
Abstract
Effective treatment options for steroid-refractory acute graft-versus-host disease (SR-aGVHD) remain limited. Mesenchymal stromal cells (MSCs) offer a promising therapeutic approach, but the optimal administration protocol is undefined. This retrospective cohort study investigated the impact of MSC infusion frequency on outcomes in patients with grade III–IV SR-aGVHD who received umbilical cord-derived MSCs either once weekly (n = 25) or three times weekly (n = 18). The primary endpoints were overall response rate (ORR) and complete response (CR) at 28 days, and secondary endpoints included overall survival (OS) and changes in lymphocyte subsets. The thrice-weekly group demonstrated significantly superior ORR (77.8% vs. 48.0%, P < 0.05) and CR rates (55.6% vs. 20.0%, P < 0.05), with a particularly notable benefit in gastrointestinal aGVHD (ORR: 73.3% vs. 35.0%, P < 0.05). Immunological analysis showed a more rapid and profound decline in CD3+CD8+ T cells in the thrice-weekly group (nadir: 21.16% vs. 52.09%, P < 0.05; time to nadir: 10 vs. 21 days, P < 0.05). With a median follow-up of 423 days, the thrice-weekly regimen was associated with significantly improved 2-year OS (78.1% vs. 47.4%, P < 0.05). Despite the limitations of a retrospective design, these findings suggest that increased MSC infusion frequency might be associated with improved therapeutic efficacy and survival in severe SR-aGVHD. However, the potential confounding effect of cumulative dose cannot be excluded, and these results warrant validation in prospective randomized trials.
Keywords
Introduction
Acute graft-versus-host disease (aGVHD) is a major complication and a significant cause of nonrelapse mortality following allogeneic hematopoietic stem cell transplantation (HSCT). 1 Currently, there are no effective treatments for severe GVHD, with corticosteroids as first-line therapy achieving a response rate of only approximately 50%.2,3 Among patients with severe GVHD who develop steroid-refractory GVHD (SR-GVHD), second-line agents remain ineffective in 17%–70% of cases.4,5 Consequently, the management of severe GVHD remains a challenging aspect of allogeneic HSCT.
Mesenchymal stromal cells (MSCs) are adherent, fibroblast-like cells characterized by their self-renewal capacity and potential to differentiate into multiple mesenchymal lineages. 6 As a primary third-line therapeutic option, the use of MSCs continues to attract clinical interest. Since the initial report by Le Blanc et al. describing complete remission of steroid-resistant acute GVHD in a pediatric patient treated with MSC infusions, 7 numerous studies have investigated the potential benefits of MSCs in severe acute GVHD.8–14 However, the optimal timing and frequency of MSC administration, as well as the immunological mechanisms underlying their effects in severe GVHD, remain to be fully elucidated.
Previous studies have explored patient selection for MSC therapy, including its use in multidrug-resistant (MDR) GVHD following haploidentical stem cell transplantation. 11 MDR-GVHD is defined as GVHD that fails to respond to at least two prior lines of treatment. These studies enrolled patients whose acute GVHD either progressed within 1 week or showed no response (NR) by 2 weeks after initiating second-line therapies. 11 When human umbilical cord blood-derived MSCs (UC-MSCs) were administered at a dose of (1.0–2.0) × 106/kg once weekly, the overall response rate (ORR) was only 57.1%. Other researchers have reported that MSC infusion—whether administered before or after transplantation—may reduce the incidence of chronic GVHD but does not appear to prevent acute GVHD or control its progression.15–17
Notably, all aforementioned studies employed a once-weekly MSC administration regimen. Basic research has shown that acute GVHD is associated with a significant reduction in MSC numbers, which can occur even before clinical manifestation of the disease. 18 Additionally, the inhibitory effect of MSCs on T cell proliferation is dose-dependent, with increasing suppression observed at MSC-to-T cell ratios ranging from 1:0.2 up to 1:5—the point of maximal inhibitory effect. 18
Therefore, it remains unclear whether increasing the frequency of MSC infusions—and thereby the cumulative cell dose—can effectively control the progression of severe acute GVHD. In this retrospective study, we aimed to evaluate the effects of two different infusion frequencies—once weekly versus three times per week—in patients with severe GVHD.
The primary objectives of this study were to compare the therapeutic efficacy of these two infusion regimens and to analyze the immune mechanisms involved in MSC treatment of severe GVHD, with particular focus on T lymphocyte subsets (CD3+CD8+, CD3+CD4+, and regulatory T cells).
Methods
Patients
From January 2018 to December 2023, 43 patients who received MSCs after allogeneic HSCT, including 15 patients with acute leukemia, 18 patients with severe aplastic anemia (SAA), and 10 patients with other types of diseases, were included in this study.
In the early stage, MSCs are used once a week for severe GVHD patients. In the later stage, from September 2021, MSCs were gradually used three times a week for the treatment of aGVHD patients.
The inclusion criteria of patients treated with MSCs were as follows:
Grade III to IV aGVHD patients (GVHD organ: gastrointestinal [GI] tract; skin; liver); aGVHD progressed within 1 week after first-line and second-line drug therapies.
Transplantation
At the time of diagnosis, before beginning transplantation, human leukocyte antigen (HLA) typing and donor-specific antibody (DSA) detection were performed to identify a suitable donor from among family members. If patients did not have an HLA-matched sibling donor (MSD), an HLA-matched unrelated donor or HLA-haploidentical donor (HID) was selected after informed consent was received from the patients and their families.19,20
The conditioning regimen consisted of the following:
Acute myeloid leukemia (FA + Bu/Cy): 30 mg/m2/day fludarabine every 3 days, 2 g/m2/day cytarabine every 3 days, 3.2 mg/kg/day Bu every 3 days, and 60 mg/kg/day cyclophosphamide every 2 days. Acute lymphoblastic leukemia (total body irradiation (TBI) + Flu/Bu): 5–8 Gy TBI, 30 mg/m2/day flu every 3 days, and 3.2 mg/kg/day Bu every 3 days. SAA (FC/antithymocyte globulin [ATG]): 30 mg/m2/day fludarabine every 4 days, 30 mg/kg/day cyclophosphamide every 4 days, and 2.5 mg/kg/day ATG every 4 days. Bucy conditioning regimen: 3.2 mg/kg/day Bu every 3 days and 60 mg/kg/day cyclophosphamide every 3 days.
