk test in Very Intensive Variable Repeated AmbulatioN Trial, indicating greater gains in either high-intensity training (HIT) group. (C and D) Gains in Functional Gait Assessment and daily stepping only observed with HIT in variable contexts.
Given the combined findings of gains in transfers as well as static or dynamic postural stability, the strategy of providing HIT in variable contexts allows therapists to prioritize stepping activities over other exercises during training sessions. An argument could be made that practice of these other tasks might still be important and the focus away from all stepping training may not substantially reduce the combined gains in locomotor tasks. However, given the associations between amount of stepping practice and changes in locomotor outcomes,8,11,12 and the findings presented above, it is uncertain what advantage this strategy would provide. The use of this strategy has shown to be successful in individuals post-stroke, with recent data in those with chronic motor incomplete SCI24,41 or TBI, 42 although more data is needed to evaluate the consistency of findings in selected populations, including in those early following injury.
With the documented gains associated with HIT in variable contexts, the combined contributions of stepping variability and intensity warrant closer consideration. More directly, practicing variable stepping tasks but without targeting higher intensities (ie, low-intensity training) revealed minimal changes in all locomotor outcomes. This finding is consistent with 5 separate studies in individuals with stroke or SCI evaluating variable stepping tasks43-47 without emphasizing intensity, which reported similar or worse outcomes as compared to other strategies. In contrast, the combination of intensity and stepping variability while targeting specific biomechanical deficits appears to be critical because it substantially elevates task demands. For example, enhancing limb-swing demands during variable stepping training might involve stepping over obstacles or adding ankle weights, although HIT in variable contexts often combines these strategies at faster speeds, which increases hip flexor demands. Similarly, stance deficits can be targeted using weighted vests or practicing stair climbing, although their combination with HIT would substantially increase stance and propulsive demands. This combination is somewhat akin to performing strengthening within locomotor tasks during HIT and is likely a critical factor that elicits gains in non-locomotor outcomes or community mobility that are not evident with variable practice at lower intensities, or with HIT alone.
Biomechanical Changes Associated With HIT in Variable Contexts
An important benefit of providing HIT in variable contexts, particularly when focusing on biomechanical deficits, is the resulting improvements in biomechanical measures (ie, kinematics and kinetics) following training. Prior studies in individuals with stroke and incomplete SCI have demonstrated gains in lower extremity kinematics with HIT, including greater step length, cadence, and spatiotemporal symmetry, with associated increases in hip and knee range of motion and intralimb consistency indicative of improved coordination.48-51 These findings emerged despite limited explicit emphasis on normalizing kinematics during training, demonstrating that practicing challenging locomotor tasks while allowing stepping errors does not degrade movement quality, but rather promotes adaptive improvements in gait kinematics.
Of particular interest are the increases in joint powers observed following HIT in variable contexts. Gains in gait speed are due in large part to gains in specific joint powers, particularly the ankle plantarflexors to increase propulsion, 52 which may be compensated by increased hip flexor powers to initiate swing in those with neurologic injury. 53 While gains in joint powers are expected with faster speeds, providing HIT in variable contexts allows therapists to strategically target patient-specific biomechanical deficits that may limit locomotor function. Examples of both single-subject and population data are provided in Figure 3 and illustrate the gains in joint powers from the VIVRANT trial. Specifically, Figure 3(A) to (C) demonstrates changes in ankle, knee and hip paretic joint powers in a single individual provided HIT in variable contexts. Average power traces across the gait cycle are labeled to indicate specific portions during which concentric (positive) and eccentric (negative) powers are typically observed for each joint. 54 Specific powers contributing to gains in forward progression include primarily positive powers associated with ankle propulsion (A2) and hip flexion to initiate limb swing (H3) as major contributors to faster higher walking speeds. 53 In addition, increases in knee extensor power (K2) in early/mid-stance are uncommon in individuals without neurologic injury, although this pattern is common in the paretic limb of individuals post-stroke,48,50 and may be a mechanism to raise the center of mass early during stance.
