
Abstract
Background:
Children with cerebral palsy (CP) have impaired motor and simplified neuromuscular control during walking. Surgical interventions, conventional therapies, and real-time biofeedback result in minimal improvements in muscle synergies, highlighting the need for new strategies to enhance motor control.
Objective:
To assess how neuromuscular control of the more-affected limb is acutely affected across walking environments and speeds for children with CP.
Method:
Eight children with CP (5 males and 3 females; age: 12.58 ± 3.91 years; height: 1.52 ± 0.20 m; and weight: 54.55 ± 30.83 kg) and 15 typically developing children had 8 surface EMG sensors on the lower limbs. Muscle synergies were calculated with non-negative matrix factorization to define dynamic motor control during walking (walk-DMC) for overground, conventional treadmill, and aquatic treadmill walking. We compared walk-DMC across environment and speed conditions (slow, normal, and fast) for the more-affected limb.
Results:
Main effects of the aquatic environment and the slow walking speed acutely increased walk-DMC in children with CP, indicating increased neuromuscular complexity. Neither conventional treadmill nor overground environments significantly impacted walk-DMC scores.
Conclusions:
Walk-DMC was sensitive to acute changes in the walking environment and speed in children with CP. These findings offer new perspectives on walking rehabilitation by accounting for the interplay between task demands and motor function. However, future studies should investigate repeated exposures to aquatic gait rehabilitation environments, particularly aquatic treadmill training and slow walking speeds.
Introduction
Children with cerebral palsy (CP) sustain a brain injury that affects their dynamic motor control,1-4 which is one’s ability to voluntarily activate muscle groups in a selected pattern without obligatory contractions of other muscles.5,6 Surface electromyography (EMG) can quantify dynamic motor control to determine muscle synergies during walking. Prior literature investigating overground and treadmill walking in children with CP shows reduced muscular synergies2-4,7 compared to typically developing children, indicating simplified neuromuscular control. Furthermore, interventions like botulinum toxin type A injections, selective dorsal rhizotomy, single-event multi-level orthopedic surgery, and conservative treatments (ie, physical therapy) have shown minimal alterations to the number of muscle synergies following treatment.3,8 Similarly, real-time biofeedback training targeting step length, knee extension, and ankle power yielded only slight changes in total variance accounted for (VAF) by the first synergy (baseline walking: VAF = 0.75 ± 0.08; step length: VAF = 0.76 ± 0.05; knee extension: VAF = 0.74 ± 0.07; ankle power: VAF = 0.76 ± 0.05). 9 These findings suggest that current interventions have a limited impact on improving selective motor control. Therefore, there is a critical need to develop and identify interventions that more effectively challenge and enhance motor control in children with CP.
The dynamic motor control index during walking (walk-DMC) can be used to quantify dynamic motor complexity.2-4 The walk-DMC method combines clinical and control values into a single metric, where each 10-point deviation corresponds to 1 standard deviation. Walk-DMC values below 100 indicate simplified neuromuscular complexity, whereas values at or above 100 indicate comparable neuromuscular complexity to typically developing values. Prior literature has used walk-DMC to quantify neuromuscular complexity across different populations, such as children with CP,2-4,6,10 individuals with traumatic brain injuries, 11 and individuals with knee osteoarthritis 12 ; all presenting simplified complexity.
Partial body weight supported gait training has previously been shown to improve walking speed, endurance, and function in children with CP. 13 Aquatic treadmill walking offers a unique form of partial body weight support, allowing individuals to practice gait in a reduced-gravity environment. Because walk-DMC reflects neuromuscular control during walking, assessing it in an aquatic environment could reveal how body weight support and hydrodynamic drag influence motor control strategies in children with CP. Despite previous investigations in CP indicating reduced walk-DMC values during overground and treadmill gait, a knowledge gap remains for walk-DMC modulation in partial body weight supported gait at different walking speeds.13-15 Therefore, we suspect long-term exposure to varied walking contexts will promote alternative neuromuscular control strategies by initially simplifying motor control and progressively expanding degrees of freedom as individuals become more familiar with these walking contexts. However, we also anticipate that even with an acute visit, an initial response to these varied walking contexts could be observed, providing meaningful insight for changes in neuromuscular complexity driven by environmental and speed variations. This process could be summarized through changes in walk-DMC values, which provide insights into neuromuscular adaptation. In addition, providing within-subject reference values amongst varied walking conditions will facilitate the planning of future studies and clinical trials using the walk-DMC metric.
The primary aim of this study was to assess how neuromuscular control is acutely affected for the more affected limb across different walking environments and speeds in children with CP. We hypothesized that the walk-DMC index would be lower in the aquatic environment than in the overground and conventional treadmill environments due to partial body weight support. We further hypothesize that faster walking speeds would increase, and slower speeds would decrease walk-DMC values as suggested by previous literature. 2 Finally, we hypothesize that there will be an interaction effect between environment and walking speeds, with slow walking in the aquatic environment having the lowest walk-DMC values due to buoyancy and hydrodynamic effects. We intend to provide needed information for designing and optimizing walking rehabilitation strategies for children with CP by quantifying the effects of varying contexts on walk-DMC values.