The recipients of haploidentical HSCT and HLA-matched unrelated HSCT also received ATG (2.5 mg/kg/day IV, days −5 to −2). The source of hematopoietic stem cells was bone marrow combined with peripheral blood stem cells. The GVHD prophylaxis program was cyclosporine A + mycophenolate mofetil (MMF) + short-course methotrexate. aGVHD and posttransplant lymphoproliferative disorders were diagnosed and graded according to international criteria.
GVHD
The diagnosis and grading of aGVHD were based on the international consensus criteria.21–23 When aGVHD was identified, corticosteroids and the optimized level of CSA were applied first. If the patients had SR-GVHD, second-line treatments included basiliximab, MMF, tacrolimus, and ruxolitinib. The use of these drugs was mostly based on the competence and experience of each physician.
MSC treatment
The preparation of human UC-MSCs was performed using explant adherent culture in a serum-free system under GMP conditions. After collection, each UC was sterilized, dissected into small tissue blocks, and cultured in 150 cm2 flasks at 37°C and 5% CO2 for primary adherent cell growth. Once cells reached approximately 60%–80% confluence, they were subcultured according to standard operating procedures.
Importantly, each MSC product used for clinical infusion originated from a single UC donor, and all infusions administered to the same patient were derived from that same donor, ensuring donor consistency throughout treatment.
MSCs at passage 2–3 were cryopreserved to create a master cell bank. For each clinical infusion, a vial was thawed, and the cells were expanded once to generate the final product. These freshly harvested MSCs were then washed, quality-tested, and infused within 12 h. Therefore, although the starting material was cryopreserved, patients received freshly prepared MSCs.
Quality control included verification of spindle-shaped morphology, viability ≥90% before infusion, sterility testing, endotoxin <0.5 EU/mL, and phenotype confirmation (CD34+/CD45+ ≤2%; CD90+/CD105+ ≥95%). 24
For adult patients, a fixed dose of 1.0 × 106 MSCs/kg body weight was administered per infusion according to institutional protocol.
The response evaluation of aGVHD
Responses were evaluated every day after the first MSC infusion.2,21,25,26 The definitions of response to GVHD treatment were based on the consensus criteria. The ORR was defined as complete response (CR) plus partial response (PR). CR was defined as the complete resolution of acute GVHD manifestations in all organs, without need for secondary GVHD therapy. PR was defined as improvement in GVHD stage in all initially affected organs, without resolution in all organs, worsening in any other GVHD target organs, or need for secondary GVHD therapy.
NR was defined as the same severity of GVHD in any organ or death or the addition of secondary GVHD therapy before day 28. Patients who experienced a flare of acute GVHD before day 28 and required therapy with increased steroids or additional GVHD therapy were also considered to have NR. Progression was defined as worsening GVHD in at least one organ with or without improvement in any other organ. NR and progression were classified as ineffective treatment for aGVHD.20–22
Flow cytometric analysis of the lymphocyte subset
PBMCs were isolated from patients using Ficoll–Hypaque density-gradient centrifugation, enabling batching of tests to minimize interassay variation. Patient blood samples in the two groups were collected once a week before and after the occurrence of aGVHD. T lymphocyte subsets (CD3+, CD3+CD4+, CD3+CD8+, CD4+CD25+Foxp3+) in peripheral blood were analyzed by flow cytometry. To determine the Treg phenotype, we used the intracellular FoxP3 Treg kit and CD4 and CD25 fluorescent antibodies. All analyses used a FACSCalibur flow cytometer and CellQuest Pro™ software. We analyzed the change in T cells before (day 0) and after (1 week to 8 weeks) MSC infusion by flow cytometry. Two indicators were applied to monitor the effect of different MSC regimens in 8 weeks on the lymphocyte subset: the median value of increase or decrease and the median time of increase or decrease to the highest or lowest point.27–30
Statistical analysis
Categorical variables were compared using Fisher’s exact test, and continuous variables were compared using the Mann−Whitney U test. Student’s t-test was used for two-sample comparisons. OS was calculated using the Kaplan−Meier method and compared using the log-rank test. Survival time was calculated from the day of allogeneic stem cell transplantation until death or last follow-up. All statistical analyses were performed using SPSS version 13.0 and the R software package (version 3.6.2; http://www.r-project.org). In addition, multivariate regression analyses were performed to adjust for potential confounding. Penalized multivariate logistic regression (Firth correction) was used to identify independent predictors of day 28 ORR, including MSC infusion frequency, GI involvement, GVHD grade, and patient age. A Cox proportional hazards model was used for OS using the same covariates, except that GI involvement was excluded due to complete separation, and donor type was omitted because sparse events produced unstable estimates. Results were reported as odds ratios (ORs) or hazard ratios (HRs) with 95% confidence intervals (CIs), and a two-sided P < 0.05 was considered statistically significant.
Results
Patient characteristics
Overall, the study included 43 grade III–IV aGVHD patients, with a median age of 36 (12–57) years. The median time of aGVHD after transplantation, including HLA-MSD (n = 13) or HLA-HID (n = 30) transplantation, was 46 (range = 11–129) days for all patients. The characteristics of the patients are summarized in Table 1. Twenty-five patients received MSC treatment once a week, and 18 patients received MSC treatment three times a week as the control group.
