
Abstract
Background:
While non-invasive electrical stimulation is used clinically to enhance motor performance, its efficacy and mechanisms remain unclear. Studies show that personal factors, such as beliefs and expectations of stimulation, can impact how much a person benefits from the stimulation itself. Furthermore, beliefs related to the “closeness is strength of effect” have been observed outside of electrical stimulation contexts, suggesting that the location of stimulation (eg, head and neck) for improving motor performance may impact how much they believe the stimulation will work. This exploratory study investigated beliefs about the optimal target region of stimulation for maximizing the effect of stimulation itself.
Methods:
Eighty participants (39 females; 46.9 ± 12.6 years) completed an online spatial mapping task in which they were asked to indicate where they would place the electrodes for electrical stimulation to hypothetically enhance specific functions: “hand movement,” “arm movement,” “leg movement,” and “attention/concentration.” Participants selected their placement by clicking a blank human figure in anatomical position. Information about prior use/knowledge of non-invasive stimulation was also collected.
Results:
Optimal target region of stimulation was significantly associated with the body movement/function to be enhanced (P < .001). This association was independent of prior non-invasive stimulation knowledge (P = .242) and sex (P = .923).
Conclusions:
These findings suggest a pre-existing belief of spatial proximity for electrical stimulation in which placing electrodes closer to the body region of interest would maximize improvement hypothetically.
Introduction
Non-invasive electrical stimulation has been used in experimental and clinical settings (eg, stroke rehabilitation) to enhance motor performance. Transcranial direct current stimulation (tDCS), transcutaneous vagus nerve stimulation (tVNS), and transcutaneous electrical nerve stimulation (TENS) are among the most common modalities due to their ease of use and affordability. However, these techniques have had mixed results for enhancing motor performance.1,2 Recent work has demonstrated that psychological factors like treatment expectation can significantly affect motor outcomes post-stimulation, even in sham-controlled studies, which could contribute to such variability in results.3,4 However, human participants bring a wide range of pre-existing beliefs about a given treatment and knowledge of their bodies. Since people outside of clinical or research fields may have limited knowledge of stimulation modalities and their mechanisms of action, they may instead rely on the “closeness is strength of effect” metaphor,5,6 where the spatial (eg, physical contact or treatment application) proximity is required for an outcome. Under this framework, individuals tend to judge the efficacy of a treatment from the spatial proximity of the cause (ie, the treatment) relative to the effect (ie, the specific improvement).5,7
Given that different stimulation modalities with different stimulation locations are used in neurorehabilitation to improve a given motor function, such as the spatial proximity between the stimulation site and the targeted region of improvement needs to be considered. For example, to improve hand function post-stroke, electrodes would be placed on the scalp for tDCS, near the ear or on the neck for tVNS, and on the arm close to the hand for TENS. However, based on the above framework, people may perceive the electrode location physically closer to the hand as a more optimal location than further away (ie, the head). This exploratory study investigated beliefs about the optimal target region of stimulation for maximizing the hypothetical effect of stimulation itself.
Methods
Eighty participants completed an Arizona State University Institutional Review Board-approved online study on Qualtrics. Participant demographics are reported in Table 1. A spatial mapping task was employed in which participants were asked where they would approximately place the electrodes of an electrical stimulator to enhance each of the following functions: hand movement, arm movement, leg movement, and attention/concentration. Participants indicated their optimal electrode placement for each function via a mouse click on a blank human figure; mouse click locations were considered during analysis as head, neck, torso/back, arm, hand, leg, feet, or other (Figure 1(A)). By asking participants to identify the optimal placement, our task served as a behavioral proxy for existing beliefs about potential treatment effectiveness. These locations were considered as physical evidence of the “closeness is strength” association, where the optimal target region for stimulation is determined by the spatial proximity to the specific body function. Mouse-clicks were collapsed across hemispheres for analysis and visualization (Figure 1(B)). Participants’ prior knowledge of electrical stimulation was recorded; no medical history or information was collected.
Demographic Characteristics of Participants (n = 80).
Data are presented as mean ± standard deviation and n (%).