Methods
Participants
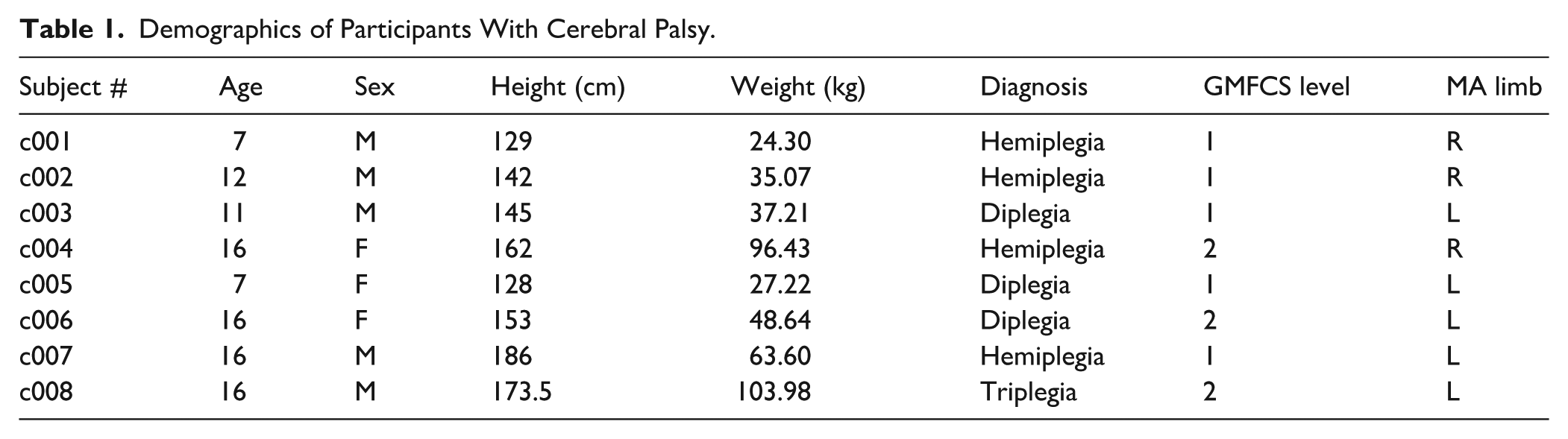
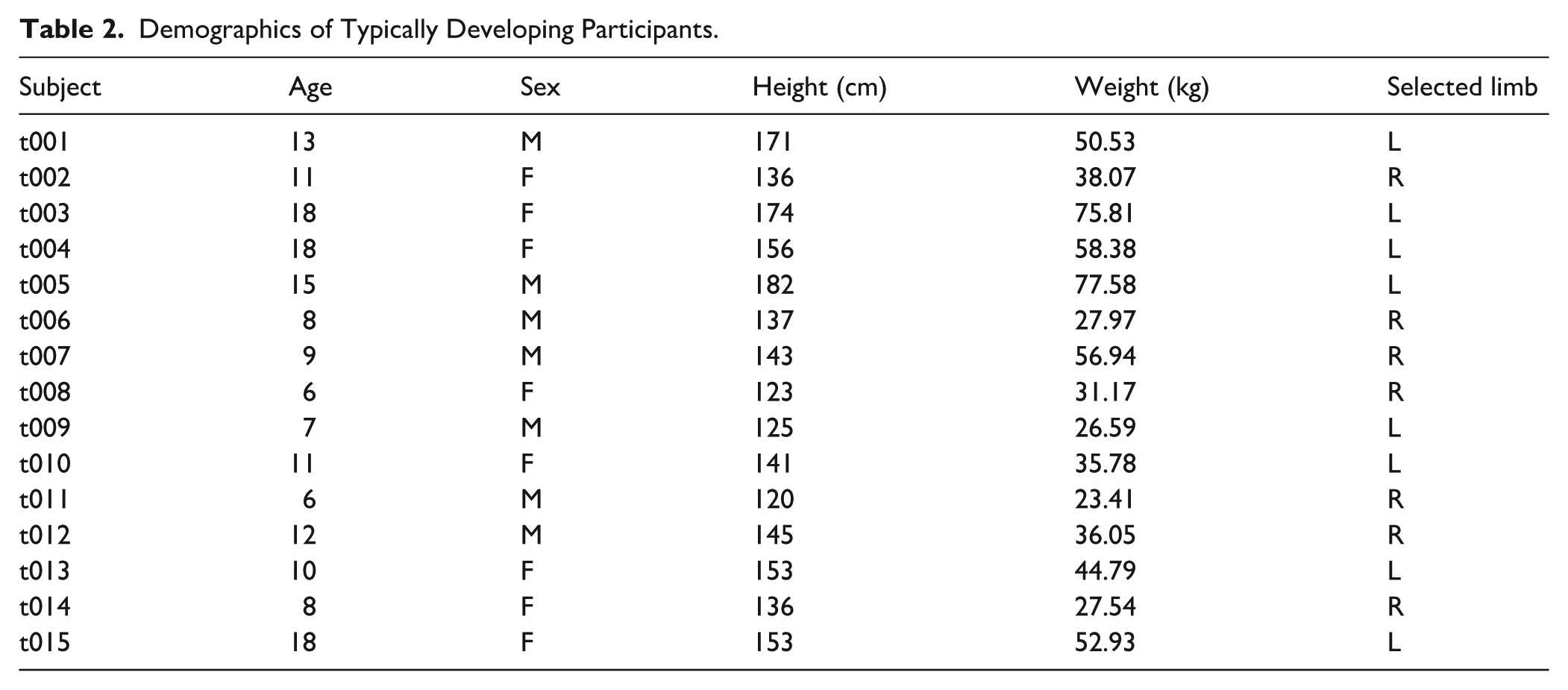
Eight children with CP (Table 1; 5 males and 3 females; age: 12.58 ± 3.91 years; height: 1.52 ± 0.20 m; and weight: 54.55 ± 30.83 kg) and 15 typically developing children (Table 2; 7 males, 8 females; age: 11.30 ± 4.10 years; height: 1.46 ± 0.18 m; and weight: 44.20 ± 16.80 kg) 16 participated in this study. The sample size was determined based on recruitment feasibility, with a post hoc power analysis conducted to confirm adequate statistical power. Children with CP were included if they were 6 to 18 years old, presented with a fixed knee flexion deformity exceeding 10°, and were types I to III on the Gross Motor Function Classification System (GMFCS). Children with CP were excluded from participating if they were outside the enrollment ages and GMFCS levels, received botulinum toxin type A injections within the past 4 months, and could not independently ambulate with or without assistive devices. Typically developing participants were included in the study if they were 6 to 18 years old and had no self-reported pain or lower limb injuries requiring hospitalization within the past year. Typically developing participants were excluded from participating if they had any musculoskeletal injury that impaired their walking or a medical history of lower limb injury or deformity requiring surgical correction. Participants and guardians reviewed and signed the informed consent approved by the University of Nebraska Medical Center’s Institutional Review Board (IRB# 0196-21-EP).
Demographics of Participants With Cerebral Palsy.
Demographics of Typically Developing Participants.
Research Design
This study was a prospective, block-randomized, cross-over design. Participants performed walking trials in 3 environments: conventional treadmill (DRY), overground (OG), and aquatic treadmill (WET). Within the DRY and WET environments, participants performed 3-minute walking trials at 3 randomized speeds: slow (75% self-selected), normal (100% self-selected), and fast (125% self-selected). For the OG environment, participants walked along a 10 m pathway at self-selected slow, normal, and fast speeds in a randomized order, completing each speed at least 3 times. The determination of treadmill self-selected walking speed and complete walking details is outlined in prior work. 16
Electromyography