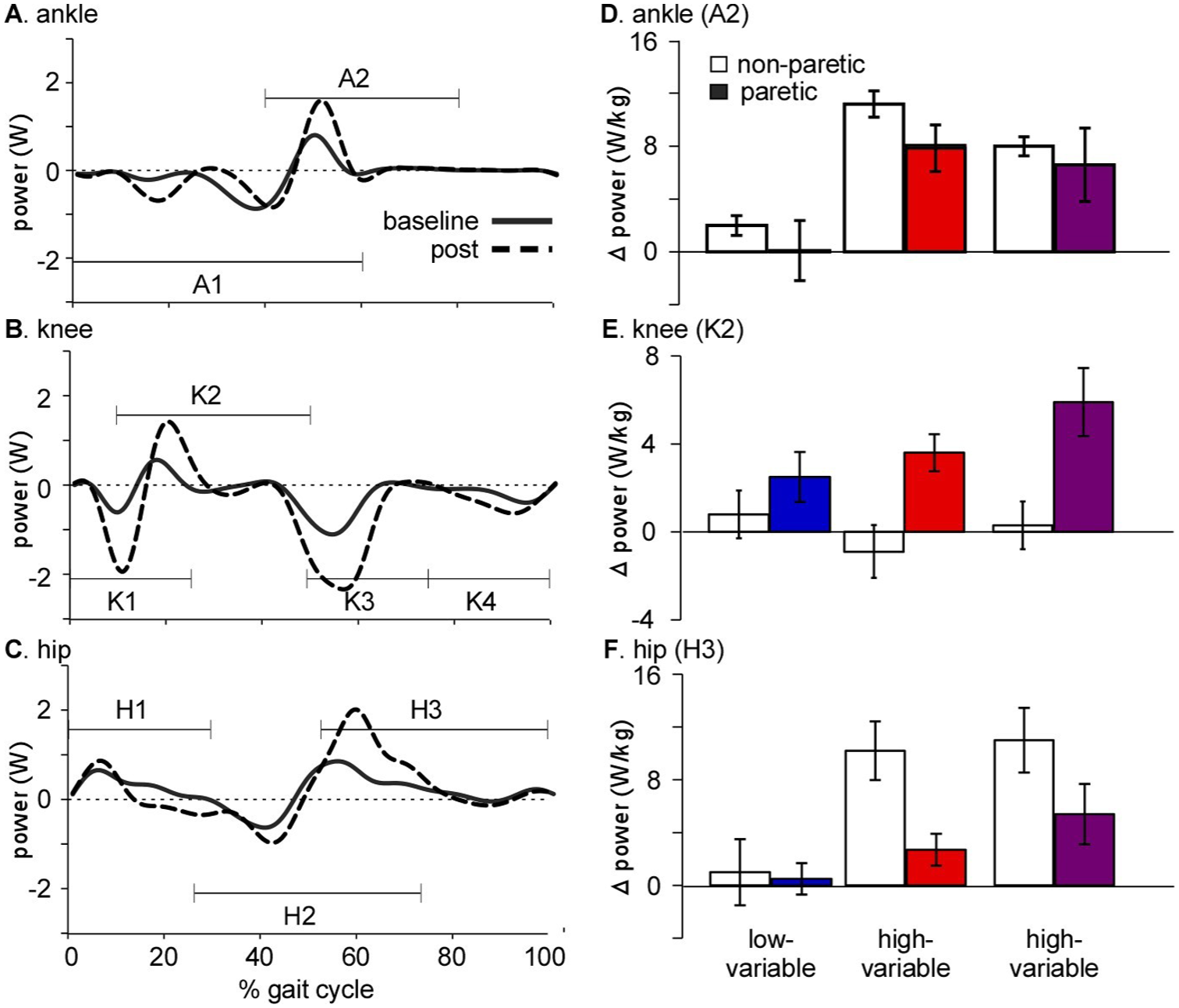
(A-C) Single subject examples of ankle, knee, and hip power prior to and following high-intensity training (HIT) in variable contexts, indicate specific changes typically observed. (D-F) Average changes in powers in each training group in Very Intensive Variable Repeated AmbulatioN Trial indicating gains primarily with HIT, with tendency for larger gains during HIT in variable contexts.
Average changes in both paretic and non-paretic ankle, knee and hip powers are also shown in Figure 3(D) to (F). Specific alterations are identified for area under the major concentric phases described above (A2, K2, and H3), with large significant differences between both HIT groups and low-intensity training consistent with differences in gait speed. 48 While differences between HIT in variable contexts vs forward walking were not significant, principal component analyses indicated a tendency of greater paretic hip and ankle powers with HIT in variable contexts, while HIT forward tended to rely on both paretic (K2 and H3) and non-paretic propulsive (A2) powers. Slightly greater gains in paretic joint power with HIT in variable contexts suggest the potential utility of targeting specific biomechanical deficits during walking, although more directed strategies towards the more impaired limb may be needed to elicit larger gains in neurologic recovery vs compensation, but are difficult with current clinical tools.