Baseline Characteristics
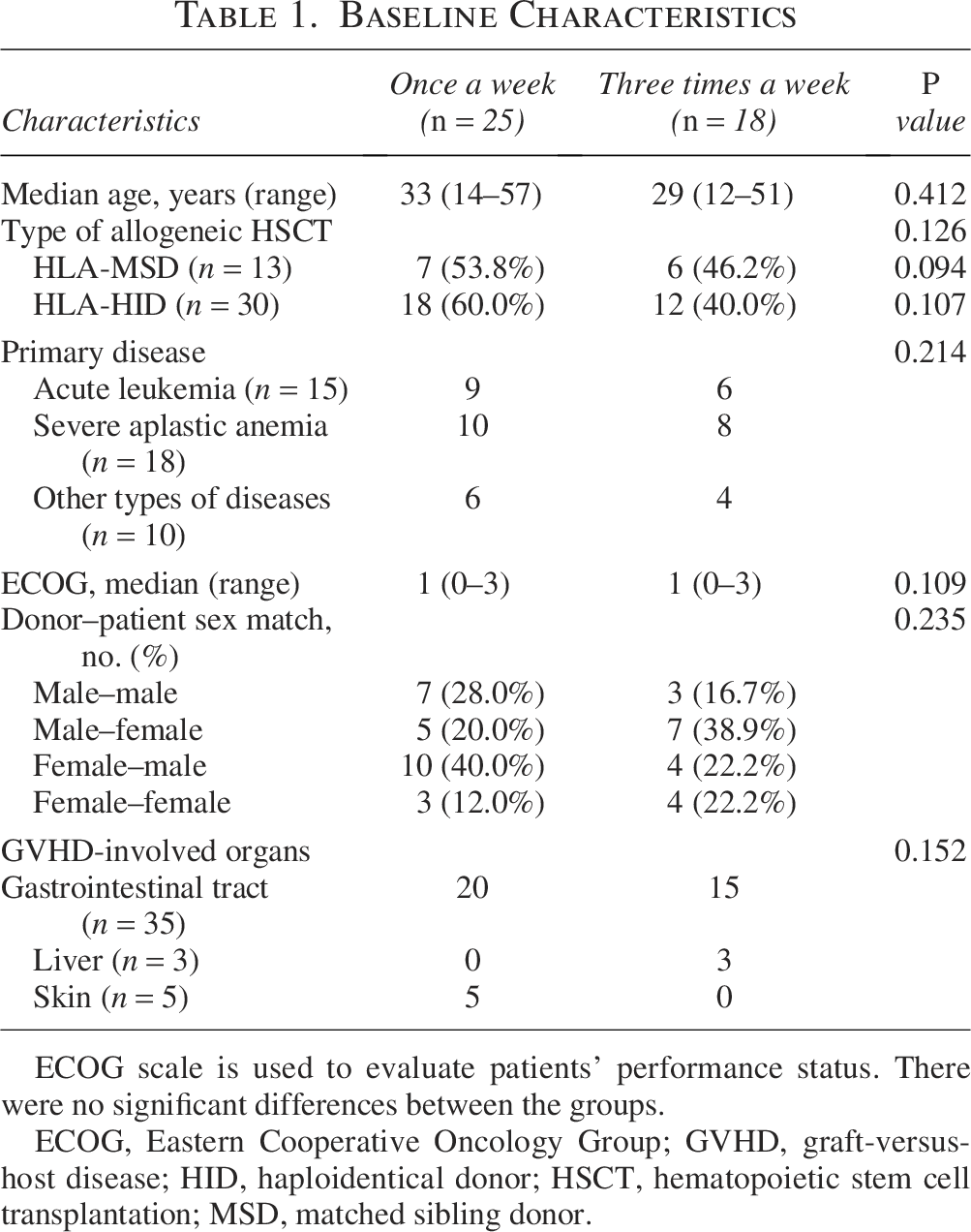
ECOG scale is used to evaluate patients’ performance status. There were no significant differences between the groups.
ECOG, Eastern Cooperative Oncology Group; GVHD, graft-versus-host disease; HID, haploidentical donor; HSCT, hematopoietic stem cell transplantation; MSD, matched sibling donor.
Treatments of aGVHD before MSC treatment
All patients received methylprednisolone combined with calcineurin inhibitors as first-line treatments and basiliximab, MMF, tacrolimus, and ruxolitinib as second-line immunosuppressants for aGVHD. In the two groups, aGVHD progressed within 1 week after first-line and second-line drug therapies. At the onset of MSC treatment, all 43 patients included 35 patients with GI tract GVHD (combined with skin and liver GVHD), 5 patients with isolated skin GVHD, and 3 patients with isolated liver GVHD (Table 2).
Characteristics of Acute Graft-Versus-Host Disease and Responses to Mesenchymal Stromal Cell Treatment
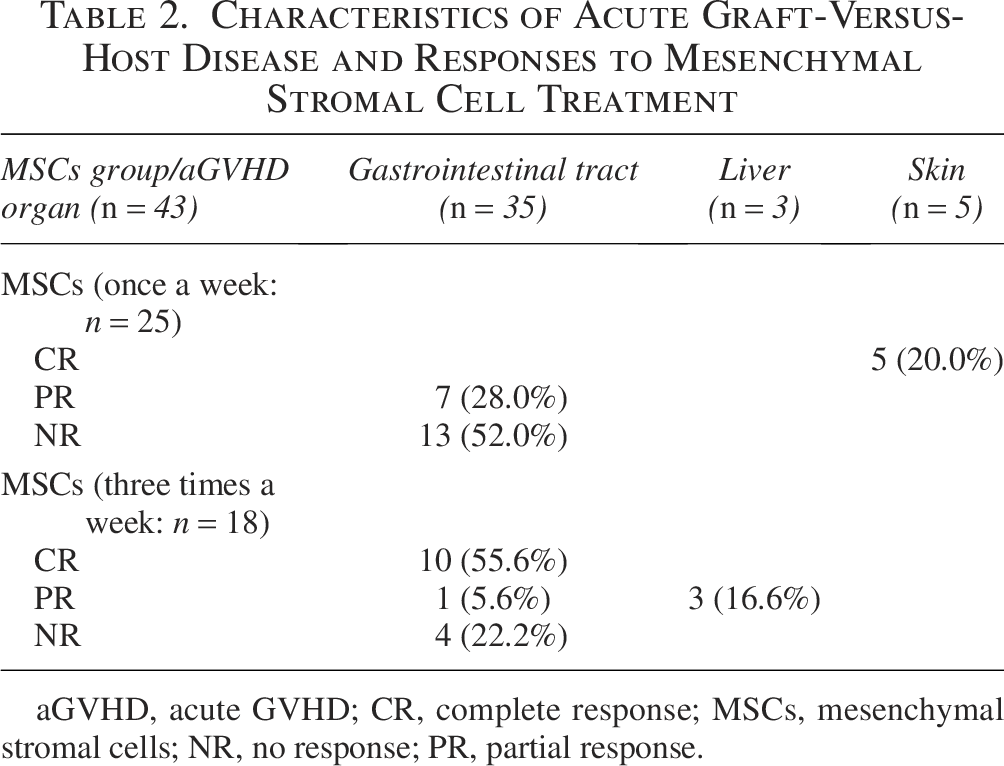
aGVHD, acute GVHD; CR, complete response; MSCs, mesenchymal stromal cells; NR, no response; PR, partial response.