Participants were instrumented bilaterally with waterproof wireless surface EMG equipment 16 (Mini Wave Infinity Waterproof, Cometa, Milan, IT; input impedance = 20 MΩ, common mode rejection ratio = 120 dB) with pre-gelled bipolar Ag/AgCl electrodes (Coviden disposable sEMG electrodes, Coviden, Dublin, IE; dimensions: 30x24 mm; inter-electrode spacing: 2.5 cm) following SENIAM guidelines. 17 Electrodes were placed after shaving and cleaning the skin with alcohol. Bilateral muscle activity of the tibialis anterior, medial gastrocnemius, rectus femoris, and semitendinosus were sampled at 2000 Hz, bandpass filtered between 20 and 500 Hz, mean-centered, full wave rectified, and then low-passed filtered at 10 Hz with a fourth order Butterworth filter following prior literature.2,3,18,19 EMG data for each muscle were then normalized by the absolute peak of the entire trial for each muscle separately, with amplitude ranging from 0 to 1. EMG data was then segmented into strides, as determined from the left and right detected events from inertial measurement units (WaveTrack Waterproof, Cometa, Milan, IT; full-scale acc sensitivity = ±8 g; full-scale gyroscope sensitivity = 1000 dps; dimensions: 36 mm × 25 mm × 10 mm). IMUs were located on the midsection of the metatarsals of the feet with the X-axis aligned and oriented proximally toward the ankle, and detected events were used to time-normalize EMG data to 101 points representing the gait cycle. Five consecutive strides, or the maximal number of available strides for each condition (Tables 3 and 4), were concatenated from the middle 80% of all available trials. The middle 80% of each trial was used to avoid acceleration and deceleration periods and to maintain consistency with prior walk-DMC studies.8,18-20 For the DRY and WET environments, 5 consecutive strides were selected from the middle of the 3-minute trails to represent steady-state walking. For the OG environment, the trial containing the greatest number of consecutive strides was selected. Limiting all conditions to 5 strides (or the maximal available) ensured comparable synergy calculations across environments, as the inclusion of larger numbers of strides can influence synergy outcomes. 18 A random side was chosen to determine the muscle synergies for typically developing children aligning with prior literature,2,3,8,18,19 whereas the more affected limb was selected for the CP children.2,3,8 In children with diplegic CP, the more affected limb was determined following data collection by comparing Gait Deviation Index 21 (GDI) scores for the left and right limbs; the limb with the lower GDI score was designated as more affected.