Use of Technology to Improve Delivery of Locomotor Training
Technological advances over the past 25 years have generated substantial enthusiasm regarding how locomotor interventions might be enhanced to maximize patient outcomes. 55 Robotic locomotor devices, in particular, offered early promise of improving locomotor outcomes, especially in those with severe locomotor dysfunction in whom physical assistance can be limited by the labor-intensive demands of manually guided stepping practice. 56 In addition, these devices could theoretically improve delivery of locomotor interventions in individuals with less severe impairments. 57 Namely, programmable robots should be able to manipulate training demands through application of precisely timed forces that can assist, resist, or perturb the limbs to address an individual’s biomechanical deficits. In principle, these devices could serve as ideal platforms for implementing shaping during varied walking tasks, as they might precisely and repeatedly modulate task difficulty based on performance in ways that may be challenging for therapists.
Despite this promise, however, most rehabilitation robotic devices utilized clinically do not possess the flexibility to modulate forces at different joints to challenge many of the biomechanical subcomponents of walking during variable walking tasks. Rather, most continue to focus on providing assistance for limb swing and stance, consistent with weight-supported treadmill training described previously. Initial clinical devices in the early 2000s include the Lokomat (Hocoma), an exoskeletal device assisting hip and knee movement over a motorized treadmill with an overhead harness support, 56 or the GaitTrainer (Rehab Technology) which provided elliptical assistance from bilateral footplates to guide the limbs during swing and stance. 58 Both devices deliver substantial stepping practice while reducing therapist burden, although evidence supporting their clinical efficacy has been mixed. Some studies, particularly those employing elliptical training in individuals early post-stroke, reported modest advantages compared with conventional therapy.59,60 However, many other studies demonstrated little to no additional benefit,61-63 and in some cases, inferior outcomes relative to alternative interventions.30,64-66 Recent development of overground exoskeletal devices held similar promise, although these devices also restrict movement substantially, with recent results also indicating limited efficacy.67-69 Many of these devices have developed resistance algorithms for increasing task demands during walking, but are typically limited to swing-phase resistance, and there are no studies to suggest this alteration elicits greater gains in locomotor function. From a shaping perspective, the lack of positive findings of these devices are unsurprising, as providing assistance for swing and stance may not sufficiently challenge the participant and offers minimal progression. Rather, since resistance can be provided only for swing deficits, other subcomponents could be targeted. For those with substantial locomotor deficits early following injury, providing guidance may be helpful (Figure 1(A)), although continued assistance and limited flexibility would, in turn, limit volitional patient engagement70,71 and decrease task demands of stepping.72,73 Accordingly, utilization of these devices appears to follow Figure 1(B) with protracted assistance beyond what may be necessary, with very little emphasis on progressing task difficulty using shaping principles.
Alternative strategies to whole limb robotic systems include programmable modular devices that can be utilized at different joints to facilitate or resist joint excursion, and provide a potential solution for directly addressing specific biomechanical deficits. Two well-tested systems both address unilateral ankle deficits, including the Robotic Exosuit Augmented Locomotion (REAL) 74 and the Assisted Mobility and Balance for the Lower Extremity (AMBLE).75-77 The REAL system, for example, facilitates ankle propulsion in late stance to complement plantarflexion power generated by the user. In a number of smaller trials,78-80 assisted plantarflexion propulsion combined with walking training at varying cardiovascular intensities elicits gains in walking function, although results have yet to be confirmed in a larger trial. Separately, the AMBLE device provides assistance-as-needed for dorsiflexion during swing phase to minimize foot drop/inversion and retrain individuals to volitionally increase dorsiflexor activation. Use of this device has been found to elicit gains in walking speed and dorsiflexion control in smaller trials with individuals post-stroke. While both may be promising, the extent to which they elicit volitional engagement depends critically on their control system and the degree to which they allow voluntary movement. Devices such as REAL and AMBLE, which are designed to support user-generated motion and provide assistance only as needed, can facilitate motor relearning. In contrast, assisted devices that deliver more continuous or less responsive assistance risk dampening volitional effort, as observed for whole limb robotic devices. 72
Conversely, a potential strategy for enhancing ankle function involves applying forces that resist plantarflexion to target propulsion, and has been attempted by both devices. In 1 study using the REAL system, the direction of forces applied was altered from plantarflexion assistance to resistance, and tested on 9 individuals post-stroke. 81 Individuals were assessed without and with different levels of resistance, with assessments immediately following removal of resistance to observe potential changes in power following brief exposure. Single-day results indicate modest changes in propulsion forces with removal of resistance (0.33%-1.49% body weight) dependent on the magnitude of forces applied. These promising results indicate a latent reserve of plantarflexion power that can be harnessed with appropriately timed delivery of resistive forces.