No statistical significance was found between the two MSC groups for the onset grade of aGVHD and preexisting second-line immunosuppressant treatments.
Response to MSC treatment
In the once-weekly group, MSC infusions were administered on consecutive weeks, with most patients completing three to six weekly doses. In the three-times-weekly group, infusions were delivered three times per week on consecutive treatment weeks, typically over 2–3 weeks, unless temporarily delayed due to clinical contraindications (e.g., fever or instability).
In the MSC treatment group, 113 doses of MSCs were administered once a week.
In 25 aGVHD patients, with a median of 4 doses (range = 3–6) per patient, 12 of 25 patients receiving MSCs had an ORR of 48.0% (12/25), including CR in 5 patients (20.0%) and PR in 7 patients (28.0%). Five patients with CR had grade III aGVHD of isolated skin, and seven patients with PR included four grade III aGVHDs of the GI tract (with skin and liver GVHD; Fig. 1).
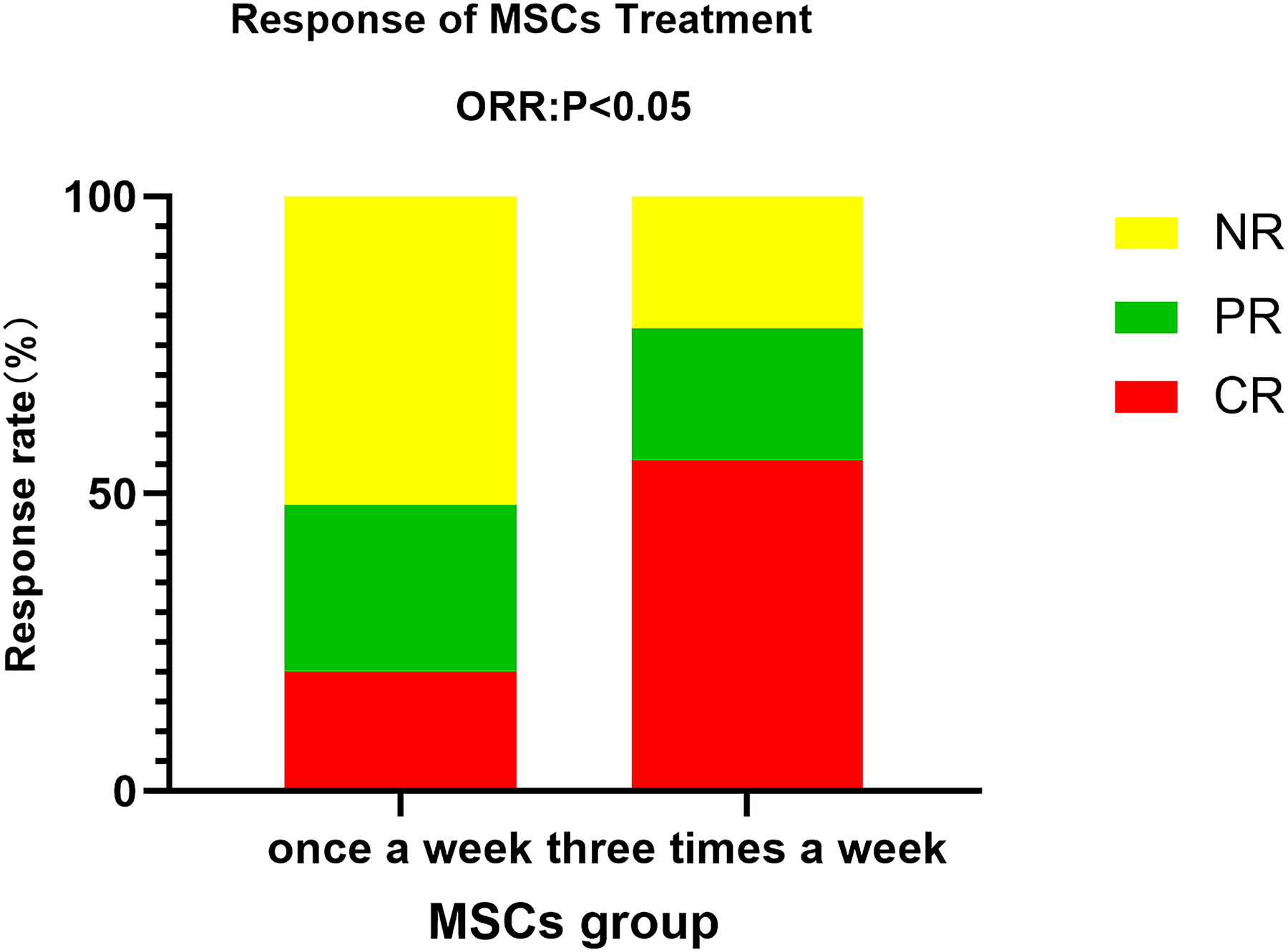
Response rates in aGVHD patients after MSCs treatment. Patients were grouped by once a week (n = 25) or three times a week (n = 18). aGVHD, acute graft-versus-host disease; CR, complete response; MSC, mesenchymal stromal cell; NR: no response; PR, partial response.
Thirteen patients showed NR or progression after weekly MSC therapy.
All 13 patients had grade III–IV aGVHD of the GI tract, including 5 patients with grade III aGVHD of the skin and 2 patients with grade III aGVHD of the liver.