Typically Developing Children’s Mean and Standard Deviation (SD) of Walking Velocity (m/s) and Variance Accounted for by the First Synergy (VAF1) Across Conditions.
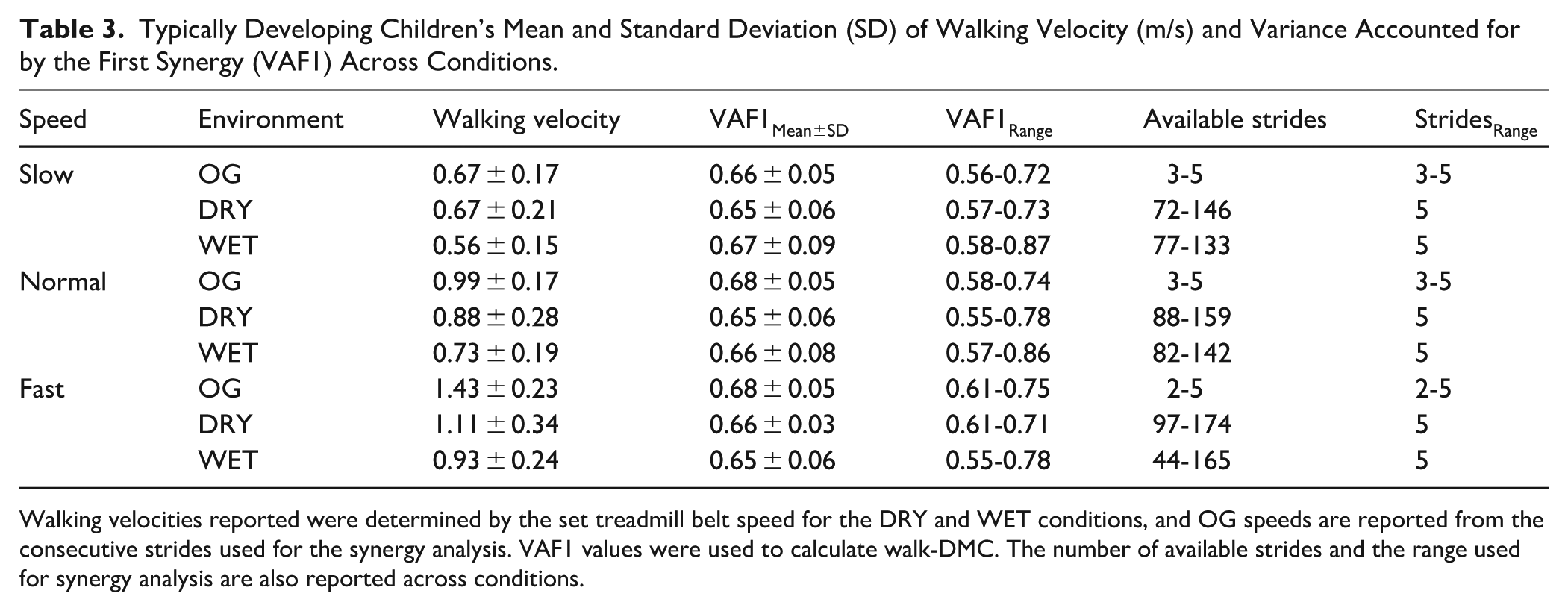
Walking velocities reported were determined by the set treadmill belt speed for the DRY and WET conditions, and OG speeds are reported from the consecutive strides used for the synergy analysis. VAF1 values were used to calculate walk-DMC. The number of available strides and the range used for synergy analysis are also reported across conditions.
Children With Cerebral Palsy’s Mean and Standard Deviation (SD) of Walking Velocity (m/s) and Range of Variance Accounted for by the First Synergy (VAF1) Across Conditions for the More-affected Limb.