To more extensively examine the potential of resistance-based training to implement shaping principles, the AMBLE device was modified to apply plantarflexion resistance during late stance. In a preliminary case series, 3 ambulatory individuals >6 months post-stroke completed up to 30 sessions of HIT targeting >70% heart rate reserve with progressively increased plantarflexion resistance and visual feedback of propulsive forces. Single-step catch trials without resistance were used throughout training to monitor volitional plantarflexion power, and resistance was upregulated when catch-step propulsive powers increased to ~170% of initial values, indicating a substantial latent reserve that could be accessed with progressive resistance. Examples of changes in propulsive powers observed during catch trials over the course over training are shown for 2 participants (Figure 4(A) and (B)). For the first individual (Figure 4(A)), average propulsive power during catch trials was low over the initial sessions and gradually increased across training, with some variability. For the second individual who typically wore an ankle-foot orthosis in the community, Figure 4(B) shows almost no plantarflexion power during catch trials at the first session, with marked improvements over subsequent sessions. Together, the provision of augmented visual feedback of propulsive powers and systematic progression of resistance based on catch-trial performance reflect the performance-based progression of task difficulty central to shaping principles, and illustrate how this technique may influence locomotor performance over time.
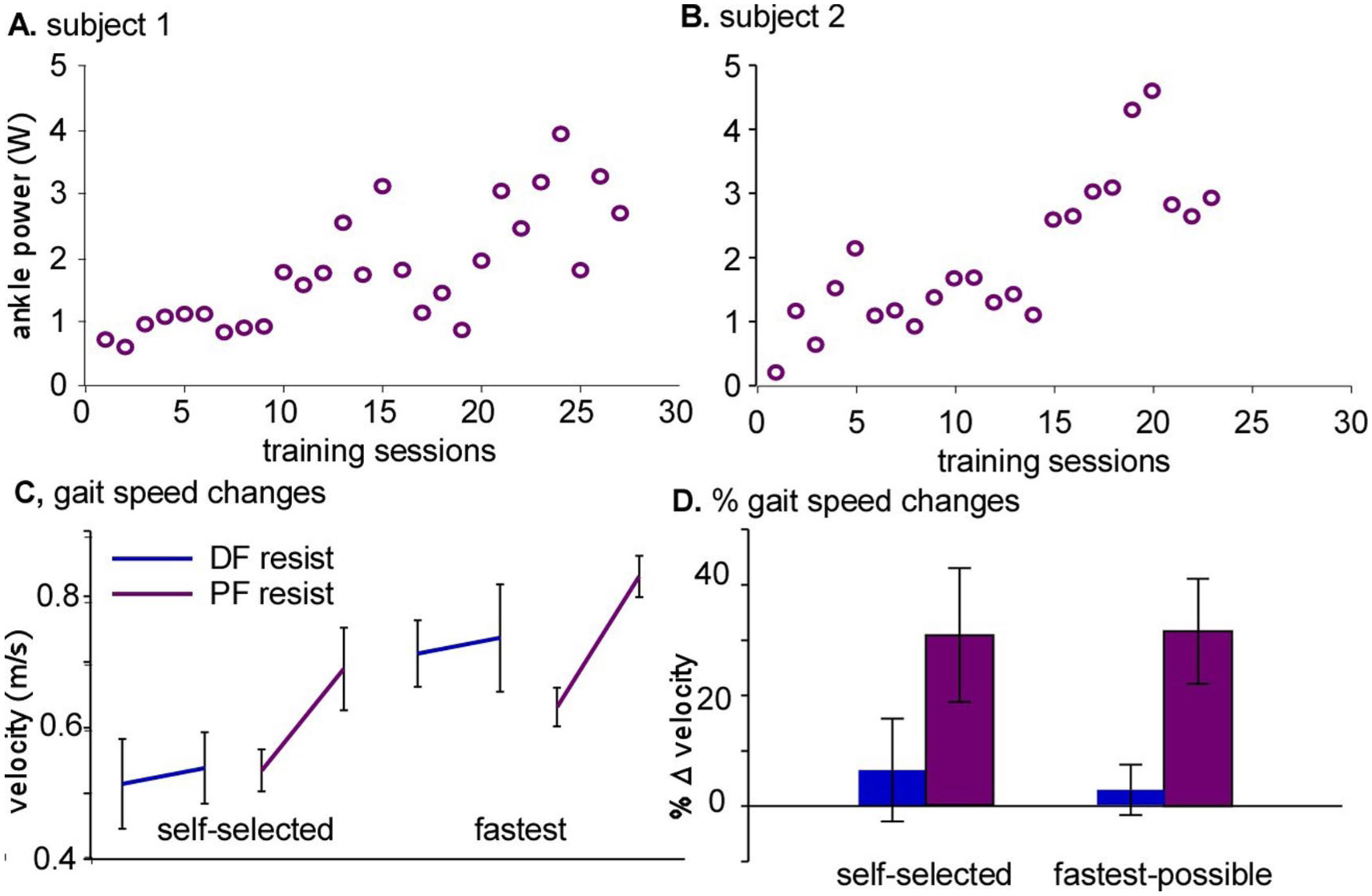
(A and B) Two single-subject examples of ankle powers during catch trials applied each session during robotic-resistance training applied with the Assisted Mobility and Balance for the Lower Extremity-high-intensity training device. (C and D) Average changes in gait speeds at self-selected and fastest pace prior to and following dorsiflexion assistance, and subsequently with plantarflexion resistance.
To further contextualize the gains observed with this approach, all 3 participants who received plantarflexion-resisted HIT had previously completed up to 18 sessions of lower-intensity stepping training with dorsiflexion assistance using the original AMBLE device at least 1 year previously. Changes in self-selected and fastest-possible gait speeds for each subject are presented in Figure 4(C) to (D) for both