In the MSC treatment group, 121 doses of MSCs were administered three times a week to 18 aGVHD patients, with a median of 7 doses (range = 5–9) per patient. Fourteen of 18 patients receiving MSCs had an ORR of 77.8% (14/18), including CR in 10 patients (55.6%) and PR in 4 patients (22.2%). Ten patients with CR had grade III–IV aGVHD of the GI tract, and four patients with PR included one grade III–IV aGVHD of the GI tract and three grade III aGVHDs of the liver.
Four patients showed NR or progression after 3 weeks of MSC therapy. All four patients had grade IV aGVHD of the GI tract (Table 2).
Comparing the two groups of MSC treatment, the ORR and CR rates in the three-times-a-week MSC group were both significantly higher than those in the once-a-week MSC group (ORR: 77.8% vs. 48.0%, P < 0.05; CR: 55.6% vs. 20.0%, P < 0.05, respectively; Fig. 1).
Comparative efficacy differences in aGVHD of the GI tract
Thirty-five patients with grade III–IV aGVHD of the GI tract had different therapeutic effects in the two MSC treatment groups.
Only 7 of 20 patients (grade III–IV aGVHD of the GI tract) reached PR in the once-a-week MSC treatment group (ORR: 35.0%, 7/20), and the other 13 patients showed NR or progression (NR: 65.0%, 13/20) after weekly MSCs.
In the three-times-a-week MSC treatment group, 10 patients reached CR and 1 patient reached PR among 15 cases of grade III–IV aGVHD with GI (ORR: 73.3%, 11/15).
For patients with grade III–IV aGVHD of the GI tract, the efficacy of the three-times-a-week regimen was significantly higher than that of the once-a-week regimen of MSC therapy (ORR: 73.3% vs. 35.0%, P < 0.05; Fig. 2).
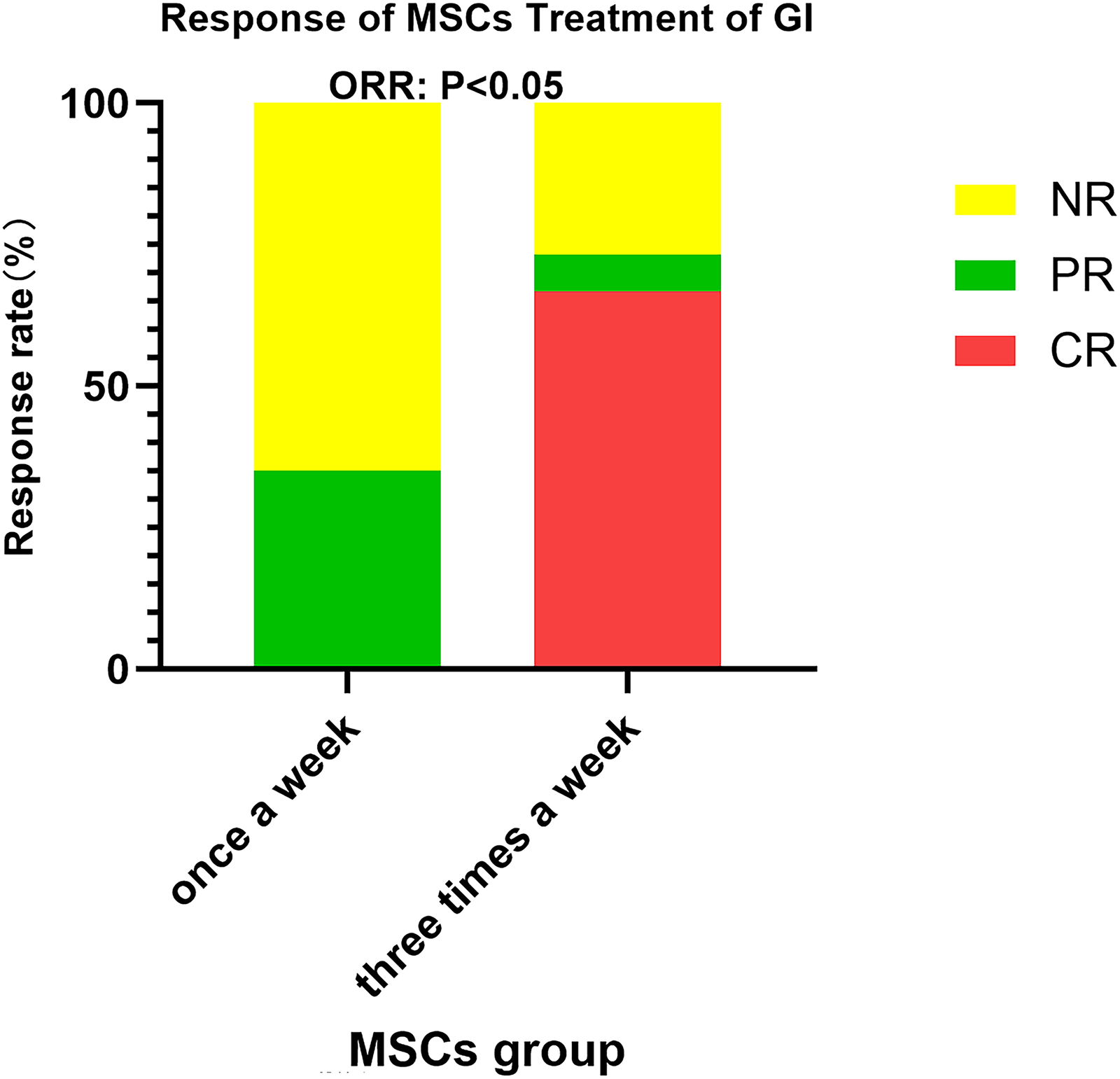
Response rates in aGVHD patients with gastrointestinal tract involvement after MSCs treatment. Patients were grouped by once a week (n = 20) or three times a week (n = 15) infusion regimens.