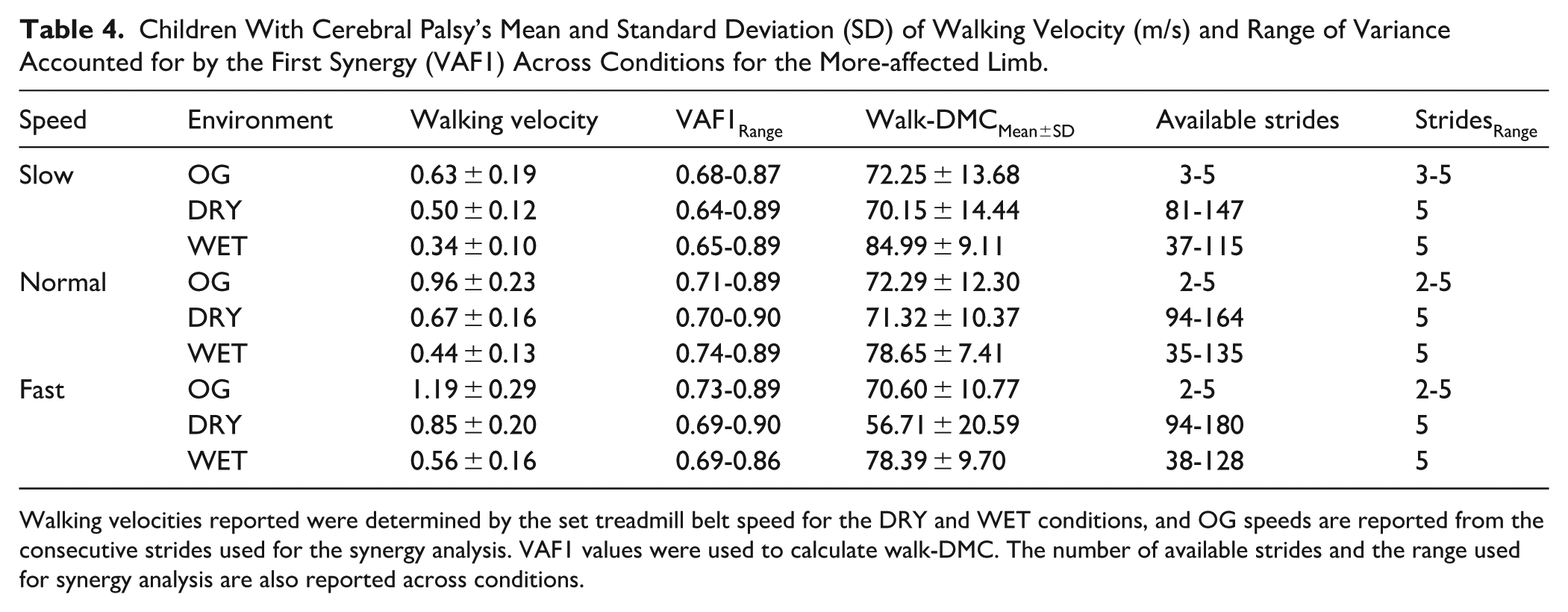
Walking velocities reported were determined by the set treadmill belt speed for the DRY and WET conditions, and OG speeds are reported from the consecutive strides used for the synergy analysis. VAF1 values were used to calculate walk-DMC. The number of available strides and the range used for synergy analysis are also reported across conditions.
Synergy Calculation
For each participant, muscle synergies were calculated using MATLAB’s non-negative matrix factorization (NNMF) function with the following parameters from prior literature2-4,10,11,19: alternating least squares algorithm, 50 replicates, 1,000 maximum iterations, 1 x 10-4 minimum threshold for convergence, and 1 × 10−6 threshold for completion (Figure 1(a)). Non-negative matrix factorization produces synergy weights (W) and synergy activations (C). W is a matrix defined by the number of muscles (

where VAF is calculated as 1 minus the ratio of the sum of square errors and the total sum of squares of the EMG data calculated across the gait cycle (Figure 1(b)).
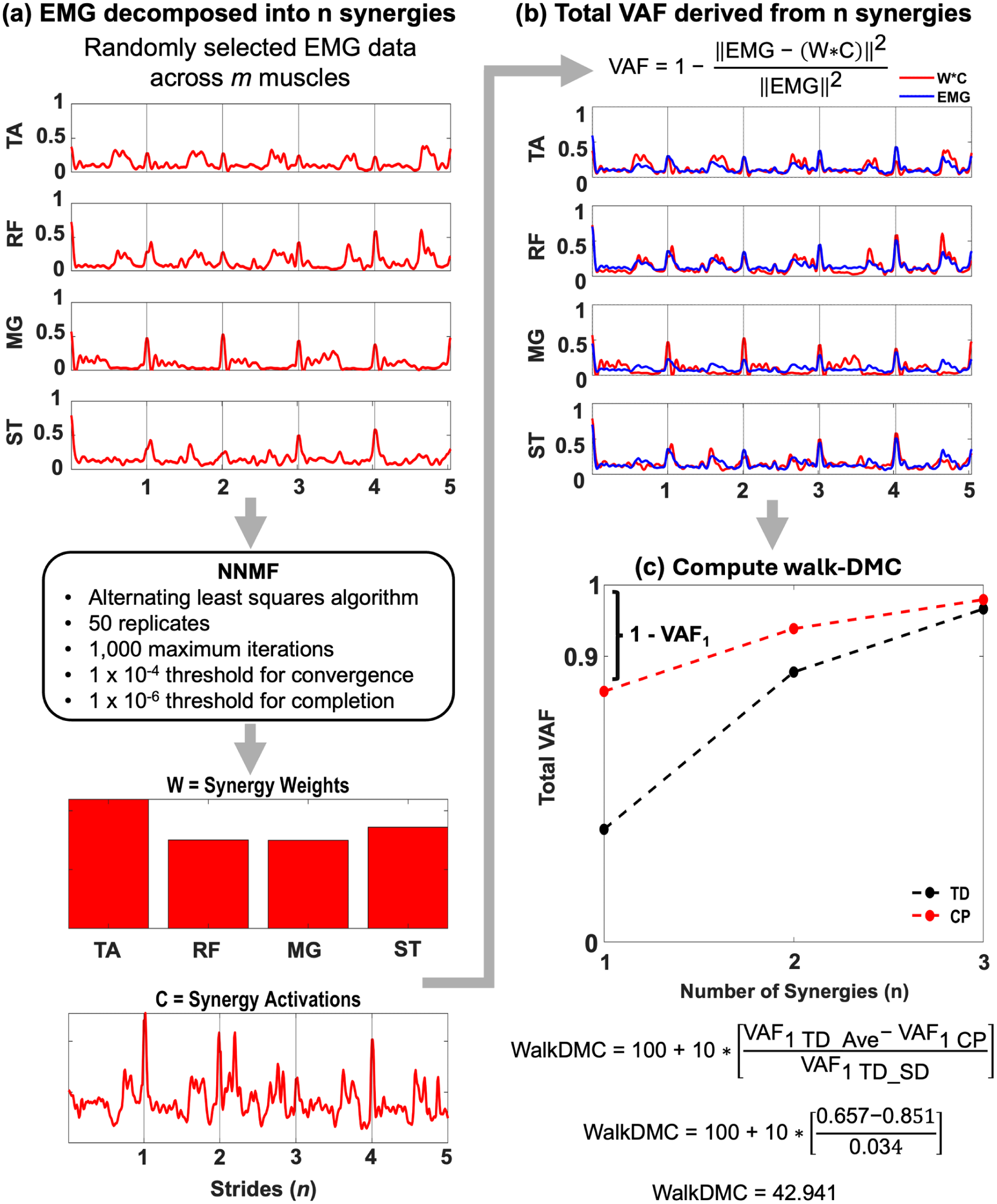
An example of the dynamic motor control index during walking (walk-DMC) calculation for a child with cerebral palsy during the conventional treadmill (DRY) fast speed condition. (a) Five consecutive strides were concatenated (red waveform) for each muscle group (TA is tibialis anterior; RF is rectus femoris; MG is medial gastrocnemius; and ST is semitendinosus) and were placed into a 4 × 505 matrix for non-negative matrix factorization (NNMF). NNMF calculated n synergies (W) and the activation of those synergies (C) over the gait cycle. (b) The variance accounted for (VAF) was calculated using 1 minus the ratio of the sum of square errors and the total sum of squares of the EMG data across 505 points of the gait cycle. In this example, 1 synergy accounted for about 85.1% of the variance in muscle activity for 4 sites. (c) With the first synergy, we calculated the walk-DMC from the total VAF of 1 synergy as a z-score compared with the mean (0.657) and standard deviation (0.034) of the typically developing children.
Walk-DMC
Walk-DMC measured muscle activity complexity across each environment and walking speed for the more affected limb as a z-score (equation (2)) 2 :

where VAF1 CP is the first synergy (n = 1; Table 3) for a CP child, VAF1 TD_Ave and VAF1 TD_SD are the mean and standard deviation of typically developing VAF values for the randomly selected limb during the first synergy (n = 1; Table 4). Walk-DMC scores were scaled such that typically developing children’s average was 100 and a 10-point increment is 1 standard deviation. 2 This scaling has been previously used in CP literature with the Gait Deviation Index and Gait Variability Index,21,22 and it assists in comparing literature and clinician interpretation.