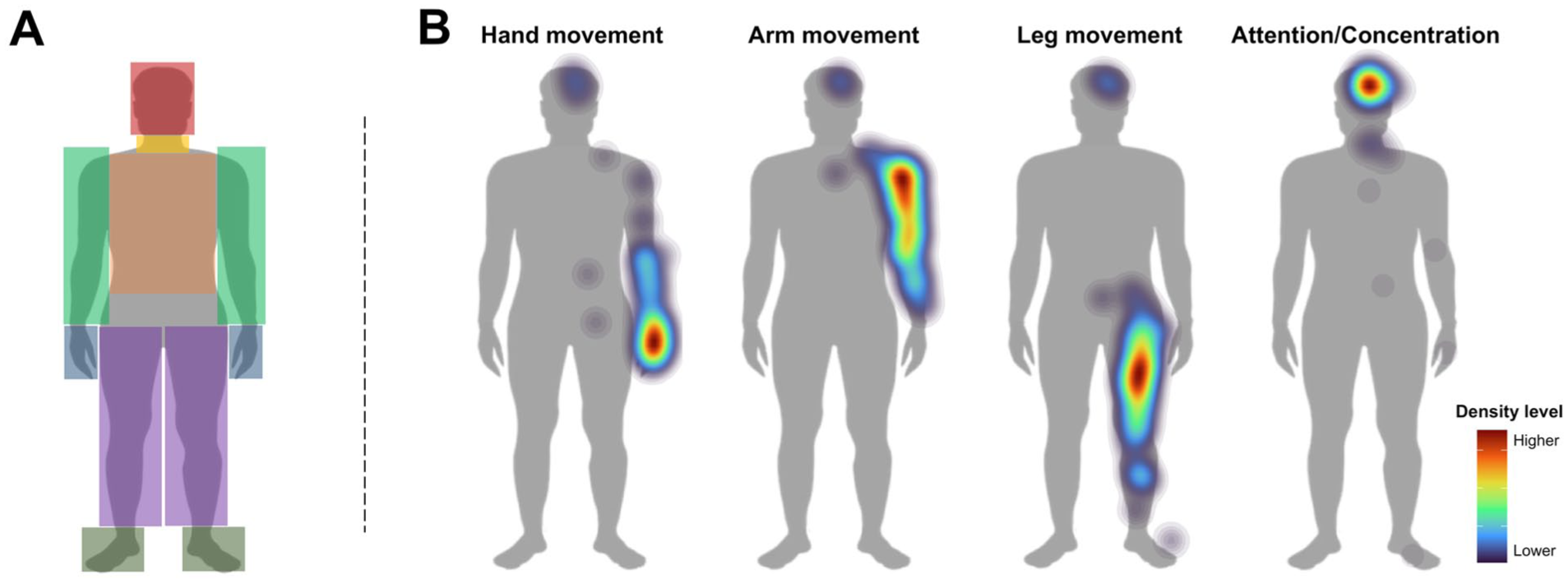
(A) Human figure in anatomical position with overlay-colored areas that represented the defined target regions used for the analysis. Participants indicated their optimal electrode placement for each function by clicking on a blank human figure (without the colored areas shown) with their mouse or cursor. Click locations were categorized into the following areas: head (red), neck (yellow), torso/back (brown), arm (light green), hand (blue), leg (purple), feet (dark green), or other (gray). (B) Density maps illustrating the participant’s selected optimal target anatomical region for enhancing each specific function in the blank anatomical human figure. The density level, indicated by color intensity (ie, hotter colors), denotes the concentration of participants’ clicks. Any responses indicated on the left side of the body (36% of the total responses) were superimposed on the corresponding location on the right side for data visualization and analysis.
Fisher’s exact tests with Monte Carlo simulations were used to evaluate the association between selected target regions and body functions. Separately, the target regions selected were compared by sex and prior knowledge with Fisher’s exact tests. Chi-square tests were performed to assess potential differences in match rates, anatomically aligned responses (eg, “Leg” for Leg Movement), across the functions. More details on the study’s protocol and statistical analysis are provided in the Supplemental Material.