Lymphocyte subset and regulatory T-cell analysis
The changes in the median value and median time in lymphocyte subsets (CD3+CD8+, CD3+CD4+, and regulatory T cells) between the two groups are shown in Figure 3. At 8 weeks, the median decrease in CD3+CD8+ T cells was significantly lower in the three-times-a-week MSC group than in the weekly MSC treatment group (weekly vs. three times: 21.16% vs. 52.09%, P < 0.05; Fig. 3A). There was also a significant difference between the two groups in the median time for CD3+CD8+ T cells to drop to the lowest point, with a shorter time of decline in the three-times-a-week MSC therapy group (21 days vs. 10 days, P < 0.05).
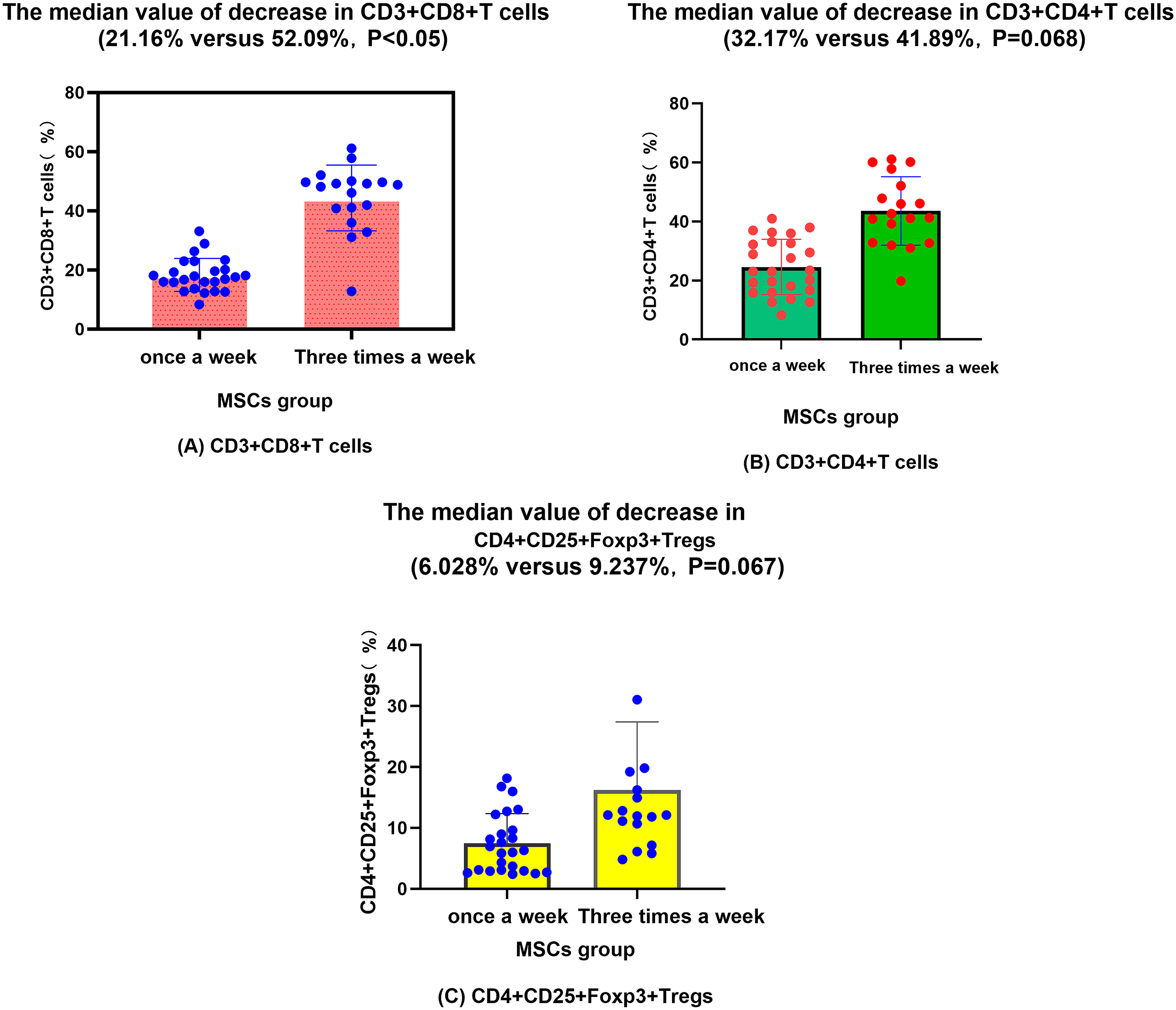
Dynamic changes in lymphocyte subsets following MSC infusions.
There was no significant difference in the median value or median time of decrease in the CD3+CD4+ T cell subgroup after different treatments (weekly vs. three times: 32.17% vs. 41.89%, P = 0.068; 16 days vs. 12 days, P = 0.089; Fig. 3B).
After analyzing the time and value of CD4+CD25+Foxp3+ Tregs, it was found that both treatments could increase the expression of regulatory cells. The median increase proportion of the once-a-week regimen was 6.028%, and the median increase proportion of the three-times-a-week regimen was 9.237% (Fig. 3C). However, there was also no significant difference in the median time of elevation or the median value to the highest point of CD4+CD25+Foxp3+ Tregs between the two groups (16 days vs. 12 days, P = 0.056).
Survival outcomes
The median follow-up time after HSCT and MSC treatment was 423 days (range = 103–1260) and 359 days (range = 91–1081), respectively. The 2-year probability of OS after MSC treatment was 47.4% and 78.1% for the once-a-week and three-times-a-week groups, respectively (P < 0.05; Fig. 4). Causes of death after MSC treatment included aGVHD progression (weekly group: n = 9; three times group: n = 3) and severe infection (weekly group: n = 4; three times group: n = 1; Table 3).