Statistical Analysis
Statistical tests were performed using R (RStudio 2023, PBC, Boston, MA, US). Linear mixed-effects analyses were used to evaluate walk-DMC values across 3 levels of environment and walking speed for the more-affected limb. Fixed effects were environment and speed with random effects for individual differences. To assess the magnitude of differences between the main and interaction effects of the linear mixed-effects model, we calculated partial eta-squared (ηp 2 ) effect sizes with .01 being small, .06 being medium, and .14 or more being large effects. 23 Post hoc pairwise comparisons with Tukey’s Honest Significant Difference corrections were used to correct for multiple comparisons. The calculated differences between the pairwise comparisons will be reported as the estimate (E), with the variability reported as the standard error. To assess the magnitude of the differences between groups, we calculated Cohen’s d (d) as the effect size for the pairwise comparisons, with 0.20 as a small effect, 0.50 as a medium effect, and 0.80 as a large effect. 23 The 95% confidence interval (CI) is reported for both partial eta-squared and Cohen’s d effect sizes. The a priori significance level was set at α = .05 and was adjusted for post hoc pairwise comparisons accordingly. A post hoc power analysis was conducted to confirm that the final sample size provided sufficient power (β > .80) to detect statistically significant effects.
Results
All children in both the typically developing and CP cohorts completed each condition, and walk-DMC values for the more-affected limb were available for each CP child across all conditions. A linear mixed-effects model was fit using the restricted maximum likelihood to investigate the effects of environment (OG, DRY, WET) and walking speed (slow, normal, fast) on walk-DMC values of the more affected limb, with random intercepts and slopes by subjects. The mean and standard deviations of walk-DMC across all environments and speeds are reported in Table 3 and Figure 2. A main effect of environment was significant (F(2,56) = 17.26, P < .001, ηp 2 = .38, 95% CI [0.18, 0.53]), indicating a large effect of environment on walk-DMC. A main effect of speed was also significant (F(2,56) = 4.54, P = .014, ηp 2 = .14, 95% CI [0.01, 0.30], indicating a large effect of speed on walk-DMC.