dorsiflexion assistance and plantarflexion resistance, indicating substantially larger gains with resistance vs assistance training. Although it is difficult to disentangle the specific contributions of plantarflexion resistance versus HIT intensity, the resistance protocol was also associated with marked increases in paretic plantarflexor power and improved propulsive symmetry. These findings suggest that targeting propulsion as a specific biomechanical deficit during training may elicit greater improvement in plantarflexor power and symmetry that can support enhanced locomotor function.
Summary/Conclusions
This review delineates the use of shaping techniques during locomotor training in individuals with locomotor dysfunction, and the detailed differences in how this concept is applied during HIT versus more traditional interventions, which likely contribute to differences in locomotor outcomes. Using primarily clinical strategies, substantial gains in locomotor and non-locomotor tasks have been demonstrated, including gains in community mobility in selected trials that are not observed with many rehabilitation strategies. Technological advances in the use of robotic rehabilitation devices were also discussed, with an emphasis on the potential for greater improvements in rehabilitation outcomes when targeting specific biomechanical deficits underlying locomotor dysfunction.
Footnotes
Author Contributions
Kelly P. Westlake: Data curation; Investigation; Methodology; Project administration; Supervision; Writing—original draft; Writing—review & editing. Katherine Dudek: Data curation; Methodology; Writing—original draft; Writing—review & editing. Anindo Roy: Funding acquisition; Investigation; Methodology; Writing—original draft; Writing—review & editing. Christopher E. Henderson: Conceptualization; Writing—original draft; Writing—review & editing. T. George Hornby: Conceptualization; Project administration; Writing—original draft; Writing—review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data from this study was funded in part by NIH/NICHD – 1R01HD108622, NIH/NICHD – 1R01NS11800, Indiana Brain and Spinal Cord Injury Research Foundation, and NIA Claude D. Pepper Older Americans Independence Center P30-AG028747.
Declaration of Conflicting Interest
Dr. Hornby is co-owns and Dr. Henderson is partially employed by the Institute of Knowledge Translation. Dr. Roy owns and Drs. Westlake and Hornby and Ms Dudek work directly with NextStep Robotics, Inc.