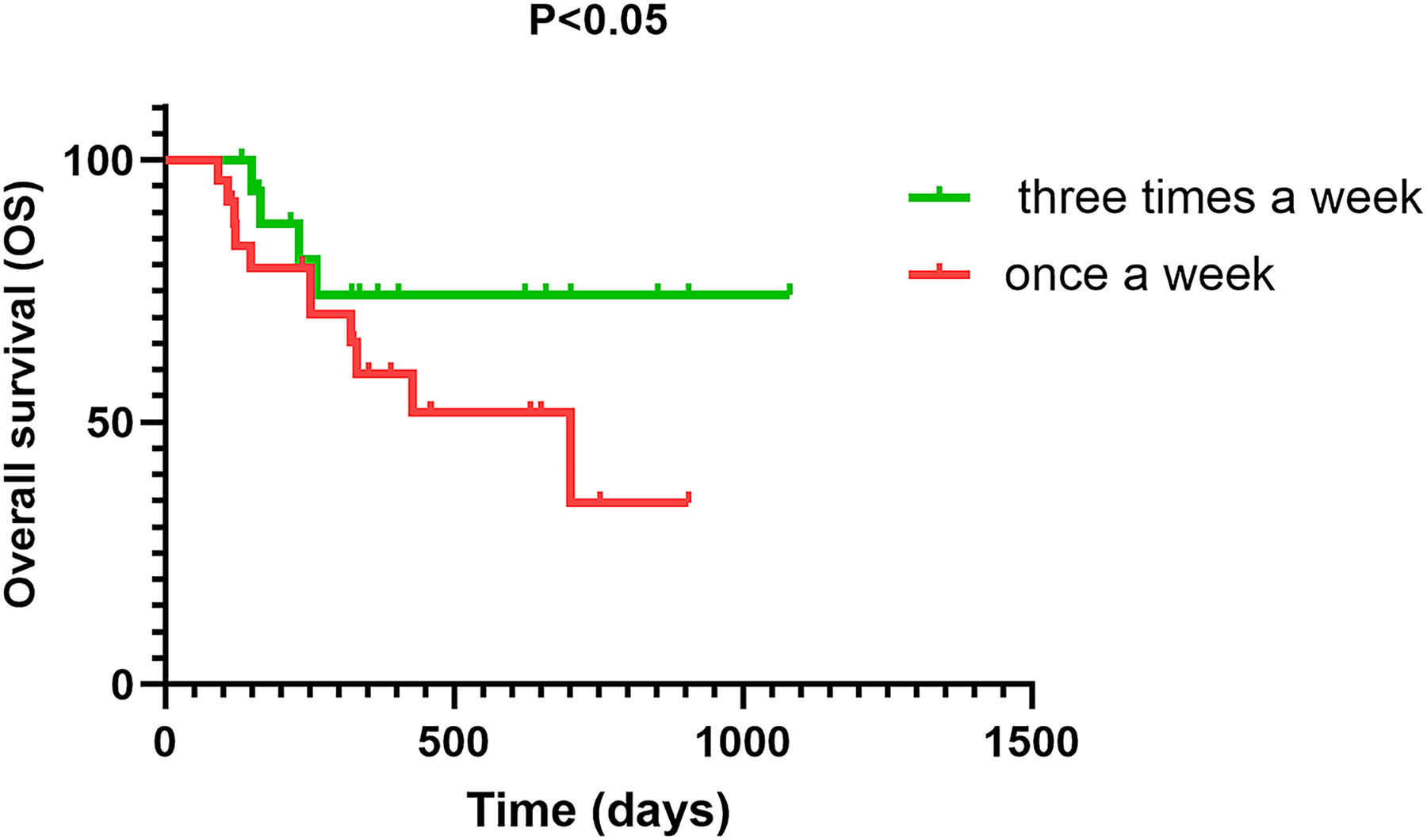
Overall survival after MSC treatment for severe acute GVHD. Kaplan–Meier curves compare patients receiving once a week (n = 25) versus three times a week (n = 18) infusion regimens.
Survival Outcomes and Causes of Death After Mesenchymal Stromal Cell Treatment
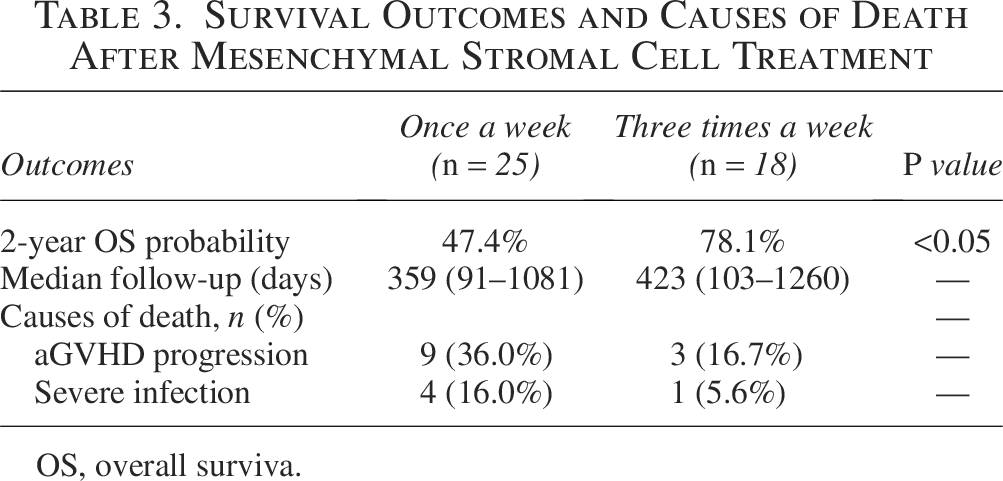
OS, overall surviva.
Multivariate analysis
To further account for baseline imbalances and potential confounding, multivariate models were performed for both treatment response and OS. In the logistic regression model for day 28 ORR, the three-times-weekly MSC regimen remained an independent predictor of treatment response after adjusting for GI involvement, GVHD grade, and age (OR = 2.50, 95% CI: 1.05–6.00, P < 0.05). GI involvement showed a trend toward reduced ORR (OR = 0.30, 95% CI: 0.05–1.25, P = 0.094), and higher GVHD grade (IV vs. III) also tended to be associated with lower response, although not statistically significant. Age was not associated with treatment response.
For OS, the Cox proportional hazards model demonstrated that the three-times-weekly regimen was independently associated with a significantly lower risk of death (HR = 0.25, 95% CI: 0.08–0.83, P < 0.05). GVHD grade IV showed a nonsignificant trend toward increased mortality risk (HR = 2.00, 95% CI: 0.85–4.70), and older age was marginally associated with worse OS (HR = 1.04 per year, 95% CI: 1.00–1.08, P = 0.050). GI involvement was excluded from the OS model due to complete separation (no deaths in the GI-negative subgroup), and donor type was excluded due to unstable estimates caused by sparse data (Supplementary Table S1).