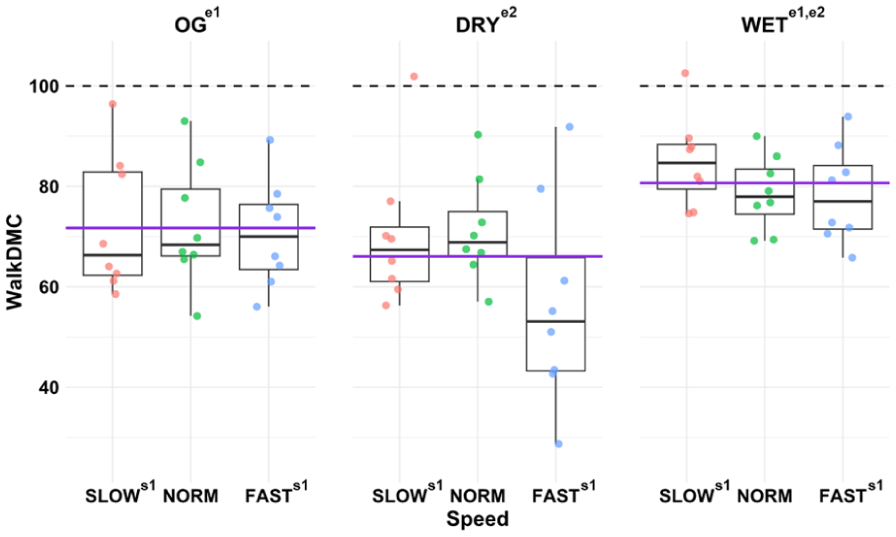
Walk-DMC scores across each environment and speed. Each panel represents the environment. Each colored dot represents a child with CP. The solid purple line within each panel represents the group mean. The black dashed line at 100 represents the typically developing values of this study. Values lower than 100 represent a simplified muscle activation pattern during gait. Values over 100 represent a more complex muscle activation pattern during gait. Superscripts that share values indicate pairwise differences (P < .05) with letters ‘s’ and ‘e’ indicating comparisons within the main effects for speed and environment.
For the large effect of environment, it was observed that the WET environment had a significantly higher walk-DMC score when compared to the OG environment (E = 8.96, ES = 2.51, t(56) = 3.57, P = .002, d = 1.03, 95% CI [0.353, 1.709]) and the DRY environment (E = 14.62, ES = 2.51, t(56) = 5.83, P < .001, d = 1.68, 95% CI [0.95, 2.41]). However, there were no significant differences in walk-DMC between the OG and DRY environments (P = .071).
For the large effect of speed, it was observed that walk-DMC was increased during slow walking speeds when compared to fast walking speeds (E = 7.23, ES = 2.51, t(56) = 2.88, P = .015, d = 0.83, 95% CI [0.17, 1.50]). There were no significant differences in walk-DMC when comparing normal to fast walking speeds (P = .080) or normal to slow walking speeds (P = .775).
To evaluate the consistency of the muscle synergy analysis across stride counts, analyses were performed using multiple iterations of 5 strides across all conditions, along with additional analyses including 15, 25, and 35 strides for the DRY and WET conditions (Supplemental Tables 1 and 2). Across both typically developing and CP groups, the variance accounted for by the first synergy (VAF1) remained consistent across stride conditions.
Discussion
The current study examined the effects of environment and walking speed on walk-DMC values of the more affected limb in children with CP. We found main effects of environment and speed, indicating that the walking paradigm in children with CP acutely impacts neuromuscular control of walking. Previous literature described that previous interventions targeting musculoskeletal and neuromuscular systems have minimal effects on the underlying neuromuscular strategies during walking, suggesting fixed motor control strategies.3,9 While these interventions induce changes in movement, they may not evoke changes in motor control.3,9 To alter motor control, interventions must actively stimulate and challenge the neural system, such as exposure to novel walking settings. 4 Our study demonstrated that acute changes in walk-DMC occur during aquatic treadmill walking and slow walking speeds.
There were no significant differences in walk-DMC between the OG and DRY environments, suggesting that these modes of walking do not impose additional neuromuscular demands that influence walk-DMC. However, walk-DMC values were significantly higher in the WET environment, likely due to the water’s resistance and buoyancy 24 acting on the lower limbs. These factors may have increased neuromuscular complexity by placing greater demands on muscle groups while enhancing stability through partial body weight support. This acute change in neuromuscular control may reflect mechanisms similar to those observed in previous aquatic therapy literature, which has been shown to improve motor control in children with CP.14,15 The buoyancy of the aquatic environment reduces effective body weight of the child, which may increase the degrees of freedom available to the lower limbs. This reduction in load to the lower limbs may allow for greater movement exploration, and consequently, support the development of motor control during the WET condition. However, this interpretation is speculative and warrants further investigation.