Results
Results showed a significant association between the perceived optimal target region of stimulation and the body function to be enhanced (Fisher’s exact test with Monte Carlo simulation, P < .001). Responses did not depend on prior electrical stimulation knowledge (Fisher’s exact test, P = .242) nor participant sex (Fisher’s exact test, P = .923). Matches between the perceived optimal target region of stimulation and the body function in question were common: >87% for both the arm and the leg for enhancing arm and leg movement, respectively. Furthermore, 83% selected the head for attention/concentration. While 47.5% selected the hand for enhancing hand movement, 35% selected the arm, and 7.5% chose the head as a relevant region for stimulation. When comparing the proportion of matches across the 4 functions, there was significantly higher mismatching when selecting the body region for enhancing hand movement compared to the other 3 functions (χ² > 21.721, df = 1, P < .001). However, there were no significant differences in body regions selected for the other functions (χ² < 0.877, df = 1, P > .349).
Discussion
This study showed that, overall, people matched the perceived optimal target region of stimulation to the body function to be enhanced. Although beliefs about the optimal stimulation location did not depend on prior knowledge of electrical stimulation, the general awareness of stimulation tended to be low (11.5% in this study and 18.7% in prior work 8 ). However, we cannot rule out that the lack of differences regarding prior knowledge may be influenced by the unbalanced subgroup sizes. It remains possible that extensive knowledge or experience could modulate this spatial proximity association, 5 which should be explored further in populations with greater knowledge or exposure to stimulation (eg, those with spinal cord stimulators). Nevertheless, it is plausible these beliefs about where stimulation would be most effective for a given function likely contribute to (or interact with) the perception of treatment efficacy, independent of any information provided by the clinician or experimenter. 9
Regarding limitations, this study did not directly compare different stimulation modalities, as these interventions typically involve interactions among verbal information, physical sensations, and technical parameters. However, by isolating these pre-existing beliefs here, we can demonstrate the potential implications of these phenomena when stimulation is applied to certain regions. It is therefore plausible that applying stimulation closer to (or on) the perceived optimal target region for a given function may be perceived as more relevant or effective than distal applications (eg, TENS on the arm vs tDCS on the scalp for enhancing hand movement). Further, while this pilot study focused on non-invasive stimulation modalities, these results may also apply to other physical manipulations. Finally, since participants’ neurological status (eg, stroke and spinal cord injury) was not collected, it is unclear how pre-existing beliefs about the optimal stimulation sites persist or change following neurological impairment. Future research should consider the extent to which this phenomenon varies across clinical and non-clinical cohorts. Additionally, future studies will also explore how these pre-existing beliefs influence and interact with treatment expectation, a premise supported by evidence of site-specific placebo effects in which responses occur only in the treated body region and not beyond. 10 We encourage future clinical trials to evaluate and, when feasible, control for participants’ pre-existing beliefs regarding spatial proximity and treatment expectations regarding electrical stimulation to better attribute any observed benefits (or lack thereof) to the appropriate mechanisms.
Supplemental Material
sj-docx-1-nnr-10.1177_15459683261456659 – Supplemental material for “Where Would You Stimulate?” Beliefs About Anatomical Relevance for Enhancing Motor Performance With Non-Invasive Electrical Stimulation
Supplemental material, sj-docx-1-nnr-10.1177_15459683261456659 for “Where Would You Stimulate?” Beliefs About Anatomical Relevance for Enhancing Motor Performance With Non-Invasive Electrical Stimulation by Bernardo Villa-Sánchez, Andrew Hooyman, Seth A. Hays and Sydney Y. Schaefer in Neurorehabilitation and Neural Repair
Footnotes
Author Contributions
Bernardo Villa-Sánchez: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Visualization; Writing—original draft; and Writing—review & editing. Andrew Hooyman: Methodology and Writing—review & editing. Seth A. Hays: Methodology and Writing—review & editing. Sydney Y. Schaefer: Conceptualization; Funding acquisition; Methodology; Supervision; and Writing—review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partly funded by the School of Biological and Health Systems Engineering at Arizona State University (discretionary funding to S.Y.S.).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplementary Material
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.