Discussion
Effective control of severe GVHD is critical for improving outcomes in allogeneic stem cell transplantation. Current first- and second-line therapies show only about 50% efficacy, and the effectiveness of MSC infusion as a third-line treatment remains controversial.2,3 Key factors influencing MSC efficacy may include patient selection, timing of infusion, and frequency of administration across different centers.
In this study, MSC therapy was administered to patients with grade III–IV aGVHD or those progressing within 1 week after first- and second-line treatments. This retrospective analysis compared once-weekly versus three-times-weekly MSC infusion regimens.
Previous studies using once-weekly MSC infusion for SR-aGVHD reported ORRs around 57.1%–59.3% and CRs of 44.4%–50%.11,31 Similarly, our once-weekly group showed an ORR of 48.0% and a CR of 20.0%, consistent with prior data.
In contrast, the three-times-weekly regimen yielded significantly higher ORR (77.8% vs. 48.0%, P < 0.05) and CR (55.6% vs. 20.0%, P < 0.05) compared with the once-weekly group. Notably, for GI aGVHD—a common and severe form—the three-times-weekly regimen also showed superior efficacy (ORR: 73.3% vs. 35.0%, P < 0.05).
Survival analysis revealed that the three-times-weekly group had significantly better OS (78.1% vs. 47.4%, P < 0.05), with GVHD progression and severe infection being the main causes of death.
Our multivariate analyses further support the superiority of the three-times-weekly MSC regimen. After adjustment for key prognostic variables, increased infusion frequency remained significantly associated with both higher ORR and improved OS. Notably, the three-times-weekly schedule independently increased the odds of achieving an ORR by approximately 2.5-fold, consistent with the unadjusted comparisons. The protective effect on survival was also robust, demonstrating a 75% reduction in mortality risk compared with the once-weekly regimen.
GI involvement and higher GVHD grade showed expected trends toward poorer outcomes, although the small sample size limited statistical significance. The absence of deaths among patients without GI involvement led to complete separation in the Cox model, highlighting the profound prognostic impact of GI tract disease. Donor type was not retained in the multivariate models due to sparse-data bias and model instability, a common limitation in small retrospective cohorts.
Despite these constraints, the consistency between adjusted and unadjusted findings reinforces the likelihood that the superior outcomes observed with the three-times-weekly regimen represent a true therapeutic effect rather than confounding.
Basic research suggests that aGVHD is associated with decreased MSC numbers, even before clinical onset. 32 Ex vivo expansion may mitigate functional differences in MSCs and enhance their immunomodulatory capacity. 33 Additionally, MSC-mediated inhibition of T cell proliferation is dose-dependent, 18 supporting that more frequent infusions may improve efficacy by increasing MSC exposure.
Lymphocyte subset analysis showed that both regimens reduced CD3+CD8+ T cells, but the reduction was faster and greater with the three-times-weekly regimen (median 21.16% vs. 52.09%, P < 0.05; median time 21 vs. 10 days, P < 0.05). Both groups also exhibited decreased CD3+CD4+ T cells and increased regulatory T cells, although without significant differences in magnitude or timing. These findings align with previous reports,15,34–36 but the impact of infusion frequency on lymphocyte subsets has not been previously described.
The infusion frequency in this study changed over time, with the once-weekly regimen used initially and the thrice-weekly regimen adopted from September 2021 onward. This retrospective design inevitably introduces the possibility of era bias. Supportive care strategies, infection monitoring, and access to second-line GVHD agents have evolved over recent years, and these changes may have influenced patient outcomes independent of MSC frequency. However, it is notable that all patients included in this analysis met strict criteria for SR grade III–IV aGVHD and had already failed comparable first- and second-line treatments before starting MSC therapy. Additionally, baseline transplant characteristics, GVHD organ involvement patterns, performance status, and immunosuppressant exposure were balanced between groups. These factors help mitigate, although they cannot fully eliminate, the impact of temporal differences in clinical practice. Therefore, the improved outcomes associated with the thrice-weekly MSC regimen in this study should be interpreted cautiously and require confirmation in prospective studies where supportive care protocols can be standardized.
Several limitations of our study must be acknowledged. First, its retrospective nature and the chronological shift in treatment protocol introduce the potential for era bias. Differences in supportive care over time may have influenced outcomes. Second, the sample size is relatively small, limiting the power for extensive subgroup analyses.
A third important limitation of our study is that the infusion frequency and the cumulative MSC dose were inherently linked. Although our center followed a fixed-dose strategy for each infusion (1.0 × 106 MSCs/kg body weight), patients in the thrice-weekly group inevitably received a higher total MSC dose due to the greater number of infusions. Therefore, the present study cannot definitively determine whether the superior outcomes observed in the thrice-weekly group were driven by the increased frequency itself, the higher cumulative cell dose, or a synergistic effect of both factors. This confounding between dose and frequency should be interpreted with caution, and future prospective randomized studies are needed to independently control and evaluate total MSC dose and administration schedules to clarify their respective contributions to therapeutic efficacy. Finally, our immune monitoring was confined to peripheral blood; analysis of the bone marrow microenvironment could provide deeper insights.
Despite these limitations, our results compellingly suggest that increasing the frequency of MSC administration is a viable strategy to enhance its efficacy against severe aGVHD. The thrice-weekly regimen was well-tolerated in our cohort.
Ethical Approval
This study was approved by the Institutional Review Board of the Third Hospital of Shanxi Medical University/Shanxi Bethune Hospital (Approval No.: YXLL-2025-042). All procedures involving human participants were conducted in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments. Written informed consent was obtained from all patients or their legal guardians before MSC infusion and data collection.
Footnotes
Author Disclosure Statement
The authors declare no competing financial interests.
Funding Information
This work was supported by the Natural Science Foundation General Project of Shanxi Province (202203021211070) and Key Research and Development Projects of Shanxi Province (201803d31144).
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.