Although slower walking speeds increased walk-DMC scores compared to fast, each speed was associated with varying motor control complexity, which may be leveraged for targeted rehabilitation. Prior literature suggests a complex relationship between motor control complexity while walking at slow and fast speeds, with changes in EMG magnitude and activation patterns compared to a normal speed.25,26 We observed no significant differences between normal and slow or fast walking speeds in motor control complexity, suggesting that using normal speeds in walking rehabilitation paradigms may not drive neuromuscular changes. Our findings suggest that slower walking speeds can evoke more complex movement patterns and improve neuromuscular complexity, whereas fast speeds increase variability, potentially reflecting the use of alternative motor strategies that could result in motor control changes. Therefore, future studies are needed to investigate how repeated exposure to slow and fast walking speeds alters motor control and if retention of walking adaptations transfers to alternative environments (ie, overground).
It is important to note that the present study reflects an acute response to each walking environment. While our results provide valuable insights into varied walking contexts, future research should investigate repeated and long-term exposure to each condition, as different walking contexts may lead to alternative changes in motor control. Previous literature on motor learning emphasizes the role of practice and experience in enhancing motor skills, where repeated exposure may reduce compensatory strategies in children with CP.15,27,28 Thus, investigating how walk-DMC changes across each walking context provides information on how motor control can be modulated in ambulatory children with CP. Rehabilitation programs should balance the benefits of the WET environment with the potential motor and cardiovascular challenges posed by slower walking speeds. Therapists may need to adjust the walking speed,29,30 body weight support, and type of walking environment to ensure that children with CP can achieve optimal motor function while balancing the cardiovascular benefits of higher workloads.
Limitations of our study need to be considered when interpreting our results. Our sample size was small, limiting generalizability to the heterogeneity of neurological impairment present in the CP population. Calculating synergies using NNMF is sensitive to the number of muscles included in the analysis, and using fewer muscles increases the estimated total VAF. 18 Although this study only used 4 sites, this is similar to prior work,4,8 and these sites are the most common surface EMG measured in instrumented clinical gait analyses within research and clinical settings. Importantly, supplemental analyses demonstrate that the VAF1 was robust to the number of strides included, with consistent values observed across a range of concatenated strides (5-35), supporting the stability of the reported results despite the limited muscle set (Supplemental Tables 1 and 2). Walking speeds were not standardized across environments, which may have influenced comparisons across conditions. Because speed was not controlled, the independent effects of walking speed and environment cannot be fully disentangled. The observed differences should be interpreted reflecting the combined influence of environment and the self-selected speeds associated with each condition. These differences in walking speed reflect the constraints inherent to each environment. Therefore, the observed changes in walk-DMC represent condition-specific responses occurring at ecologically valid speeds rather than isolated speed effects. The sample included children aged 7 to 16 years, which may have introduced variability in neuromuscular control. Subgroup analyses by age were not performed due to the small sample size, and future studies with larger cohorts are needed to explore age-related effects. Despite these limitations, investigating how consistent practice in varying walking contexts affects learning and retention of motor skills will be crucial for developing effective rehabilitation strategies. 27
This study highlights the complex nature of environment and walking speed on motor control in children with CP. Both slow walking and the WET environment pose unique motor control challenges that may increase neuromuscular complexity. Our results suggest that walking in a WET environment, characterized by slower ecologically valid walking speeds, is associated with increased dynamic motor control in children with CP. However, these findings likely reflect the combined influence of environment and self-selected walking speed. These findings indicate that rehabilitation programs should consider environment and speed to optimize gait training in children with CP. Furthermore, future studies should investigate the potential benefits of repeated exposure to these conditions to neuromuscular complexity and their retention and transferability to alternative walking contexts.
Supplemental Material
sj-docx-1-nnr-10.1177_15459683261454950 – Supplemental material for Walking Environment and Speed Differentially Change More Affected Limb Dynamic Motor Control in Children With Cerebral Palsy
Supplemental material, sj-docx-1-nnr-10.1177_15459683261454950 for Walking Environment and Speed Differentially Change More Affected Limb Dynamic Motor Control in Children With Cerebral Palsy by Stephanie N. Mace, Joseph W. Harrington, Vivek Dutt, Brian A. Knarr and David C. Kingston in Neurorehabilitation and Neural Repair
Footnotes
Ethical Considerations
This study was approved by the Ethics Committee of the University of Nebraska Medical Center’s Institutional Review Board (IRB# 0196-21-EP) on September 29th, 2023. All participants and guardians provided written informed consent prior to enrollment in the study. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Consent to Participate
The study was approved by the University of Nebraska Medical Center’s Institutional Review Board (IRB# 0196-21-EP) on September 29th, 2023. All participants and guardians provided written informed consent prior to participating.
Author Contributions
Stephanie N. Mace: Formal analysis; Investigation; Writing—original draft. Joseph W. Harrington: Investigation; Writing—review & editing. Vivek Dutt: Conceptualization; Funding acquisition; Resources; Writing—review & editing. Brian A. Knarr: Conceptualization; Funding acquisition; Writing—review & editing. David C. Kingston: Conceptualization; Funding acquisition; Supervision; Writing—review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Nebraska Collaboration Initiative Pilot Award (26246) and the National Institutes of Health (1R15HD109666). Equipment for this study was supported by the Center of Research in Human Movement Variability of the University of Nebraska at Omaha and the National Institute of Health (P20GM109090).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplementary Material
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.